Abstract
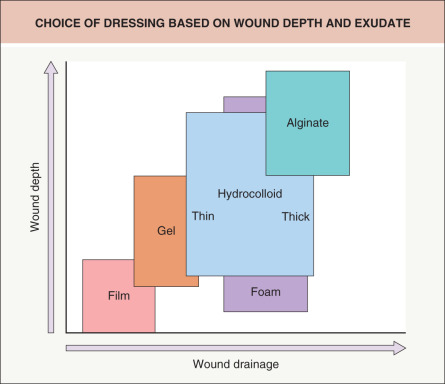
Chronic wounds fail to heal in a timely fashion, do not progress through the normal phases of wound healing in an orderly manner, and may remain in a persistent inflammatory and/or proliferative phase. By creating a moist wound environment, dressings can be used to speed the healing of chronic wounds. The choice of dressing is often determined by wound characteristics (e.g. depth, amount of exudate), availability, cost, and patient preference. The main categories of wound dressings are films, foams, hydrogels, alginates, and hydrocolloids.
The presence of bacteria in the wound environment may delay healing and when critical colonization is present, dressings impregnated with antiseptics (e.g. silver, iodine) can be employed. Negative pressure wound therapy is helpful in the management of various wounds, especially those that are postsurgical. An important component of the treatment regimen for venous ulcers of the lower extremities is compression (e.g. stockings, bandages).
Scientific and clinical advances, including growth factors, stem cells and skin substitutes, have increased the therapeutic options for refractory chronic wounds. Dermatologists often care for patients with wounds and need to know how to select and apply wound dressings based upon the specific clinical scenario in order to promote healing and improve the patient’s quality of life.
Keywords
wound healing, films, foams, hydrogels, alginates, hydrocolloids, hydrofibers, gelling fibers, antiseptics, local wound care, dressings, debridement, compression therapy, negative pressure wound therapy, hyperbaric oxygen, PDGF, skin substitutes, moisture-retentive dressings
- ▪
Wound dressings have evolved from simple wound coverings to more active wound management tools that directly interact with the wound environment
- ▪
No perfect dressing exists for all wounds but when used appropriately, dressings can improve healing time and cosmesis as well as reduce pain and infections
- ▪
Semipermeable or occlusive dressings provide a moist environment, retain wound fluid that contains growth factors conducive to healing, and promote a low tissue oxygen tension that stimulates angiogenesis and deposition of collagen
- ▪
The major types of moisture-retentive dressings include films, foams, hydrogels, alginates, gelling fibers, and hydrocolloids
Introduction
Dermatologists are involved in the care of a variety of acute and chronic wounds including surgical incisions. The range of treatment options is substantial and expanding, providing therapeutic flexibility. Appropriate wound dressing selection requires an understanding of the properties of various dressings, as well as their advantages and disadvantages. As the wound heals, the ideal dressing may change based on the amount of exudate, necrotic tissue and pain or degree of superficial infection ( Table 145.1 ).
| SELECTION OF APPROPRIATE DRESSINGS | |
|---|---|
| Wound factor | Dressing |
| Exudate | |
| Hydrogel |
| Film, hydrocolloid |
| Foam, alginate, gelling fibers |
| Pain | |
| Hydrogel, soft silicone, non-adherent |
| Bleeding | |
| Alginates |
| Superficial infection | |
| Impregnated with silver, chlorhexidine, iodine, honey, or methylene blue plus gentian violet as antiseptics |
Moist Healing Environment
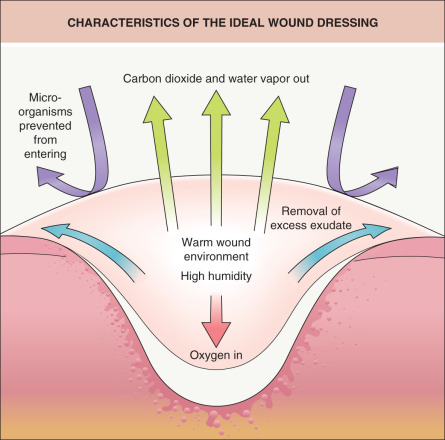
Providing a moist wound environment is an important principle of wound healing. There are several mechanisms by which moisture assists the reparative process, the most basic of which is the suppression of tissue desiccation and crust formation. Studies by Winter clearly demonstrated that uncovered, air-dried wounds developed thicker crusts and re-epithelialized at a slower rate (see below). This slower rate has been attributed to the requirement of the regenerating epidermis to migrate below the dry fibrous tissue to a region of moisture where live cells survive. It is only in such an environment that epidermal cells can move toward bridging the defect of the wound; therefore, the thicker the scab, the deeper the migration. This, along with the continuing loss of dermis and a reduction in adnexal structures, contributes to greater scar depth and worse cosmetic outcome .
