Introduction
A variety of traumatic ear defects are observed after amputation, be they partial, subtotal or total, all of which require complex contour reconstruction.
There are multiple causes of ear amputations and this summary chapter aims to define some principles and guidelines that permit a precise surgical management plan.
Initial Assessment Concerning a Posttraumatic Amputation
Mechanism of Ear Amputation
Clean Amputations
These are usually secondary to trauma involving a knife, surgical resection or sharp bites (animals or human). Primary treatment consists of debridement and suturing of the edges of the wound.
If we exclude surgical amputation for cutaneous malignancy, it is tempting to replant the amputated segment of ear. Many different techniques have been proposed to ensure success of such replantation (burying, fibrocartilage fenestration, cartilage storage, and secondary replantation). Whatever the degree of success of such a surgical approach, the final result will be disappointing. Even though it may be difficult to make the decision not to attempt replantation and sacrifice the amputated ear segment, this will preserve the skin potential for a superior secondary reconstruction.
Replantation should only be considered when vascular anastomosis is possible and reliable.
Crush Injury
These injuries occur after a fall, road traffic accident, blunt trauma ,and violent compression. In such circumstances the ear defect is generally only part of complex injury involving the surrounding soft tissue.
Burn Injury
Thermal, chemical or electrical injury are frequent causes of traumatic ear defects. Both ears are frequently affected and the burn area extends around the auricular area. Besides the zone directly injured by the burn, a secondary chondritis often results in severe resorption of the fibrocartilage. When limited to the ear, the defect usually affects the scapha and helix, but often retroauricular skin and the scalp is affected with scars and alopecia.
Burn patients are generally managed in a burns unit where initial stabilization and grafting is performed. Reconstruction of the ear is a last step of management. These patients, who have undergone multiple surgical procedures, may opt not to have an ear reconstruction. In some cases, an ear prosthesis is indicated.
Analysis of the Defect
A precise analysis of the defect is critical in all reconstructive efforts. The missing contours must be appreciated and reconstructed in all dimensions.
To correctly appreciate the defect it is essential to draw the normal ear on a transparent template and place it on the injured ear to appreciate the missing contours needing reconstruction. Skin alone is not adequate to reconstruct the contours of the ear and depending upon the size of the defect either fibrocartilage or rib cartilage is required as part of the reconstruction.
Analysis of the Skin Potential
The specific problem encountered in cases of posttraumatic amputation is the presence of scars. It is essential to analyse their location and the skin availability to cover the reconstructed cartilage construct. The following three factors need consideration:
- 1.
The quality and quantity of skin in the auricular area must be appreciated. The presence of lax and scarless retroauricular skin provides the best conditions for coverage of the cartilage framework.
- 2.
Scars. After inspection of scars, a surgical approach is chosen to minimize the use of new scars and ensure vascularity of the skin to cover the cartilage construct.
- 3.
Deficit of skin. In cases where there is no skin available in the auricular area, surrounding fascia (temporoparietal or occipital) or the use of skin expansion will have to be considered to cover the cartilage framework.
Reconstruction in Partial Amputations
Partial traumatic defects of the ear are always located along the free border of the ear.
In this discussion we will exclude defects of the helix that can be closed directly or using skin flaps or chondrocutaneous flaps. The Antia–Buch flap can be used for small defects but its principle of moving the helix after a scaphoid resection always reduces the size of the ear.
In partial amputation skin availability is usually adequate and the main concern is to choose the best support to reproduce the missing cartilage contours. Either fibrocartilage or rib cartilage may be used. It is essential to draw the normal ear on a template, and then transpose the template on the affected ear to work out what is missing and what contours need reconstructing.
