Introduction
Definition
Dupuytren disease (DD) is a benign fibromatosis of the palmar fascias in which nodules and skin pits in the distal palm are usually the first signs. As it progresses, cords are formed which in time may contract limiting extension of the fingers and causing webspace contractures. The disease usually starts in the ring finger and little finger ray, but may affect any ray in a variable pattern. The same is true for the age at which the first symptoms occur. In the majority of cases the disease emerges in people of over 50 years of age. In the younger age groups, males are more affected than females. Systematic meta-analysis of the published work on prevalence has revealed it to range from 0.6 to 31.6%. The disease may affect all races, although prevalence of DD has not been studied extensively in other than Caucasian races (only incidence reports).
Similar fibromatoses may affect the fascias in the instep area of the foot (Ledderhose disease (LD)), the penis (Peyronie disease (PD)), and the knuckles of the finger joints (Garrod pads). LD can cause pain during walking. Toe contractures are only sporadically seen. In PD contraction of plaques formed within the tunica albuginea may cause penile curvature during erection, sometimes hampering sexual intercourse.
Impact of DD and its Reflection in Patient-Rated Outcome Measures
The impact of DD on the patient varies with the demands the patient has. Awkwardness and functional incapacity are usually direct consequences of increasing contracture, especially when the total extension deficit of a finger exceeds 90 degrees, turning the finger into a hook that inadvertently catches objects, that cannot be easily released. Specific common complaints may be difficulty to put on gloves or getting one’s hand into a pocket, eye poking with the bent fingers during facial wash and embarrassment in social hand shaking. Dupuytren contractures may interfere with various job-specific tasks and functionally impair in numerous ways. Primary DD in general does not limit finger flexion.
It is not easy to quantify the disabilities, since most general upper limb impairment scores do not reflect the specific impairment of the contractures, nor their effect on performance of activities or quality of life. There are a few disease-specific questionnaires, but they have been found to have their limitations in use too.
Variable Disease Course of DD
In the majority of DD cases contractures do not develop and it is good to realize that in clinics a subset of the affected population is seen; those who become patients do so mostly because they have developed contractures. Within this group, a further subset of patients can be distinguished that challenges surgeons the most, due to an aggressive disease course (Dupuytren diathesis): in these patients, whose family members often also are affected, the disease typically starts at a young age, affects both hands, also involves the radial side of the hand and is commonly associated with fibromatoses such as knuckle pads, PD and LD. Since these patients develop contractures earlier in life, treatment is often needed at a younger age. Because the disease activity is higher, they often develop (early) recurrences – especially of the little finger – which may demand additional and repeated surgery, which ultimately may inflict damage to neurovascular (NV) bundles and even gangrene.
In the symptomatic population in general, DD is often found to recur or progress and should therefore be regarded as a chronic disease that at present cannot be cured. Therefore, a thoughtful individually tailored treatment strategy is indispensable. On one hand, the aim is to correct the disabling contractures with as minimally invasive treatment options as possible. On the other hand, more aggressive measures sometimes need to be considered in those cases, where recurrence is almost inevitable. This chapter aims to summarize the current knowledge of the various aspects of this disease and give some guidelines for treatment.
Surgical Anatomy of the Palmar Fascia and Changes Found in DD
McFarlane and McGrouther have to be credited for pointing out the anatomical basis of most of the fascial structures relevant for DD and for relating them to what may be expected at surgery. ,
Palmar and Digital Fascias
In the palm the normal fascial structures form a three-dimensional network consisting of longitudinally, transversely, and sagittally running fibers. The longitudinal fibers are organized in a triangle and form the palmar aponeurosis. In this triangle, pretendinous and prelumbrical bands can be distinguished, the former being more condensed than the latter. They all pass superficial to the transverse ligament of the palmar aponeurosis (TLPA), which is situated at a line joining the proximal and distal palmar crease. The ulnar border of the TLPA forms a crossroad with fibers of the hypothenar fascia and the radial border is continuous with the proximal commissural band, which runs through the first webspace and ends in the thenar fascia at the level of the first metacarpophalangeal joint. Just beyond TLPA, the pretendinous bands divide into three layers ( Fig. 55.1 ). Layer 1 is the most superficial layer, which has its insertion in either the skin of the distal palm or the proximal phalanx. Layer 2 fibers form the so-called “spiral band,” since it spirals around the NV bundle on its course towards the finger. This band is present on both sides in all long fingers, except for the ulnar side of the little finger. Layer 3 is the deepest layer of fibers, which takes a sagittal course into the hand on both sides of the flexor tendon sheath to insert on either side of the corresponding metacarpophalangeal (MCP) joint.