By reducing moisture transmission, moisture-retentive dressings optimize healing by providing a moist environment ( Fig. 145.1 ). In addition, they increase the availability of growth factors and matrix materials and maintain an electrical gradient within the wound, which also promotes healing.
Role of Debridement
Debridement is the removal of necrotic, contaminated, or foreign material from a wound or from areas adjacent to the wound. It is considered a key component of wound management . Five types of debridement exist: surgical, mechanical, autolytic, enzymatic, and biologic. Although surgical debridement is often the fastest and most direct way of removing unhealthy tissue, it may not be the method of choice for all patients, depending on patient characteristics and preferences, the frequent need for analgesics, possible bleeding, and the practitioner’s level of expertise. An example of mechanical debridement is the dry-to-wet dressing that is employed for wounds with significant necrotic tissue but does not distinguish between viable and non-viable tissue (see Ch. 105 ).
In autolytic debridement, occlusive dressings provide a moist wound environment which promotes the lytic activity of enzymes present in accumulated wound fluid. This assists in the clearance of residual debris during early wound healing. Enzymatic (chemical) debridement involves the topical application of an enzymatic agent and can be used to supplement autolytic debridement. Currently, one agent is FDA-approved: collagenase (Santyl ® ) ointment. It assists in the removal of devitalized tissue and aids in granulation tissue formation and re-epithelialization.
Biologic debridement employs fly larvae (maggots) and has been used for centuries to debride chronic ulcers. Nowadays, the most commonly used maggots are those of the green bottle fly, Lucilia sericata . Maggots digest necrotic tissue via collagenases and trypsin-like enzymes, thereby exposing healthy tissue. They also have antimicrobial effects, including secretion of anti-bacterial compounds (e.g. phenylacetic acid, phenylacetaldehyde) in addition to ingestion and subsequent killing of Gram-positive bacteria (including MRSA) and, to a lesser extent, Gram-negative bacteria. In a clinical trial of 267 patients with leg ulcers, larval therapy led to faster debridement than hydrogel therapy, but larval therapy has not been shown to improve healing rates or decrease bacterial load .
History of Wound Dressings
The use of wound dressings dates back to antiquity. For at least 4000 years, fabrics such as linen were employed, until woven absorbent cotton gauze was introduced in 1871. The Edwin Smith Surgical Papyrus, which is one of the earliest medical treatises (circa 1615 BC), describes the use of linen strips and plaster to dress wounds, stating that closed wounds would heal more quickly than open wounds . Ancient documents disclose how lint was used to pack and fill open wounds and how bandages were used to re-approximate wounds in order to facilitate healing. Linen strips were sometimes coated with grease or oil in order to prevent adherence to wounds or with honey to create a semi-occlusive and adherent dressing .
Lister connected the presence of pus with infection. However, this association became linked so strongly that it was held that one is always indicative of the other, which is not always true. This association significantly interfered with the acceptance of occlusive dressings. Although the work of Pasteur, Koch and Lister in the late 1800s on the cause of bacterial infections spurred the investigation of specific therapies for wound management, it was not until the mid-1900s that the understanding of wound healing changed. Despite the teaching of the Smith Papyrus, it was believed wounds healed more quickly if kept dry and uncovered.
In 1948, Oscar Gilje described a “moist chamber effect” for wound healing . Two years later, Schilling and colleagues studied common minor wounds with highly occlusive or semi-occlusive nylon films and found semi-occlusive dressings to be more effective for healing than open treatment. The finding that semi-occlusive dressings were more effective than the highly occlusive dressings is thought to have set back further study. In 1962, George Winter conducted the landmark study on moist wound healing, demonstrating a 30% greater benefit of occlusive dressings compared with air drying of wounds . Many studies conducted since Winter’s seminal work have supported the benefits of moist wound healing by occlusive dressings.
