This article reports on the early experience with the 1440-nm wavelength, using a specially designed side-firing fiber, in a four-step approach, primarily to the lower third of the midface and neck. The author presents the clinical protocol, procedure steps, outcomes, and adverse events of use of the laser. Outcomes are described at 3 months, 6 months, and 18 months.
- •
Use of the 1440-nm wavelength has been shown to significantly increase skin thickness and elasticity 6 to 18 months from baseline measurements in the lower third of face and neck.
- •
The procedure was not recommended for correction of strong and separated bands of the platysma muscle.
- •
The 1440-nm wavelength produced the highest fat and dermal tissue ablation efficiency, with minimal localization of heat over depth.
Introduction
The recent adoption of the internal 1440-nm pulsed laser has advanced the safety, efficacy, and versatility of laser lipolysis and tissue tightening in face and body rejuvenation. The longer wavelength provides increased localized photothermal and vaporizing effects in front of the fiber on fatty tissue and collagen fibers (water), achieving 20 times more absorption in adipose tissue than the 1064-nm/1320-nm and 40 times more absorption than 924-nm/980-nm wavelengths. In recent clinical studies, use of the 1440-nm wavelength has been shown to significantly increase skin thickness and elasticity 6 to 18 months from baseline measurements. This article reports the early experience with the 1440-nm wavelength, using a specially designed side-firing fiber in a four-step approach primarily to the lower third of the midface and neck.
Laser device system
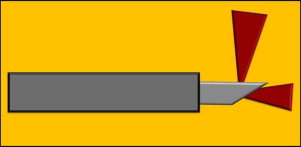
The laser workstation delivered the 1440-nm wavelength pulsed laser from a 800-μm side-firing fiber that was enclosed and protruded 2 mm from the tip of a temperature-sensing 1.2-mm cannula. The side-firing fiber distributed about half of its energy perpendicular to the fiber axis and the other half transmitted along the fiber axis ( Fig. 1 ). Chevron markings on the handpiece designated the direction of the laser emission perpendicular to the fiber axis. This emission design permitted a more targeted delivery of laser energy to the structures of interest, which included in turn fat, fibrofascial layer of the muscle, and the skin-dermis. During treatment of the fatty tissue and deeper fibrofascial muscle layer, the temperature-sensing cannula acted as a thermal switch by sensing temperatures set between 45°C and 47°C at the immediate laser-delivery point. When the recommended target temperature was attained, an audible signal was triggered. If the surrounding tissue temperatures exceeded the preset threshold level, a beeping audible signal warned the operator to move to another area to reduce excessive thermal injury. Maintenance of this thermal window distributed laser heat energy evenly to melt fatty tissue and denature collagen in a safe manner. When the laser fiber treated shallow subdermal tissue (5 mm below the dermis), the temperature-sensing cannula was programmed at the same 45°C to 47°C temperature range, which in turn produced a superficial skin temperature between 38°C and 42°C, which was optimal for collagen denaturation and later delayed tissue tightening. An infrared thermal camera (Therma View EHS, FLIR Systems Inc., Niceville, FL) obtained continuous skin temperatures between 38°C and 42°C and ensured a uniform, real-time deliverance of heat by depiction of a confluent orange-red coloration within each treatment site. A hand-held infrared noncontact thermometer (MiniTemp MT6; Raytek Corporation, Santa Cruz, CA) was used simultaneously with the thermal camera to measure rapidly surface skin temperatures by spot-checking to ensure skin safety.
Laser device system
The laser workstation delivered the 1440-nm wavelength pulsed laser from a 800-μm side-firing fiber that was enclosed and protruded 2 mm from the tip of a temperature-sensing 1.2-mm cannula. The side-firing fiber distributed about half of its energy perpendicular to the fiber axis and the other half transmitted along the fiber axis ( Fig. 1 ). Chevron markings on the handpiece designated the direction of the laser emission perpendicular to the fiber axis. This emission design permitted a more targeted delivery of laser energy to the structures of interest, which included in turn fat, fibrofascial layer of the muscle, and the skin-dermis. During treatment of the fatty tissue and deeper fibrofascial muscle layer, the temperature-sensing cannula acted as a thermal switch by sensing temperatures set between 45°C and 47°C at the immediate laser-delivery point. When the recommended target temperature was attained, an audible signal was triggered. If the surrounding tissue temperatures exceeded the preset threshold level, a beeping audible signal warned the operator to move to another area to reduce excessive thermal injury. Maintenance of this thermal window distributed laser heat energy evenly to melt fatty tissue and denature collagen in a safe manner. When the laser fiber treated shallow subdermal tissue (5 mm below the dermis), the temperature-sensing cannula was programmed at the same 45°C to 47°C temperature range, which in turn produced a superficial skin temperature between 38°C and 42°C, which was optimal for collagen denaturation and later delayed tissue tightening. An infrared thermal camera (Therma View EHS, FLIR Systems Inc., Niceville, FL) obtained continuous skin temperatures between 38°C and 42°C and ensured a uniform, real-time deliverance of heat by depiction of a confluent orange-red coloration within each treatment site. A hand-held infrared noncontact thermometer (MiniTemp MT6; Raytek Corporation, Santa Cruz, CA) was used simultaneously with the thermal camera to measure rapidly surface skin temperatures by spot-checking to ensure skin safety.
