Dupuytren Contracture
Description
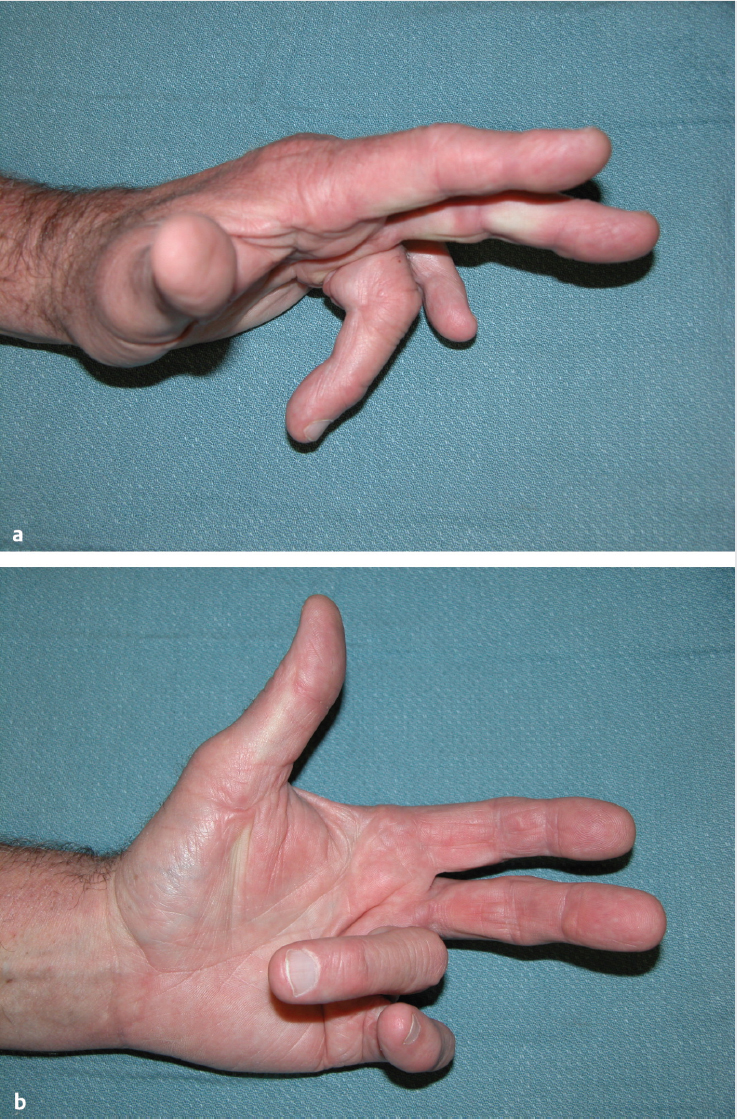
Flexion contracture of the ring and small finger metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints with palmar and digital cords is consistent with Dupuytren contracture.
Work-up
History
Symptoms and degree of impairment of activities.
Age at presentation and duration of disease. Dupuytren diathesis denotes patients with a young age at onset, strong family history, and high incidence of ectopic disease.
Family history of Dupuytren disease.
Ethnicity: More prevalent in northern Europeans and Japanese.
Plantar or penile fibrosis.
Risk factors: Alcohol, epilepsy medications, diabetes mellitus, smoking.
Previous surgical treatment for the condition.
Trauma to the palm can result in traumatic palmar fasciitis.
Physical examination
Observe presence and location of pits, nodules, and cords.
Palpate for asymptomatic nodules and cords.
Tabletop test: Patient is unable to lay the palm flat on a rigid surface.
Note the digits and joints involved and measure the degree of contracture.
Observe for any adduction contracture of thumb.
Measure joint range of motion and note any fixed joint contractures. Simultaneous MCP joint flexion with interphalangeal joint extension points to the absence of fixed joint contractures.
Assess integrity of extensor mechanism.
Flex wrist and MCP joint to create tenodesis effect.
An extensor lag indicates that the central slip is attenuated, and postoperative extension splinting may be required. The patient should be cautioned that full extension of the affected finger will likely not be regained.
Sensory examination of all digits.
Sites of ectopic disease.
Garrod nodes (nodules on dorsum of PIP joint) and knuckle pads (fibrosing lesions on dorsum of PIP joint).
Ledderhose disease (plantar fibromatosis).
Peyronie disease (penile fibromatosis).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