Functions of a Wound Dressing
The essential function of every dressing is to optimize the healing environment, but because the process of wound repair is dynamic (see Ch. 141 ), each stage may require a different dressing. While an ideal wound dressing would have many positive features (see Table 145.1 ), the main function of a dressing is to promote healing by protecting the wound from trauma, bacterial invasion or exposure to caustic substances; this is especially important during the acute inflammatory stage when promotion of granulation tissue formation and epithelialization is crucial. In addition, the dressing should be composed of a material that does not shed fibers or other material into the wound that could lead to a foreign body reaction or an irritant or allergic contact dermatitis . The “ideal” dressing that meets all of these requirements for every wound type does not yet exist ( Table 145.2 ). However, given the array of dressings available, it is possible to achieve one’s goal.
| CHARACTERISTICS OF AN IDEAL DRESSING – COMPARISON OF MOISTURE-RETENTIVE DRESSINGS | |||||
|---|---|---|---|---|---|
| Comfort | Absorbency | Pain relief | Easy to re-apply | Debridement | |
| Films | + | + | |||
| Foams | + | ++ | + | + | |
| Hydrogels | ++ | + | ++ | + | ++ |
| Alginates | ++ | ++ | + | + | |
| Hydrocolloids | + | ++ | + | + | + |
Traditional Wound Dressings
Wound dressings can be categorized either by the dressing technique and how the dressing is utilized relative to the wound (see below) or by the composition and structure of the dressing . Naturally occurring materials such as cotton, silk, linen, or cellulose-based substances have a long history of use and have been produced in various combinations for maximal clinical usefulness.
The basic cotton gauze bandages in use today are frequently composed of cotton plus cellulose acetate (added for increased absorbency) and are manufactured with or without various substances incorporated into the fabric. Gauze bandages are inexpensive and easy to use but have limited moisture-retentive capacity; the latter can be enhanced by impregnation with hydrophobic coatings. White petrolatum and other ointments such as soft paraffin wax (e.g. Vaseline ® gauze, Aquaphor ® gauze, Adaptic™ dressing), with or without antibacterials such as povidone-iodine (Betadine ® ), sulfadiazine, bismuth tribromophenate (Xeroform™ dressing), framycetin or chlorhexidine, are examples of impregnated substances. Balsam of Peru is found in the tulle gras dressing used predominantly in Western Europe. These medicated dressings are often composites of rayon, nylon or gauze and are used for malodorous wounds such as chronic ulcers. Activated charcoal cloth (with or without antibacterial silver salt) is also used for exudate absorption plus odor control.
These types of dressings are placed directly against the wound bed and have the advantage of less adherence to the wound as well as the ability to mold into the depression of deeper wounds for the purpose of filling dead space and providing absorption. The disadvantage of this type of dressing is the potential for maceration of the wound and surrounding skin should the dressing remain in place for an extended period of time. While traditional dressings are relatively inexpensive and readily available, they require frequent replacement, which is time-consuming and can be costly due to the expense of nursing care .
Primary dressings are those that are in contact with the wound whereas secondary dressings cover the primary dressing and/or secure the dressing in place. Most conventional dressings are “layered” and are constructed as either “pressure” or “non-pressure” dressings. A layered dressing is usually created in three parts: (1) the contact or interface layer, which is usually a non-adherent, fluid-permeable material that makes direct contact with the wound; (2) the absorbent layer, usually a cotton pad, gauze or other such material, which is placed on top of the contact layer to “wick in” and retain wound exudate and help the dressing mold to the shape of the wound; and (3) the outer layer or wrap, often tape or other banding material for retention of the underlying layers. Each layer is placed in close approximation to the prior one, without gaps or air pockets, and should increase in size and degree of overlap, from wound bed to outermost layer.
A “pressure” dressing has more bulk added to the absorbent layer and is used to assist hemostasis. Usually applied immediately after debridement or surgery, a pressure dressing is changed to a lighter dressing within 24 hours. In addition to limiting bleeding, the pressure dressing also reduces edema and supports the surrounding tissue. It is important to be aware of the amount of pressure exerted upon the wound bed so as not to create localized ischemia, potentially resulting in tissue necrosis .
First and Second Intention Healing
Typically, primary closure is employed for postsurgical wound defects that are clean and free of debris. Aseptically placed sutures provide hemostasis, reduce the possibility of wound infection, and may improve the ultimate cosmetic result. After suture removal, the use of external splinting tape (e.g. Steri-Strips™) or tension-relieving dressings (e.g. embrace ® ) supports the tissues, enabling favorable collagen remodeling that may limit scar formation and hypertrophy.
Second intention healing is often employed following cutaneous surgical techniques such as tangential biopsy, cryosurgery, laser surgery, excision ( Fig. 145.2 ), and curettage. In such cases, moisture at the wound bed is the key to optimal spontaneous healing. A semi-occlusive dressing is the treatment of choice, with the topical application of ointment directly on the wound. Monitoring the wound for signs of infection and preventing the wound bed from drying until re-epithelialization has occurred are usually sufficient measures for the management of this type of surgical wound .