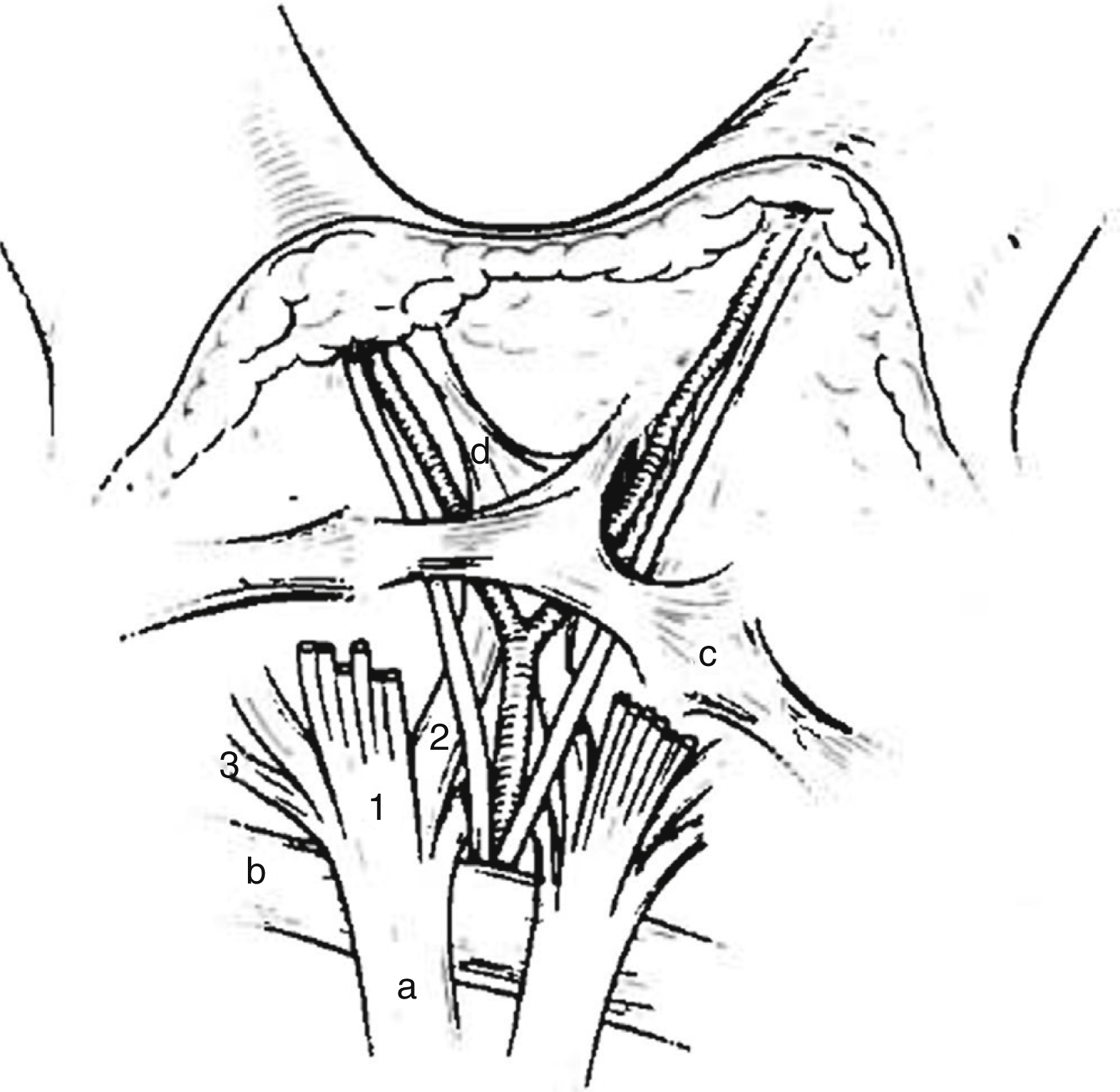
Another important transverse fascial structure is the natatory ligament (NL). This ligament lies just underneath the skin in the distal palm and is situated superficial to the NV bundles (see Fig. 55.1 ). On its ulnar end it is continuous with the hypothenar fascia, and on the radial side with the distal commissural band. NL has attachments to the flexor tendon sheet, lines the webs, and has extensions along the lateral sides of the digits. It also blends with fibers from the spiral band and is continuous with the lateral digital sheet. It is important not only because it may be affected, but also because its proximal border defines the place where a spiral nerve superficially crosses a spiral cord, making it vulnerable during surgery.
