Introduction to Wound Care in Hidradenitis Suppurativa
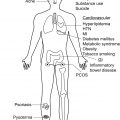
The most important step in managing hidradenitis suppurativa (HS)-related wounds is to treat the underlying disease with appropriate medical and surgical approaches. Even so, proper local wound care is a key cornerstone of management for patients with HS, especially in those with advanced disease. Clinicians will encounter two types of wounds: typical or lesional HS wounds, and post-surgical wounds. The former can be further sub-divided into draining nodules and abscesses, draining tunnels, pyogenic granuloma-like lesions, and frank ulcerations (e.g., knife-like ulcers, pyoderma gangrenosum-like ulcers). Local wound care is instrumental to suppress potential triggers of immune dysfunction, manage exudate, reduce maceration, and decrease the likelihood of secondary infection. The benefits of such an approach include accelerated healing, decreased pain, optimized cosmesis, and improved quality of life. Lesional HS wounds cause pain, produce exudate and odor, and thus have significant and typically underappreciated effects on patients’ quality of life. Social embarrassment, decreased work productivity, and missed employment opportunities are commonly reported. Indeed, many patients with HS live with dressings that require frequent, cumbersome changes that further interfere with everyday activities.
Standard post-surgical wound care is well-established ; however, selection of an effective and comfortable dressing for typical HS lesions is often an overlooked dimension of care with immense potential to improve quality of life. Currently, there are no HS-specific dressings, which is a significant limitation especially with regard to the anatomical location of typical wounds in HS (i.e., skin folds). Therefore, when choosing a dressing for HS-specific lesions, clinicians should take into account the location and morphology of lesions, the degree of pain and inflammation, amount of exudate, odor, and the cost and availability of the product. The ideal dressing for HS-specific lesions should: appropriately absorb exudate to maintain healthy moisture balance, protect the skin from external trauma and infection; promote collagen synthesis and re-epithelialization; stay in place to avoid friction; and be appropriately shaped to fit curved locations if necessary. Selecting the optimal dressing for a given patient is challenging given that HS classically involves difficult anatomic areas (e.g., groin, axillae) and is characterized by fluctuating disease activity.
Evidence to support optimal choice of dressings for HS is scarce and limited to few small studies. Current knowledge is primarily derived from expert opinion and studies on acute wounds and other types of chronic wounds. Recommendations herein are thus based on synthesis of this available data by experts in HS and wound care.
Given lack of evidence and the heterogenous nature of the disease, it is unlikely that one dressing will fit the needs of all patients or lesions at all times. Therefore, clinicians must become familiar with the fundamental properties of the dressings available on the market and together with their patients build a regimen that will address the patients’ needs, dynamic as they may be. Key to a successful wound care regimen is the realization that typically, wound care is delivered by the patient on a daily basis, at home. Therefore, treatment planning should always begin with listening to the patient’s needs (e.g., work schedule, access to supplies and home care), assessing their health literacy and ability to care for their disease, and ensuring that the final treatment plan is practical. Clinicians should demonstrate dressing changes for the patients and provide written instructions, as well as other resources, in order to ensure the success of the wound care plan.
In this chapter, a lesion-based clinical approach is proposed for each type of HS wound. For clarity, the discussion is divided into management of typical lesions (e.g., nodules, abscesses, etc.) and post-surgical wounds. For each of these broad categories, descriptions and evidence levels for each type of dressing are provided, where applicable. All HS dressing discussed herein, their characteristics, and utility are summarized in Table 20.1 . Finally, an overarching algorithm for dressing selection in HS patients is outlined.
