Endocrine disorders present with a range of findings that may affect any layer of the skin. The associated skin changes can lead the astute physician to suspect the underlying disorder and order appropriate confirmatory tests.
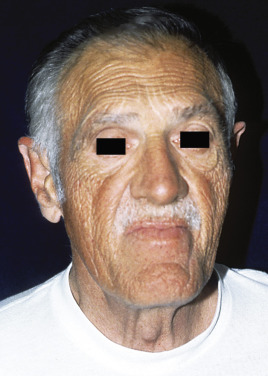
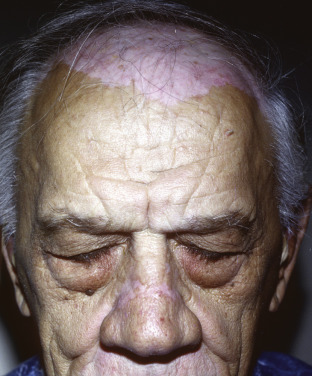
Excess growth hormone before closure of the epiphyses leads to gigantism, whereas in adults it leads to acromegaly with hypertrophy of the chin, nose, and supraorbital ridges and thickening and wrinkling of the forehead, sometimes accompanied by cutis verticis gyrata. The distal digits are expanded. Addison disease leads to generalized hyperpigmentation as well as orolabial pigmented macules and nail streaks, whereas Cushing disease results in moon facies, fat redistribution giving rise to a buffalo hump, and hirsutism. An appreciation of the range of clinical findings in these conditions can lead to the early diagnosis of systemic disease.
Thyroid disease can present with subtle edema, most prominent around the eyes, in the case of hypothyroid myxedema, or with pebbly thickening of the skin of the shins and dorsal foot in Graves disease–associated pretibial myxedema. Necrobiosis lipoidica presents as atrophic, orange-to-yellow plaques with prominent vascularity and occasional ulceration. The plaques often involve the shins. Diabetes can cause acanthosis nigricans, a velvety thickening and darkening of the skin, noted most prominently over the flexures.