The vertical or sagittal ligaments in the palm worth mentioning are the septa of Legueu and Juvara that are usually just as wide as TLPA and, except in the thumb, connect the longitudinal fibers at the level of the TLPA, and TLPA itself with the deep transverse palmar ligament that runs between the volar plates of all MCP joints. On cross-section, the TLPA and the deep transverse ligament, together with the ligaments of Legueu and Juvara, form nine boxes, which on an alternating basis hold either the lumbrical muscle and NV bundles, or the flexor tendons of each ray. Much smaller vertical fibers are dispersed throughout the palmar aponeurosis and anchor it to the overlying skin.
The digital fascial structures relevant to Dupuytren disease bear the names of Cleland and Grayson. Their detailed anatomical description has undergone significant changes over time and drawings depicting the exact course of their fibers have been conflicting. Recently their microanatomy has been redefined ( Fig. 55.2 ). , Grayson ligament as it was described in 1941 appears to be the most condensed part of a trabecular network of fibers that is located volar to the NV bundle and consists of fibers that originate from the outside of the flexor tendon sheet and end in the deep dermis on the contralateral side of the finger. The fibers have an inverted V-shaped orientation, which becomes less pointed during flexion. Since the trabecular network encompasses fat lobules, it seems to accommodate the adaptation of the skin to objects held in the flexed finger hands.
