Introduction
In this chapter, endoscopic dacryocystorhinostomy (DCR) is performed using an up-biting and down-biting 4 mm Kerrison ronguer for the bony osteotomy. The medial portion of the lacrimal sac is also removed and sent for routine histopathology. For indications, preoperative evaluation, and complications refer to Chapter 53 .
Surgical Technique
Injection of local anesthetic
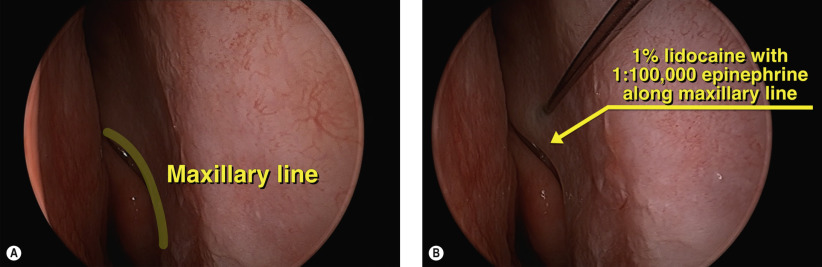
Preoperative nasal decongestion is maximized as described in Chapter 53 . Figure 55.1A shows the maxillary line, which is the mucosal projection of the maxillary–lacrimal suture line comprising the lacrimal crest. Local anesthetic containing 1% lidocaine and 1 : 100,000 epinephrine is injected into the nasal mucosa overlying the lacrimal sac at the maxillary line ( Figure 55.1B ).
Creation of osteotomy
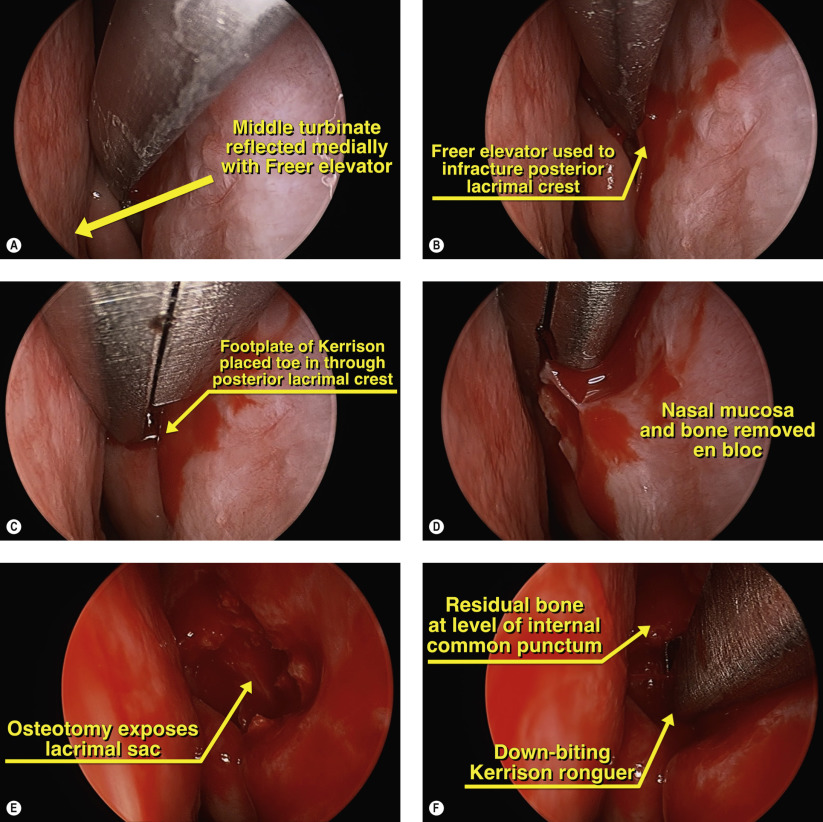
A Freer elevator is used to reflect the medial turbinate medially ( Figure 55.2A ). This creates room for the Kerrison ronguer to later engage the lacrimal fossa bone. The Freer elevator is then used to infracture the posterior lacrimal crest posterior to the maxillary line ( Figure 55.2B ). A 4 mm Kerrison ronguer is used to medially reflect the middle turbinate and the footplate is placed in a “toe-in” position through the infractured lacrimal bone ( Figure 55.2C ). Nasal mucosa and bone are removed en-bloc at the initial osteotomy site ( Figure 55.2D ). Care should be taken to avoid traumatizing the nasal septum or surrounding mucosa during all endonasal manipulations to minimize bleeding and postoperative scarring. External compression over the skin helps to identify the lacrimal sac ( Figure 55.2E ). The lacrimal sac is kept intact while bone is progressively removed superiorly. At the most superior level of the lacrimal sac, a down-biting 4 mm Kerrison ronguer can be used to remove this difficult-to-remove bone ( Figure 55.2F ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