| Type | Subtype | Strengths | Weaknesses | Utility in HS |
|---|---|---|---|---|
| Moist | Hydrogel | Maintain moist environment Cools and soothes skin Facilitate autolytic debridement | Poor absorptive capacity | Dry to minimally exudative Acute nodules Simple post-surgical |
| Absorbent | Gauze | Low cost Easy to acquire | Requires tape which may be irritating May be painful to remove | Mild-to-moderately exudative (non-adherent gauze) |
| Absorbent | Abdominal Pads | Absorbent | Expensive Bulky | As cost/coverage necessitates |
| Absorbent | Infant Diapers/Adult Briefs/Sanitary Napkins | Highly absorbent Can be bought in bulk Wick away moisture | Bulky May be uncomfortable | Cost-effective solution |
| Absorbent | Foams | Easily removable Impregnable with antimicrobials Flexible, pliable High absorptive capacity | Expensive | Moderately exudative Nodules Chronic Tunnels Post-surgical (simple or complex) |
| Absorbent | Hydrocolloid | Maintain moist environment Temperature regulation Facilitate autolytic debridement | Unpleasant odor/color changes | Mild-to-moderately exudative Chronic Tunnels |
| Absorbent | Hydrofiber | Higher absorptive capacity than hydrocolloids May be less painful to remove | Not compatible with oil-based products, e.g., petroleum jelly | Mild-to-moderately exudative Simple post-surgical |
| Absorbent | Alginate | Highly absorbent Hemostatic properties Reduce bacterial infections Long wear-time | Expensive Distinctive odor May disintegrate quickly | Moderately exudative Deroofed nodules Post-surgical (simple or complex) |
| Absorbent | Superabsorbent | Highest absorptive capacity | Expensive | Highly exudative Acute Tunnels Post-surgical (simple or complex) |
| Antimicrobial | Silver | Bactericidal May control odor | May inhibit acute wound healing | Clinical signs of infection |
| Antimicrobial | Iodine | Bactericidal Does not impede healing | May irritate skin | Clinical signs of infection |
| Antimicrobial | Honey | Bactericidal Relieves pain and inflammation in acute wounds | No evidence for efficacy in chronic wounds | Clinical signs of infection |
| Antimicrobial | Topical Antiseptics | Reduces development of bacterial antibiotic resistance | Effects attenuated by biofilms | Clinical signs of infection Often recommended as maintenance therapy |
| Contact Layers | Contact Layers | Easy to remove Will not disrupt wound bed | Requires secondary dressing |
Dressings for Typical Hidradenitis Suppurativa Lesions
Typical HS lesions to consider include acute inflammatory nodules and tunnels both acute (flared) and chronic. Acute HS nodules tend to be painful and have minimal to no drainage. Given these characteristics, acute nodules would most benefit from non-adherent dressings with cooling effect such as hydrogel or hydrocolloid dressings. These atraumatic dressings will limit skin damage and minimize trauma and pain with dressing changes. In case drainage occurs from a nodule, foams may serve as an added padded layer on the affected skin, further aiding with pain management and providing excellent absorption.
Flaring tunnels are often associated with pain and heavy drainage. Dressings of choice for these lesions therefore include absorbent and superabsorbent dressings (see section “Absorbent Dressings for Typical HS Lesions”). Chronic tunnels, that is, those which have failed to heal by approximately 40% within 4 weeks, ought to be treated as chronic wounds. Chronic wounds typically exhibit increased fibrinogen and fibrin, which are thought to impair the wound healing process. Chronic wounds are also at risk of infection, and may require debridement. Depending on the amount of drainage, hydrocolloid dressings (see section “Superabsorbent Dressings for Typical HS Lesions”) or foams (see section “Foam Dressings for Typical HS Lesions”) can be beneficial for these, as they can facilitate wound healing by assisting with autolytic debridement.
Absorbent Dressings for Typical Hidradenitis Suppurativa Lesions
The 2008 consensus on wound exudate management per the World Union of Wound Healing Societies recommends absorbent dressings for heavily exudating wounds. These include foams, gelling fibers, and super-absorbent polymers. These dressings will be discussed in the sections below. Additionally, hydrocolloid dressings and over-the-counter absorbents are discussed. Overall, data on absorbent dressings for typical HS lesions is limited. Data on the use of absorptive dressing for primary HS lesions is critically needed to guide clinicians. In the interim, clinical judgement should be practiced for dressing selection. Close follow-up is advised in order to understand the amount of dressings used by the patient over the course of an average week in order to ensure adequate supply is available.