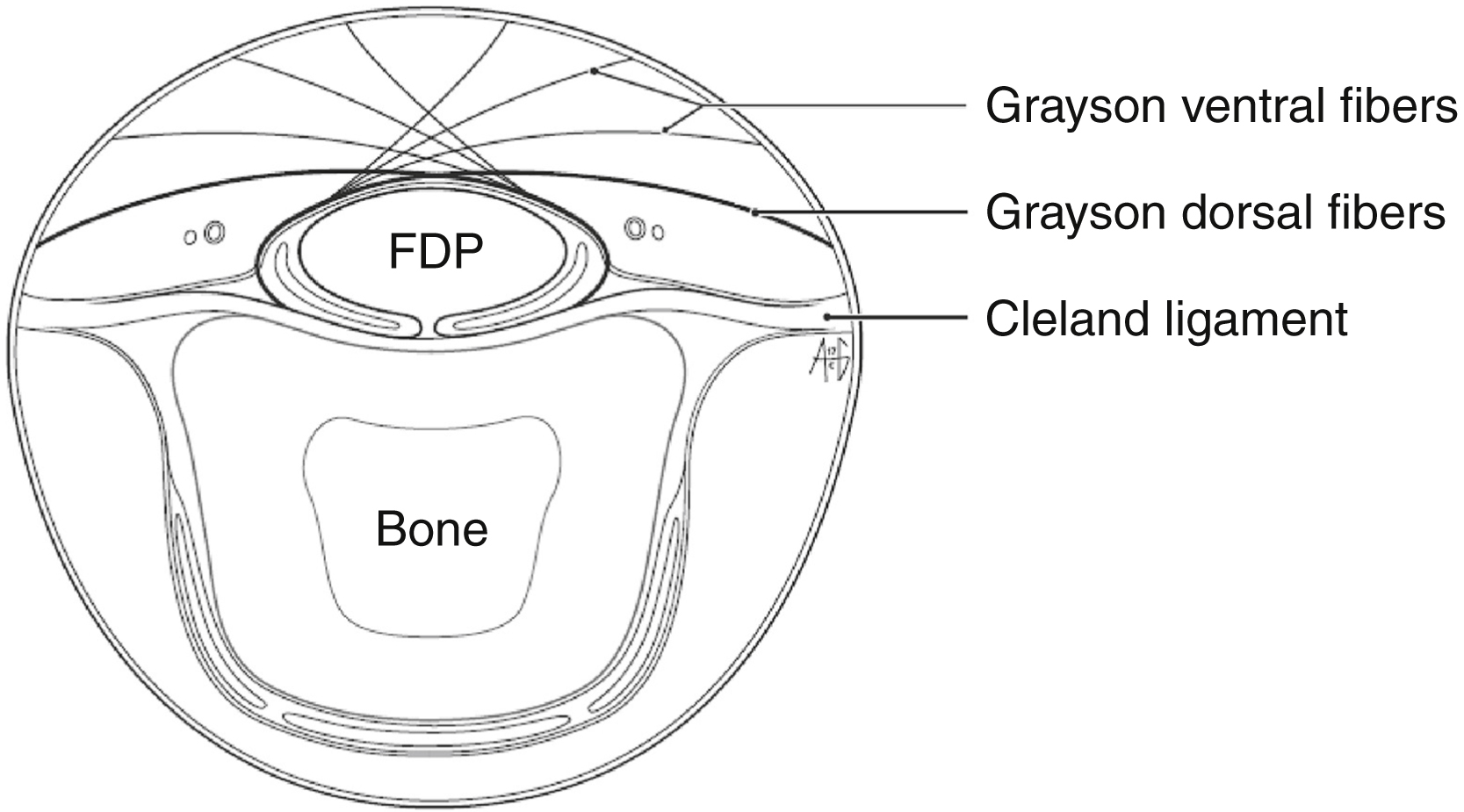
Regarding Cleland ligaments, they have been found to be oriented in pairs located on each side and originating at the level of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints, and from there they course proximally and distally. Three layers have been distinguished: the most volar layer emerges from the fibers of the C1 and C3 pulleys of the flexor tendon sheet, the middle layer from the volar plate, and the most dorsal layer, which actually is a double layer, circumvents the extensor apparatus. After joining just lateral from the volar plate, they fan out proximally and distally, and run dorsal to the NV bundles.
At the place where the hypothenar muscles pass into the little finger there is a blending of fibers that run in all three directions, and they all seem to play a role in Dupuytren disease. At the thenar and in the first webspace there is also a complex three-dimensional network of bands, which may also play a part in the disease.
Band and Cords
There is consensus about the role of most of these fascial structures in the disease ( Table 55.1 ). If a well-defined band becomes affected by disease, it is no longer called “band” but becomes “cord.”