Wound Cleansers
The removal of loose debris from the wound surface is termed wound cleansing and is a component of local wound care . Optimal wound cleansers should have low cytotoxicity and they include water, isotonic normal saline (0.9% sodium chloride), and in some cases, dilute acetic acid or other mild acid solutions. Isotonic normal saline is a good cleanser for the majority of wounds and a Cochrane collaboration review found clean tap water as a suitable alternative .
Wound cleansing can be performed via three methods: compresses (gauze squeezed so no excess fluid), soaking (saturated gauze), and irrigation. Irrigation can cause trauma to the wound bed and is not recommended for deep wounds unless one can be assured no cleansing fluid is retained within a “pocket” in the wound.
Topical Antimicrobials and Dressings That Contain Antimicrobial Agents
The presence of bacteria in wounds may delay acute wound healing and it contributes to delayed healing of chronic wounds. In the latter, resident bacteria are often held in balance by host resistance. Bacteria compete with adjacent cells for oxygen and nutrients and they can also produce toxins that delay healing. Differentiating a wound in bacterial balance from a wound where bacteria are delaying healing remains a challenge.
While a clean wound created with good aseptic technique (e.g. sutured surgical excision) does not require topical antimicrobials, they may be needed for some acute and chronic wounds. Topical antimicrobial agents include antiseptics and antibiotics. Antiseptics non-selectively destroy or inhibit the growth of microorganisms, whereas antibiotics are only effective against specific bacteria . Due to the emergence of bacterial resistance and the risk of development of allergic contact dermatitis, topical antibiotics are typically reserved for superficial cutaneous infections such as impetigo. Mupirocin, retapamulin, and fusidic acid are indicated for the treatment of cutaneous infections due to Staphylococcus aureus or Streptococcus pyogenes . Silver sulfadiazine has broader antimicrobial coverage, but a pseudo-eschar can form which may delay healing . Triple antibiotic cream or ointment formulations available over the counter may contain combinations of polymyxin, gramicidin, bacitracin, and/or neomycin; however, the latter two are amongst the ten most common allergens in North America (see Ch. 14 ).
Because antiseptics often affect cellular metabolism (including cell wall formation), they are less often associated with the emergence of resistant organisms. The antimicrobial activity and cellular toxicities of various antiseptics are listed in Table 145.3 . Silver has been used since ancient times for treating wound infections due to its antimicrobial activity. When in contact with wound fluid, silver metallic salt (Ag 0 ) becomes ionized (Ag + ) and highly active against bacteria. The bactericidal action of ionized silver can be explained by the binding of silver ions to tissue proteins or by reactions with chloride anions, which then bind to bacterial DNA and RNA and alter bacterial cell walls and nuclear membranes . Silver also has anti-inflammatory effects and may have angiogenic properties. In addition, silver ions decrease the levels of matrix metalloproteinases (MMPs) that are often up-regulated in non-healing wounds. Despite these effects, a recent Cochrane review found no significantly higher healing rates with silver dressings . Newer dressings, in which high-density polyethylene mesh is impregnated with nanocrystalline silver ( Fig. 145.3 ) , can release antibacterial levels of silver for 3–7 days .
| DRESSINGS THAT CONTAIN ANTISEPTICS | ||||
|---|---|---|---|---|
| Antimicrobial agent | Examples of dressings | Coverage spectrum | Advantages | Disadvantages |
| Silver | Acticoat ® Flex 7 Silver, Actisorb ® Silver 220, Algicell ® Ag (alginate), Aquacel ® Ag, Contreet ® Biatain Ag Foam, ColActive ® Plus Ag, Mepilex ® Ag, PolyMem ® Silver, SilvaSorb ® (hydrogel), Silvercel ® (alginate), Silverlon ® , UrgoTul ® Ag/Silver, UrgoTul ® SSD | Broad-spectrum antibacterial, including MRSA and VRE |
|
|
| Chlorhexidine or polyhexamethylene biguanide (PHMB), a chlorhexidine derivative | Bactigras ™ (chlorhexidine), Kendall ™ AMD foam (PHMB), Kerlix ™ AMD gauze (PHMB) | Broad-spectrum |
|
|
| Povidone-iodine * Cadexomer-iodine polymer * | Inadine ® , Betadine ® cream applied to gauze, Iodoflex ™ , Iodosorb ® | Broad-spectrum antimicrobial – bacteria, fungi, viruses |
|
|
| Honey | Activon Tulle, Medihoney ® Calcium (alginate, hydrogel) | Broad-spectrum antimicrobial – bacteria, fungi, viruses |
|
|
| Methylene blue and gentian violet | Hydrofera Blue ® | Broad-spectrum antibacterial, including MRSA and VRE, and anti-candidal |
|
|
| Hypertonic saline | Mesalt ® | Broad-spectrum | Less irritating to skin | |
* Not to be used in young children, pregnant or lactating women, or individuals with a known iodine sensitivity; to be used cautiously in patients with thyroid disorders.