Foam Dressings for Typical Hidradenitis Suppurativa Lesions
Foam dressings are composed of semipermeable materials that aid in managing wound exudate. The absorptive capacity of foams depends on the thickness of the dressing. The contact area of foam dressings is non-adherent, making these dressings easily removable, thus preventing dressing-related trauma and minimizing discomfort and pain at the wound site. Additionally, foams can be impregnated with anti-microbial agents such as silver or honey (see section “Contact Layers for Typical HS Lesions”). Foams are flexible and can be molded or cut to fit different body parts, making them particularly useful in HS. Studies that have attempted to establish optimal wound care for HS have favored foam dressings for these reasons. Finally, foam dressings have increased capacity for autolytic debridement, which may be a useful property in tunnels and frank ulcerations when appropriate.
Superabsorbent Dressings for Typical Hidradenitis Suppurativa Lesions
Superabsorbent dressings are multilayered with highly absorptive materials, such as cotton, rayon, or cellulose, designed to manage highly exudative wounds. These can be used as primary or secondary dressings. A prospective observational study done on 15 patients with highly exudating wounds demonstrated that these dressings reduced maceration as well as the number of dressing changes required from once daily to twice weekly. Superabsorbent dressings were found to overall reduce complications associated with exudate production, save time and cost for caregivers, and increase patient comfort. This is significant in HS, where exudate management has a large impact on quality of life.
Hydrocolloid and Hydrofiber Dressings for Typical Hidradenitis Suppurativa Lesions
Hydrocolloid dressings are composed of gelatin, carboxymethylcellulose, pectins, and an occlusive backing. The occlusive backing is typically in the form of a film or foam and serves to protect the wound from the environment. This allows patients to maintain their daily activities, such as showering, with more ease. Hydrocolloids form a gel when in contact with exudate. This gel helps to protect wounds by maintaining wound moisture, temperature, and facilitating autolytic debridement. Hydrocolloid fiber (Hydrofiber) dressings build upon the gel-forming properties of hydrocolloids and boast an increased absorptive capacity. Notably, available data on hydrocolloids and hydrofibers relates to post-surgical wounds while data on their use in primary lesions of HS is lacking. Nonetheless, these dressings are useful for typical HS lesions exhibiting mild-to-moderate levels of exudate.
Over-the-Counter Absorbent Dressings for Typical Hidradenitis Suppurativa Lesions
Other relatively cost-effective and simple dressings that can be used to treat typical HS lesions include infant diapers, adult briefs, and sanitary napkins. These are highly absorbent, can be bought in bulk, and are designed to wick away moisture. However, they can be bulky and uncomfortable compared to the other dressings discussed in this chapter. Abdominal pads are very effective for exudative wounds but are even more expensive (albeit often covered by health insurance policies) and bulky than the aforementioned options.
Topical Antiseptics for Typical Hidradenitis Suppurativa Lesions
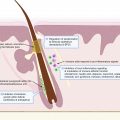
The role of cutaneous flora in the pathogenesis of HS is becoming increasingly recognized. Dysregulation of normal skin flora and secondary infection of active HS lesions are significant drivers of disease activity. Additionally, biofilms (extracellular polymeric matrices secreted by bacteria which grant protection against host defenses and conventional therapies) may contribute to the pathology seen in HS, though their exact role remains unclear. Accordingly, topical antimicrobial therapy is a mainstay of therapy for patients with HS and topical antiseptics and cleaning solutions are commonly employed for this purpose in the management of HS. Therefore, when considering wound care for typical HS lesions, topical antiseptics are essential for a comprehensive approach. Chlorhexidine, a broad-spectrum biocide, is used to reduce the stimulation of the immune response by resident bacteria. However, the effects of chlorhexidine are greatly impaired in the presence of biofilms. Although it is commonly recommended by clinicians, clinical evidence for the use of chlorhexidine in HS is low, and its benefits lie mainly in the reduction of bacterial resistance compared with oral antibiotic therapy alone.
Contact Layers for Typical Hidradenitis Suppurativa Lesions
Contact layers are designed to lie directly on the wound bed and protect wound bed tissue as well as the surrounding skin during healing. They are generally non-adherent or lightly adherent and, while not highly absorbent themselves, are designed to allow upward drainage of fluids into a secondary dressing. Contact layer dressings have been shown to promote granulation and epithelialization in non-HS related wounds. These dressings are easy and painless to remove and will not disrupt the wound bed during dressing changes. In HS patients, using a contact layer as a primary dressing that can stay on the wound for 2 to 3 days will allow for more frequent secondary absorbent dressing changes (e.g., alginate) without trauma to the wound.
