| Symptomatic epiphora secondary to canalicular obstruction or canalicular atresia |
| Intractable epiphora in the setting of failed prior lacrimal bypass procedures |
| Intractable epiphora in the setting of facial paralysis and poor lacrimal pump function |
| Probing and irrigation of canaliculi to determine location of obstruction |
| Ocular surface examination including caruncle and plica semilunaris to determine optimal location for Jones tube |
| Nasal exam to rule out intranasal pathology and septal deviation that may interfere with Jones tube placement |
| Assess orbicularis strength and cranial nerve (CN) VII function |
| Assess eyelid laxity |
| Inspection of puncta to identify stenosis or atresia |
Introduction
Conjunctivodacryocystorhinostomy (CDCR) with Jones tube is an operation performed for symptomatic epiphora secondary to canalicular obstruction untreatable by other means. It should not be undertaken lightly and must be viewed as a procedure that requires long-term follow-up and maintenance. CDCR can also be useful in some situations of multiple prior failed lacrimal bypass procedures and intractable epiphora secondary to facial nerve (CN VII) palsy. In cases of symptomatic isolated canalicular obstruction, a thorough discussion should be undertaken with the patient of other options available, such as canalicular trephination and silicone stent placement prior to proceeding with CDCR.
CDCR with placement of the Jones tube can be performed either through an external or endoscopic approach. Our preference is for the endoscopic approach, which provides direct intranasal visualization during the operation. Preoperative evaluation should include probing of the canaliculi to determine the location of the obstruction, examination of the ocular surface, and intranasal exam. For preoperative considerations for endoscopic surgery, please see Chapter 53 .
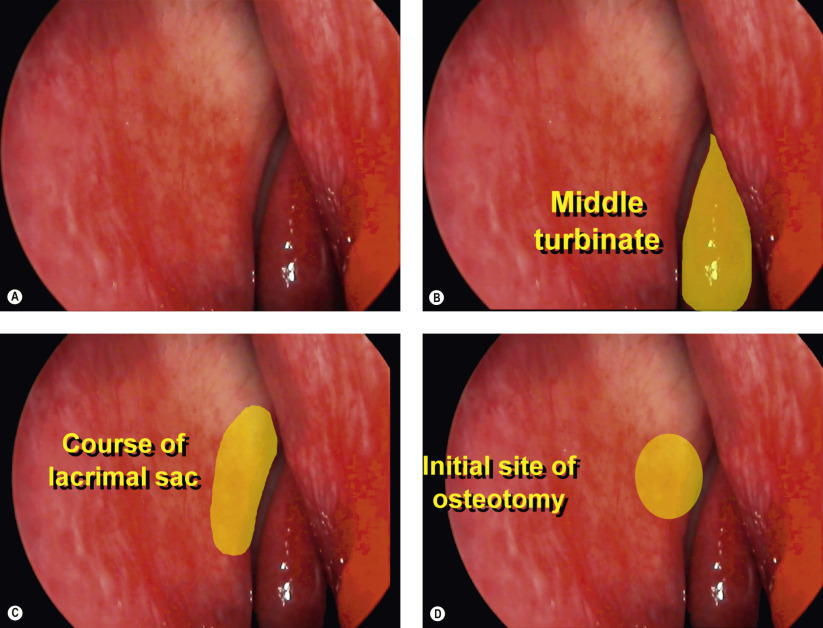
For optimum function, placement of the Jones tube should be as vertically oriented as possible. The location on the ocular surface should be at the junction of the plica semilunaris and caruncle. Although varying versions of the original glass tube have been fabricated, we prefer the straight Jones tube with 4.0 mm diameter flange and fixation hole. Fixation of the tube is performed with an 8-0 Vicryl suture to the surrounding conjunctiva. Intranasal location of the Jones tube should be just anterior and inferior to the origin of the middle turbinate. The tube should not abut the nasal septum or middle turbinate. Occasionally partial middle turbinectomy of the anterior tip is required to provide a clear unobstructed pathway for the tube.
Patients should be advised that extrusions and clogging of the tube can occur and regular maintenance is required. Daily “sniffing” through the tube with closed nostrils helps to clear the tube and ensure patency. Periodic removal with cleaning and replacement of the tube may be required. A porous polyethylene-coated tube can be used in cases of repeated extrusion. Despite complications and continued symptoms that may occur in up to 25% of patients in some published series, many patients experience complete relief of epiphora.
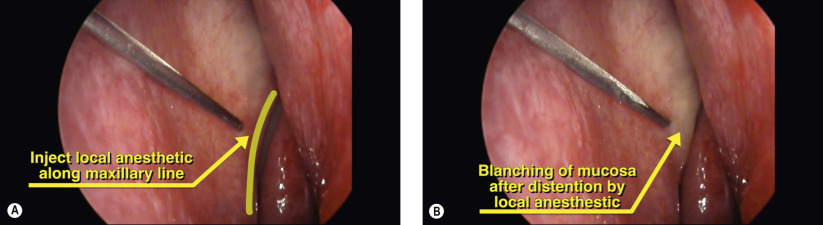
Surgical Technique