Clinical protocol
Patients were selected for isolated mild to moderate accumulations of fat to the lower third of the face and neck and mild to moderate tissue laxity of the muscle and skin. After review of their medical history, subjects were consented for their office procedure and the usage of local anesthesia. A preoperative physical examination, blood chemistry panels, and electrocardiogram were required from each patient within 2 days of surgery. Before surgery, patients were weighed, photographed by standardized digital imaging, and prescribed a pain medication and antibiotic. In four randomized patients, skin thickness was measured at the same spot three times with a 20-MHz high-frequency ultrasound probe (DermaScan C, Cortex Technology, Hadsund, Denmark) at baseline and 6 months. In one patient, biopsies from opposing sides of the treated neck below the ear lobule were submitted for hematoxylin and eosin staining for assessment of tissues at completion of procedure.
The procedure was not recommended for correction of strong and separated bands of the platysma muscle. Exclusion criteria included pregnancy, uncontrolled diabetes mellitus, collagen disorders, significant cardiovascular diseases, bleeding disorders, smokers, and previous surgical procedures within a year to treatment sites. Aesthetic treatment efficacy from baseline to 6 months was rated by two independent investigators using the Investigator Global Aesthetic Improvement Scale from standardized photographs (0 = no change, 1 = mild improvement, 2 = moderate improvement, and 3 = significant improvement). Patients used a Subject Global Aesthetic Improvement Scale from their baseline to 6 months photographs (0 = no change, 1 = mild improvement, 2 = moderate improvement, and 3 = significant improvement).
Procedure
The procedure was as follows:
- •
In the sitting position, the patient’s treatment sites were marked with one 3 × 5 cm sector lateral to each marionette line and two 5 × 5 cm sectors on each side of the midline of the neck ( Fig. 2 ).
Fig. 2
( A–C ) Presurgical markings of the six sectors are outlined with the patient in the sitting position. Sectors 1 and 6 were rectangles (3 × 5 cm) in each lower third of face; sectors 2, 3, 4, and 5 were squares (5 × 5 cm) in the neck.
- •
Subjects received an oral sedative 30 minutes before surgery.
- •
After skin preparation with povidine-iodine antiseptic washes, a 1-cm incision was made behind each ear lobe and also at the transverse submental crease line.
- •
Twenty to thirty milliliters of tumescent anesthesia mixture (50 mL of 0.5% lidocaine, 1 mg epinephrine per liter of warm saline, and 20 mL of 8.4% sodium bicarbonate) was infused into each sector through the access incisions at the deep and superficial levels of subcutaneous fat.
- •
After 20 to 30 minutes, the 800-μm side-firing fiber, enclosed in its temperature sensing cannula, was inserted through one of the three access incisions.
- •
All procedures were performed awake with oximetry and electrocardiogram monitoring without need for external oxygen administration.
- •
The red-aiming beam from a diode 630-nm laser source visualized the tip of the fiber during the three steps involving the laser with the fiber tip either in the down or up direction. The intensity and distribution of the red-aiming beam during lasering in a darkened or dimmed room guided the surgeon to position optimally the laser’s energy and direction to the mid-level of fat, over the platysma muscle and under the skin-dermis.
Standard laser guidelines, as outlined by the American National Standard for the Safe Use of Lasers in Health Care Facilities, included the use of protective goggles for the patient and staff during phases of laser treatments.
In the first step, the fiber was inserted through one of the access incisions in the down position ( Fig. 3 ). Once in place, the activated cannula-fiber was moved back and forth in a fanlike pattern in the mid-to-deep levels of the subcutaneous fat in each sector. Two sectors on one-half of the neck were treated at a time to optimize laser delivery. The power and pulse frequency settings were set between 6 and 10 W and 25 H, respectively. The endpoints of treatment were determined when the total number of joules delivered ranged between 500 and 700 J/sector, and limited or no tissue resistance to the fiber’s passes while the temperature-sensitive cannula maintained a 45°C to 47°C threshold. External skin temperature monitoring was performed with the thermal infrared imaging camera and the hand-held infrared noncontact thermometer.
In the second step, liposuction with a 1.2-mm round two-hole cannula to the lower third of the face and with a 3.2-mm two-hole flat cannula to the neck evacuated the liquefied fat, tumescent solution, and tissue debris under a low vacuum pressure of 350 to 500 mm Hg in the six sectors. Liposuction permitted immediate contour assessment and created an environment with less debris that facilitated more rapid elevation of threshold subdermal temperatures during the subsequent shallow lasering.
In the third step, the activated fiber-cannula was inserted in the down direction ( Fig. 4 ), reciprocated in a fanlike motion, and deposited a total of 200 to 300 J on the fibrofascial surface of the platysma muscle in each sector. It was anticipated that the denatured collagen fibers would eventually reorganize and tightened the muscle unit.
Related posts:
 Are We Witnessing the Emergence of a Superspecialty?
Are We Witnessing the Emergence of a Superspecialty?
 Applications of Biomaterials in Plastic Surgery
Applications of Biomaterials in Plastic Surgery
 Impact of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Impact of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