Moist Dressings for Typical Hidradenitis Suppurativa Lesions
Hydrogel dressings are semi-occlusive, gel-based products with a high (90%) water content that protects the wound bed and provides a moist wound-healing environment. In addition to re-hydrating wounds and eschars, hydrogels are also designed to aid in autolytic debridement without harming epithelial cells or granulation tissue. Hydrogels have a cooling and soothing effect on the skin, which is particularly useful in HS-specific lesions. Hydrogels work by expanding when in contact with water, or fluids such as wound exudate. These types of dressings are recommended for typical HS lesions that dry or are mildly exudative and can remain in place for up to 3 days.
Odor control for Typical Hidradenitis Suppurativa Lesions
Slough, bacteria, and exudate release volatile organic compounds that are processed as odor by the olfactory apparatus. Malodor is a significant driver of decreased quality of life for patients with HS as it contributes to embarrassment, stigma, and poor self-image, increasing the barrier to interpersonal relationships. A high level of odor has been linked to a greater degree of social isolation as well as more significant quality-of-life impairment as measured by the Skindex-29. Odor in HS is thought to be a marker of bacterial colonization, and it has been suggested that antiseptic dressings may help in this regard by destroying surface bacteria. Dressings containing charcoal may be useful in absorbing wound-associated odors. There are many purported treatments for wound odor; however, few are well-studied in high-quality randomized-controlled trials. Silver dressings and metronidazole gel have the best evidence to support efficacy in combating chronic wound odors, but HS-specific data is currently lacking.
Post-surgical wounds
Post-surgical wounds can be closed primarily, left for secondary intention healing, or grafted. Management of post-surgical wounds in HS is generally similar to other post-surgical wounds. A comprehensive discussion of post-surgical wound care is beyond the scope of this chapter. Generally, the astute surgeon should follow current surgical guidelines. A summary of the existing evidence for post-surgical wounds after HS-related surgery is presented herein. Current guidelines cite minimal evidence to support any specific dressing for post-surgical wounds in HS. Complex post-surgical HS wounds that have become infected or otherwise failed to follow an appropriate healing trajectory may require additional attention. Absorbent dressings (i.e., foams, alginates, hydrofibers, etc.) or negative-pressure wound therapy (NPWT) may be useful for such slow-healing wounds. Post-surgical wounds should be closely monitored for infection and cultured appropriately if necessary. Antimicrobial dressings can be used in the event of an infected wound.
Absorbent Dressings for Post-Surgical Wounds in Hidradenitis Suppurativa
Alginates for Post-Surgical Wounds in Hidradenitis Suppurativa
Alginate dressings are light, nonwoven fabrics derived from algae or seaweed. Designed for moderately to heavily exudating wounds, they are highly absorbent, have mild hemostatic properties, reduce bacterial infections, and can stay on the wound bed for days. Alginates have been used in combination with silicone dressings for post-surgical wound care of surgically deroofed HS cysts and sinuses, as well as for Skin Tissue-Sparing Excision with Electrosurgical Peeling (STEEP) procedures for patients in advanced stages of HS. Alginate dressings tend to fall apart faster than other dressings, which may present a significant limitation in use for primary HS lesions, as parts of the dressing may lodge in sinuses. Use of a contact layer as a primary dressing may improve the overall performance of an alginate dressing.
Hydrocolloids and Hydrofibers for Post-Surgical Wounds in Hidradenitis Suppurativa
The use of these dressings has specifically been described in HS. One study described the use of hydrocolloid dressings for 2 days in addition to polymyxin B ointment and bacitracin on 61 HS patients who underwent CO 2 laser excision. All patients in this study healed with excellent cosmetic outcomes and comfort. Hydrofibers have been used for postoperative care of HS patients undergoing CO 2 laser surgery. A retrospective analysis of 35 patients treated with hydrofibers for CO 2 laser surgical wounds of different sizes and anatomic locations, left to heal by secondary intention, found a mean healing time of 4 weeks. A second cohort of nine patients, some healed by first intention and others by second, found a mean healing time of 2 weeks. It has been suggested that hydrofiber dressings may be less painful to remove than other dressings for these post-surgical wounds, however these claims have not yet been studied in a controlled manner.