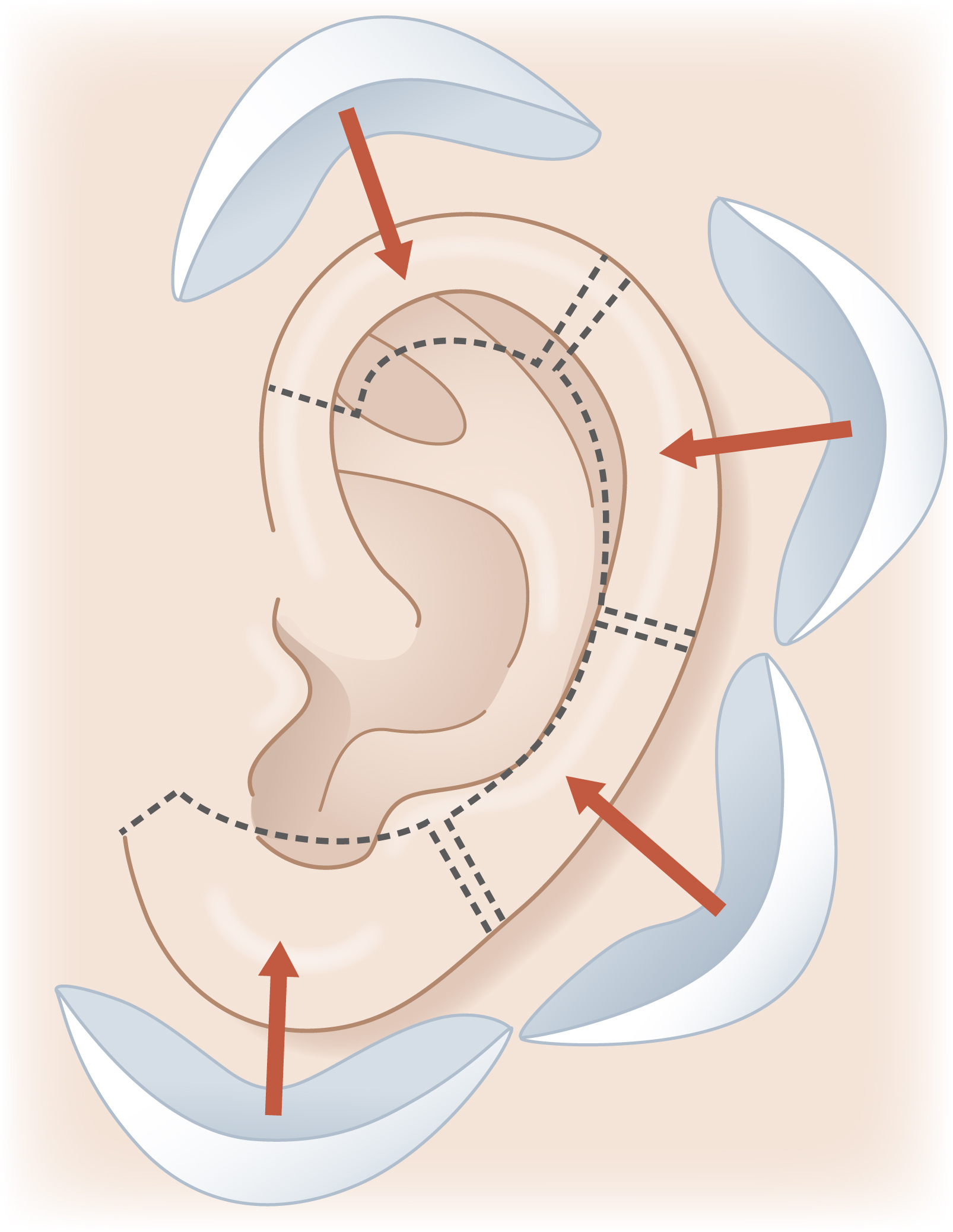
The rule is that fibrocartilage can only be used to reconstruct a partial defect after trauma if it is no more than a quarter of the border of the ear and includes no more than two adjacent planes. Harvesting all of the concha can only reproduce two adjacent planes and just a quarter of the ear. If the defect is less than a quarter but includes three planes, then rib cartilage should be harvested to correctly reproduce the missing contours ( Fig. 32.1 ).
Reconstruction Using Fibrocartilage
Harvesting the Fibrocartilage Graft
The concha is the best donor site considering its size and the fact that it will not be visible if harvested correctly. The entire concha has to be harvested taking care to preserve the root of the helix and enough posterior wall of the concha.
Depending on the case, it can be harvested through an anterior or posterior approach from the ipsi- or contralateral ear.
The choice concerning the skin approach (anterior or posterior) depends on the defect and the skin vascularity. The choice concerning the harvesting on the ipsi- or contralateral side may be discussed with the patient, who sometimes is reluctant to have surgery performed on the normal ear.
Depending on the location of the defect and the skin potential, the reconstruction will be performed in one or two stages.