Chlorhexidine gluconate is a biguanide antiseptic with a wide range of antimicrobial activity against Gram-positive and Gram-negative bacteria, yeasts, and molds. It works by disturbing the cytoplasmic membrane . However, there can be associated cytotoxicity, especially to the cornea, inner ear (in the setting of tympanic membrane rupture), and cartilage; exposure to these structures should be avoided . Systemic and local hypersensitivity reactions have also been observed. A chlorhexidine derivative, polyhexamethylene biguanide (PHMB), appears to be safer and has been added to several wound dressings including gauze, ribbons, foam, and hydrogels.
Iodine is a broad-spectrum antiseptic that is available in different formulations . However, povidone-iodine, a commonly used antiseptic, can inhibit wound healing. In contrast, newer formulations such as cadexomer-iodine polymer, which slowly releases iodine from dextran beads, do not slow healing and have not been found to have toxic effects on keratinocytes. The starch lattice in the cadexomer-iodine polymer is highly absorptive (1 gram absorbs up to 7 ml of fluid) and as the fluid is absorbed, the iodine is slowly released . The iodine confers antimicrobial activity for several days, but is in a low enough concentration that cytotoxic effects are avoided. The frequency of dressing changes is determined by the rate of iodine release, which is largely dependent on wound exudate .
Studies in patients with venous leg ulcers have shown a significant decrease in ulcer size when cadexomer-iodine was compared to hydrocolloid and paraffin gauze dressings . When compared to other treatments for diabetic foot ulcers, cadexomer-iodine was associated with a cost benefit . Because iodine can be absorbed systemically, caution is required when using these dressings in patients with a history of thyroid disease. They should not be used in young children, pregnant or lactating women, or patients with known iodine sensitivity.
Honey is an ancient treatment that has been revived due to recognition of its antimicrobial properties. The latter is related to honey’s high osmolality which minimizes the availability of water to bacteria . Manuka honey, a commonly used type of honey, also contains flavonoids and aromatic acids that have antimicrobial properties. In addition, honey exhibits an anti-odor effect by decreasing the wound pH; release of hydrogen peroxide and glucuronic acid stimulates macrophages/monocytes, promotes inflammatory cytokine production, and provides analgesic and antibacterial effects . A Cochrane review found that topical treatment of superficial and partial-thickness burns with honey may improve healing when compared to some conventional dressings .
Methylene blue and gentian violet , two organic dyes, have been combined in a polyvinyl alcohol sponge to produce an antimicrobial dressing (Hydrofera Blue ® Bacteriostatic Dressing) . These dyes are not released from the dressing, thus avoiding previously reported tissue toxicities. The dressing has broad-spectrum activity against Gram-positive bacteria, Gram-negative bacteria, and Candida spp.