| Anatomical Structure | Name if Affected by DD | Clinical Relevance |
|---|---|---|
| Fascial Structures in the Palm | ||
| Pretendinous band (PTB), prelumbrical band (PLB) | Pretendinous cord (PTC), prelumbrical cord (PLC) | Situated immediately beneath the skin in the palm. Responsible for earliest signs of disease in most patients. Divides in three layers distal to transverse ligament of palmar aponeurosis |
| Layer 1 of PTB | PTC in palm, central cord in finger | Situated immediately beneath the skin, distal to line joining proximal and distal palm crease. May cause MCP joint and PIP joint contracture. Does not displace NV bundle |
| Layer 2 of PTB (spiral band) | Spiral cord | Contracture causes displacement of NB bundle medially and palmarly. May cause MCP joint contracture. Warning sign: Short–Watson sign |
| Layer 3 of PTB | Vertical cord | Dives deep into the hand on both sides of MCP joint. May cause painful triggering |
| Transverse ligament of palmar aponeurosis (TLPA) | – | Runs along line joining proximal and distal palmar crease, deep to PTB/PLB. Not affected by DD. Can be left behind during fasciectomy. Will facilitate subsequent surgery when left intact |
| Ligaments of Legueu and Juvara | – | Connect TLPA to deep transverse ligament |
| Natatory ligament (NTL) | Natatory cord | Situated immediately beneath the skin and superficial to NB bundle. May cause web contracture |
| Proximal/distal commissural band | Proximal/distal commissural cord | Proximal band is extension of TLPA; distal band is extension of NTL. Situated immediately beneath the skin in the first web; may cause first web contracture |
| Abductor digiti minimi fascia | Abductor digiti minimi cord (ADMC) | Forms Y-shape together with PTB and ulnar NV bundle can always be found proximal to junction. ADMC may have multiple levels |
| Deep transverse ligament (DTL) | – | Connects volar plates of MCP joint. Together with ligaments of Legueu and Juvara and TLPA forms nine boxes through which flexor tendons and lumbrical muscles and NV bundles pass |
| Fibers of Gosset | – / nodules in palm? | Dispersed over palmar aponeurosis. Anchor palmar skin to TLPA |
| Fascial Structures in the Digits | ||
| Lateral digital sheet | Lateral digital cord | Situated immediately under the skin on each side of each finger; may displace NV bundle towards midline. May cause MCP joint and PIP joint contracture when involved together with spiral cord and Grayson’s ligament inserting to A4 pulley. May also cause DIP joint contracture as lateral cord |
| Grayson’s ligament | Central cord (CC) | Harbors nodules and cords at proximal phalanx. May cause PIP contracture |
| Cleland’s ligament | Cleland cord | Not easily visualized, since situated behind NV bundle. May cause PIP and DIP joint contracture |
| Transverse retinacular ligament | – | Connects mid slip of the extensor apparatus at PIP joint to the lateral bands and the volar plate. Palmar portion may shorten in severe PIP joint contractures, preventing the lateral bands to slide back after contracture release |
| Oblique retinacular ligament (Landsmeer) | – | Connects volar plate of PIP joint to dorsal capsule of DIP joint. May shorten and cause boutonnière deformity |
At present it is believed that the transverse ligament of the palmar aponeurosis (TLPA) is not affected by DD. Because of this, and since this structure lies palmar to the NV bundles but dorsal to the pretendinous and prelumbrical cords, most surgeons agree that it can be left in situ, and as such serves as a reference point during secondary surgery. Distal to TLPA, however, the dissection always needs to be performed with great care as the NV bundle may be displaced by a spiral cord medially and volarly and may become so intimately related to it that only the experienced eye can discern it. Fat present between a cord and the skin in between TLPA and NT, should raise a high suspicion of a spiral cord. In 2010, Hettiaratchy et al described a number of cases in which a double spiral around the digital nerve was encountered, and in these cases, at least one of the spirals was found in the finger. McFarlane tried to simplify the often complex phenotype of the disease in the finger by defining three anatomical patterns of disease: the central cord, the lateral cord, and the spiral cord. Further work is required to be able to explain all these findings, including those of Hettiaratchy et al, during surgery.
Etiology
The etiology of DD has still not been fully clarified, but it is clear that an interplay of genetic and environmental factors sets the stage for the emergence of the disease. Additionally, the disease occurs more frequently when other diseases such as diabetes mellitus, liver disease or epilepsy needing long-term barbiturate use are present. In addition, there is an association between high levels of exposure to manual labor and vibration (metanalysis odds ratio (OR) for manual work: 2.0 [1.6;2.6] and for vibration exposure: 2.9 [1.4;6.1]) and the development of Dupuytren disease in certain cases. Vibration exposure may also be the reason that DD was found more often in field hockey players.
As for the genetic basis for the disease, a number of older population studies suggesting an autosomal dominant trait with variable penetrance have been set aside by recent Genome Wide Association Studies (GWAS). Using this technology first Dolmans et al and later Ng et al have shown that DD is a polygenetic disease. , It has been calculated that the sibling recurrence risk for DD is 4.5. From a recent Danish study in twins it was concluded that the heritability of Dupuytren’s disease was approximately 80%, showing that genetic factors play a major role in the development of DD.