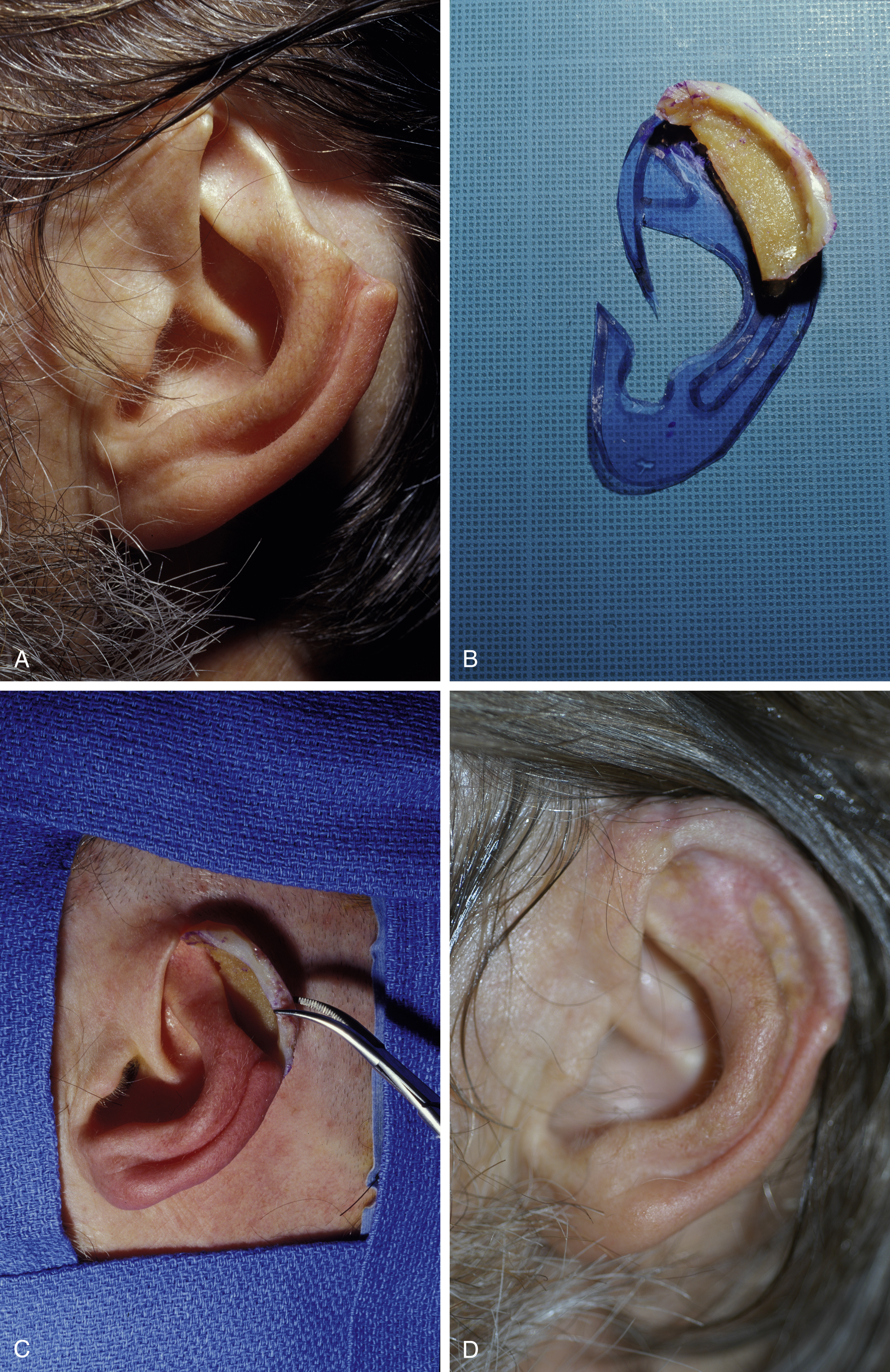
Case 1 ( Fig. 32.2 )
Reconstruction in one stage using ipsilateral conchal graft. The defect is secondary to chondritis after trauma. It is a quarter of the contour of the ear and no more than two adjacent planes .