Antimicrobial Dressings for Post-Surgical Wounds in Hidradenitis Suppurativa
Silver for Post-Surgical Wounds in Hidradenitis Suppurativa
The antimicrobial properties of silver have been known for centuries. Ionized silver (Ag 2 + ) is toxic to a wide variety of pathogenic organisms commonly found in wounds. Accordingly, silver has been incorporated into a variety of dressings which vary in the types of material used, formulation of the silver compound, location of compound in the dressing, and total silver content released into the wound. Although some studies have found silver to have beneficial effects on healing outcomes in chronic wounds, others have failed to observe any differences between silver and non-silver dressings. Studies focusing on silver dressings in the context of HS are limited. Silver dressings should be used judiciously as they are not intended to be used for extended periods, particularly if there is no infection. Additionally, in vitro and in vivo studies have found that silver is toxic to fibroblasts and keratinocytes and thus inhibits acute wound healing by slowing re-epithelialization.
Iodine For Post-Surgical Wounds in Hidradenitis Suppurativa
Iodine is another agent with broad-spectrum antimicrobial activity, boasting anti-inflammatory properties and an excellent safety profile. It has not been found to disturb wound healing. In a study where 44 HS patients with various stages of disease activity underwent deroofing of lesions, postoperative wound care was achieved with 5 days of mupirocin, with wedging to keep the wound open, followed by once-daily dressing changes with iodine-ointment-containing gauzes. The surgical defects were found to generally heal with cosmetically acceptable scars. However, the small number of patients and lack of control arm limits the applicability of these data for treating people with HS related wounds, except to suggest an acceptable safety profile for both silver and iodine. Although less likely with modern iodine formulations (e.g., iodophors), iodine-containing compounds may cause skin irritation.
Honey for Post-Surgical Wounds in Hidradenitis Suppurativa
Honey has antibacterial, anti-inflammatory, and antioxidant properties that can be harnessed and incorporated into a dressing in order to promote wound healing. Honey’s antibacterial effects are due to its high acidity, osmotic effect, and hydrogen peroxide content. The usage of honey in the setting of wound healing has been associated with pain relief and a decreased inflammatory response. However, these effects have only been demonstrated in acute wounds such as acute burns and postoperative wounds. Honey has not been found to be effective in chronic wounds such as chronic leg ulcers. The use of honey-impregnated dressings may therefore be limited to acute HS wounds, and postoperative wounds in particular.
Negative-Pressure Wound Therapy for Post-Surgical Wounds in Hidradenitis Suppurativa
NPWT may also be considered for complex wounds, heavily exudating wounds, those not closed primarily, or those with significant depth. NPWT helps by increasing oxygen tension, decreasing bacterial load, stimulating cellular activity, and promoting granulation tissue and also serves to prepare the wound bed for grafting if necessary.
Gauze Dressings for Post-Surgical Wounds in Hidradenitis Suppurativa
Gauze has historically been ubiquitous in wound care and may still play a role in the treatment of patients with HS despite the availability of modern dressings. Its low cost and accessibility can make it an attractive choice, although it requires the use of tape to adhere to the skin, which may be irritating and cause pain during dressing changes. Gauze also tends to stick to wounds when exudate dries which may further increase pain. Non-adherent gauze may serve similar purposes without the pain and disruption of the wound bed associated with changing a dry gauze. In a cohort of 185 patients undergoing CO 2 laser excision for HS lesions, patients received postoperative wound care with antibacterial ointment and hydrocolloid dressing for 2 days, followed by daily warm water compresses, petroleum jelly, and a non-adherent gauze dressing until healing. All patients healed with acceptable-to-excellent cosmetic and recurrence outcomes during a follow-up period ranging from 1 to 19 years.
Summary
Selection of an effective dressing for HS is challenging due to the inherently fluctuant nature of the disease and diverse array of lesions that may be present. Many factors must be taken into account during dressing selection, namely: the location and morphology of lesions, the extent of disease activity, amount of exudate, odor, and the cost and availability of the product. A summarized approach to dressing selection for HS based on wound type and characteristics can be found in Table 20.2 .
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