Pathophysiology and Histology
The cells that have a key role in DD and deposit the superfluous extracellular matrix proteins are called myofibroblasts. They have contractile properties and express α-smooth muscle actin that is known from smooth muscles cells of vascular origin. Much basic research is being devoted to this cell type in DD and it is clear now that myofibroblasts derived from DD nodules exhibit an abnormal response to mechanical tension : they pull back harder than control fibroblast when lattices in which they have been seeded are put under tension. Contracture formation in DD seems to start with fixation of extended myofibroblasts to their extracellular matrix (ECM) followed by their active contraction. The shortened situation is thereafter fixated by the secretion of collagen type I and III and other ECM molecules. The collagen acts to stabilize the contracture, allowing the myofibroblast to relax again and repeat the cycle. Recently, researchers also revealed an influence of adipocytes and macrophages on myofibroblast behavior in laboratory settings. ,
In this respect the classic work of Luck in 1959 and the newer work of Lam et al in 2010 still has some relevance. Luck analyzed the histopathology of Dupuytren disease and proposed a quite artificial subdivision in three phases and Lam analyzed the changes in collagen content over time:
- 1.
During the proliferating phase an abundance of disorganized cells are found in nodules. In this phase Lam et al found that over 35% of the collagen that is deposited is of type III.
- 2.
During the involutional phase the number of cells declines but alignment along lines of stress becomes obvious. The amount of collagen type III diminishes (20%–35%), whereas the amount of type I collagen increases.
- 3.
In the residual phase the pathology resembles a scar and is hypocellular and consists of less than 20% of collagen type III.
The relevance of the presence of nodules with an abundance of proliferating cells is that it has been found to be a predictor for early recurrence. It is, however, good to realize that nodules and cords may occur simultaneously and that nodules may even be found within cords, and that therefore the prognostic value of histological analysis of Dupuytren tissue remains controversial today, as compared to clinical parameters for fibrosis diathesis.
Clinical Assessment and Differential Diagnosis
The early signs of DD are subtle irregularities in the palm under the skin, which may be difficult to discern, even for specialists. Such nodules and skin pits suggest the diagnosis, but the differential diagnosis in that stage should include ganglia and inclusion cysts, occupational hyperkeratosis, callous formation, tenosynovitis, giant cell tumors, and epitheloid sarcoma or even metastatic disease. Once contractures emerge, the diagnosis is usually clear, although one may confuse DD with burn scars, congenital conditions (such as camptodactyly), stuck trigger finger, tendon bowstringing after pulley rupture as in rock climbers, tendon adhesions following infection or repair, tendon imbalance (as in sagittal band rupture), intrinsic joint contractures, CRPS 1 and cerebral or psychogenic spasticity.
The speed at which the disease progresses from nodules to cords to contractures has been subject of research by Lanting and Broekstra, who followed more than 250 people with early DD for 20 months and found that 75% of the participants had either stable disease or showed regression. Regression was correlated with a smaller surface area of pathology as projected on the skin.
Notwithstanding this, once cords have formed, contracture formation is more likely to follow an exponential course than a linear one. Cords in the fingers can be central, and/or on either side and may be short, or extend from the palm to beyond the DIP joint. They can cause extension deficits of any finger joint, although DIP joint contracture is rare. More often, a longstanding PIP joint flexion position leads to an attenuation of the central slip, resulting in a proximal migration of the extensor apparatus, forcing the DIP joint into hyperextension and thereby causing a boutonnière deformity of the affected finger. DD often affects both hands, but often in dissimilar phases.
Grading Systems
The most practical grading systems for research purposes are those of Iselin, and Tubiana and Michon ( Table 55.2 ). Iselin’s staging system is very practical for quick scoring such as during prevalence studies. Tubiana’s system is more sophisticated and the modification suggested by Tubiana in 1986 makes the system relatively complex, hampering its widespread application. The downside of this system is that progression into a higher stage may take 5–40 degrees and is therefore not linear, but stepped. Therefore, for follow-up studies it is better to register and report the active or passive extension deficit (AED or PED) by joint and its sum by ray (TAED/TPED).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