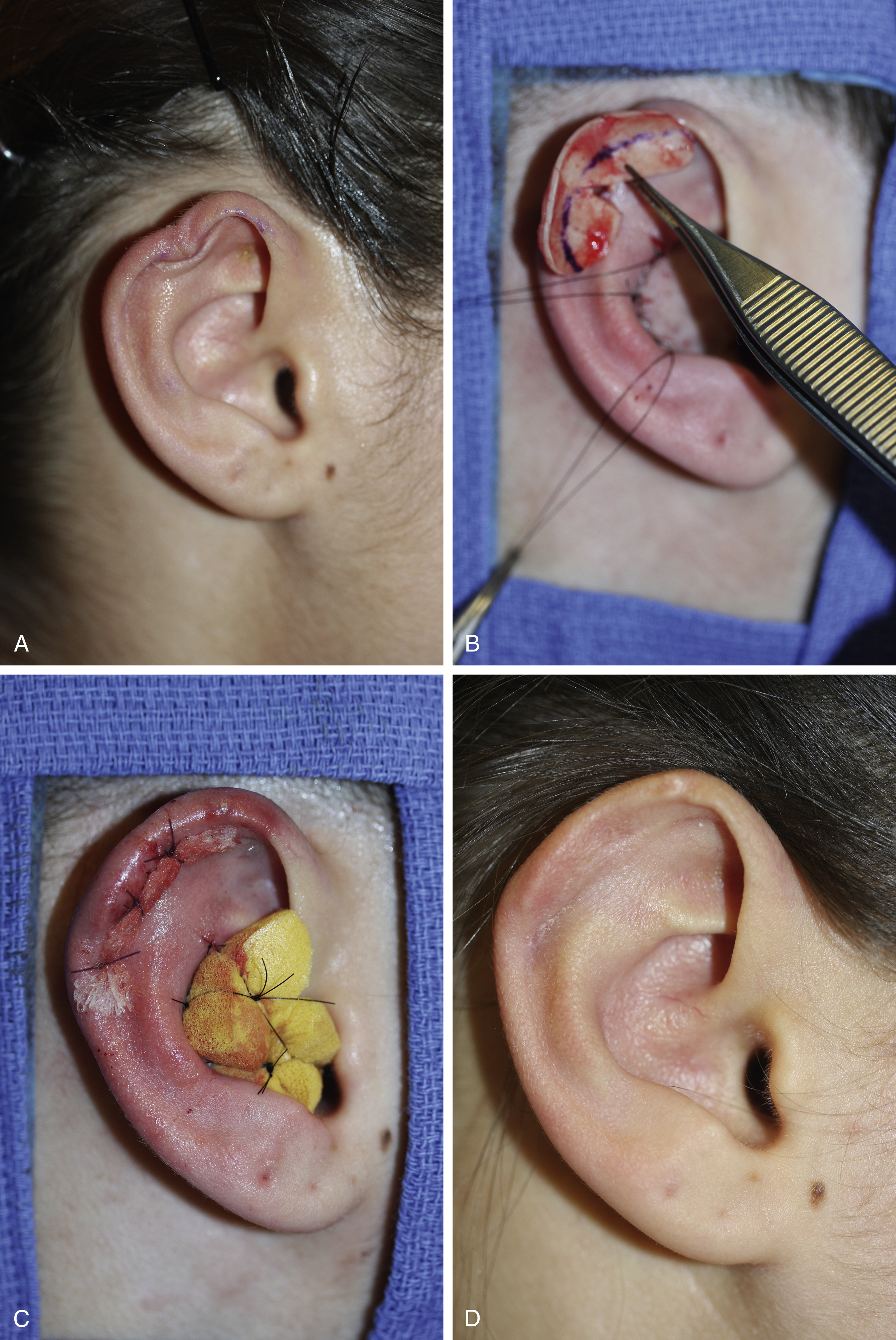
Case 2 ( Fig. 32.3 )
The defect being a quarter and no more than two planes, the reconstruction was performed using a contralateral conchal graft covered with retroauricular skin. Creation of the retroauricular sulcus behind the reconstructed part of the ear will be performed in a second stage. Elevation of the ear is performed respecting the soft tissues behind the ear, to cover the area with a small full-thickness skin graft harvested from the opposite retroauricular sulcus .

Reconstruction Using Costal Cartilage
There is an abundant amount of cartilage when harvesting from the thorax but when harvesting for reconstruction of partial defects, only one segment of cartilage is required. In such situations the scar on the thorax will be short.
Harvesting cartilage is a routine procedure with minimal risk. Pain is avoided by injecting local anesthetic into the muscles.
Using only a skin flap to reconstruct a partial amputation located on the periphery of the ear cannot reproduce complex contours and will give a poor result.
It is important to differentiate cases were the entire antihelix has been preserved from cases where part of it is missing, particularly the posterior wall of the concha. If part of the antihelix is missing it has to be reconstructed respecting the anatomical unit of the antihelix and the base that supports it.
Cases with Normal Antihelix
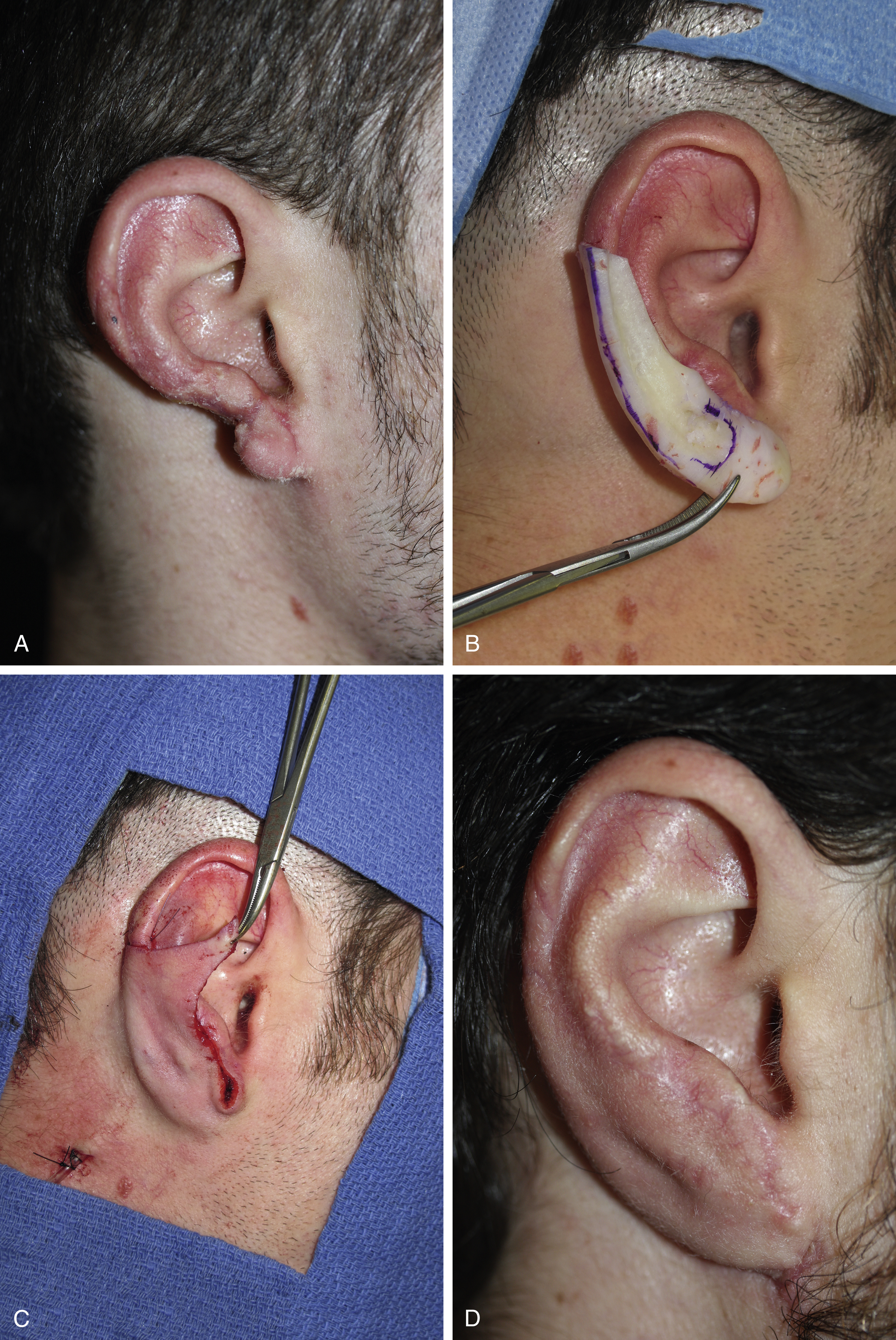
Case 3 ( Fig. 32.4 )
Clean amputation with a defect that is no more than two adjacent planes but more than a quarter of the ear or the border of the ear requiring the use of rib cartilage support. The reconstruction will be performed in one stage as there is enough retroauricular skin to cover the narrow cartilaginous graft .

Case 4 ( Fig. 32.5 )
The amputation is secondary to a human bite. An unsuccessful replantation has left a defect involving half of the inferior border of the ear, including the lobule. The reconstruction was performed in two stages with a very good result. The former scar was used to prepare the flap to cover the cartilage framework during the first stage. Advancement of the retroauricular skin and grafting the posterior surface of the reconstructed ear was done 4 months later during the second stage .
Case 5 ( Fig. 32.6 )
Using a rib cartilage graft on a 60-year-old patient is possible as there is no correlation between the age and ossification. Texture and color of the cartilage will just be different. The rib segments are thicker so the scapha and helix can be sculpted in one segment. Elevation of the reconstructed upper third of the ear will be performed 4 months later.