Moisture-Retentive Dressings
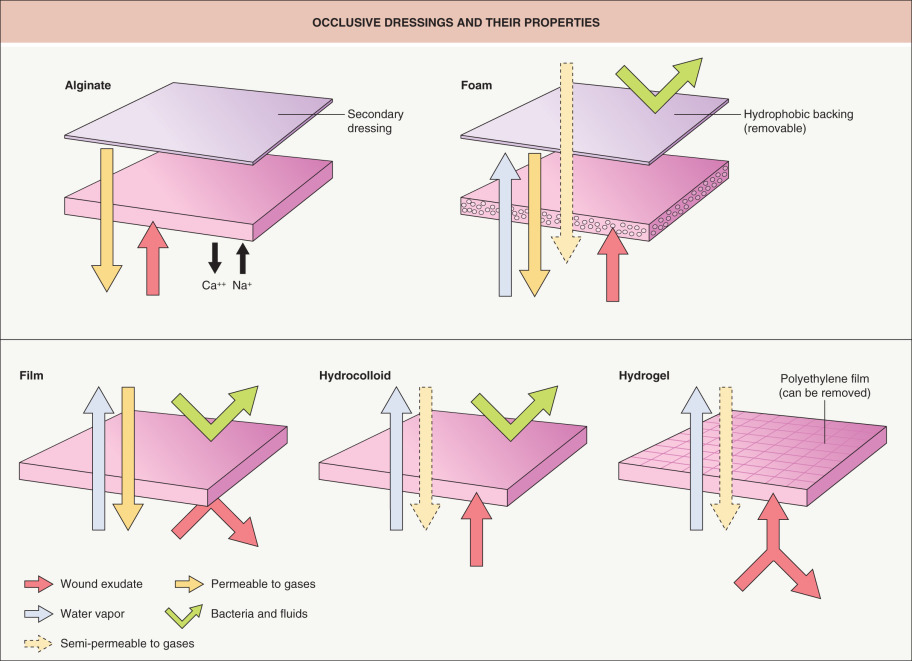
Moisture-retentive dressings, traditionally called passive dressings, are distinct from active dressings, with the former commonly divided into five major groups: films, foams, hydrogels, alginates, and hydrocolloids ( Fig. 145.4 ; Table 145.4 ). In choosing the most appropriate dressing for a particular wound, it is important to strike a moisture balance, i.e. not too dry and not too wet.
| MOISTURE-RETENTIVE DRESSINGS | ||||||
|---|---|---|---|---|---|---|
| Dressing type | Examples | Composition | Permeability | Indicated uses | Advantages | Disadvantages |
| Films | Bioclusive™; Blisterfilm™ Transparent Film Dressing (TFD); Carrafilm™; Mefilm ® ; Opsite™; Polyskin ® II; Silon-TSR ® ; Tegaderm™ TFD; Transeal ® TFD | Thin polyurethane sheet | Semipermeable |
|
|
|
| Foam | Adherent and non-adherent : Allevyn™; Biatain™; Biopatch ® ; CuraFoam™; Flexzan ® ; Hydrosorb ® ; Lyofoam ® ; Mepilex ® ; Optifoam ® ; PolyMem ® ; Reston™; Sof-Foam™ | Bilaminate polyurethane or silicone | Semipermeable |
|
|
|
| Hydrogels |
| Hydrophilic polymer sheets, gel and impregnated dressings | Semipermeable with outer membrane in place |
|
|
|
| Alginates | AlgiCell ® ; AlgiDERM ® ; AlgiSite™ M; AlgiSorb ® ; Algosteril ® ; Fibracol ® Plus, a collagen (90%)–alginate (10%) dressing; Kalginate™; Kaltostat ® ; Maxorb ® ; Sorbsan ® | Seaweed-based complex polysaccharide | Semipermeable |
|
|
|
| Hydrocolloids | Allevyn™; Comfeel ® ; DuoDERM ® ; Exuderm ® ; Hydrocol ® II; N-Terface ® ; Nu-Derm ® ; Primacol ® ; RepliCare™; Sorbex ® ; Tegasorb™; Tielle™ | Starch or plastic woven polymer, dextran, polyethylene glycol, water | Semipermeable |
|
|
|
| Silicone dressings | Mepilex ® (foam); Mepitel ® (film); Mepilex ® Transfer (foam); Mepitel ® Border (foam) | Silicone-based | Semipermeable Suitable as primary or secondary dressings |
|
|
|
| Non-adherent dressings |
| Flexible polyester mesh | Non-adherent Non-occlusive |
|
| |
Films
Polymer films are thin, self-adhesive, transparent sheets of polyurethane or other synthetic semipermeable material ( Fig. 145.5 ). These dressings are gas permeable, allowing for the exchange of oxygen, carbon dioxide and water vapor, but impermeable to larger molecule efflux, due to their pore size. Therefore, bacteria, proteins and wound fluid are prevented from moving across the dressing. Its permeability to water vapor allows for the release of insensible water and sweat from the skin. This provides the potential advantage of preventing maceration of the wound and surrounding skin. The semi-occlusive nature of this dressing allows for passage of oxygen to the wound, which had been considered to be an important feature when these dressings were initially introduced. Since then, evidence has indicated that low pO 2 levels (similar to those that actually exist under the dressings) facilitate healing.

Advantages/disadvantages
The advantages of this type of dressing include translucency, thereby allowing direct visualization of the wound without removal of the dressing; permeability to water vapor; and tendency to reduce postoperative pain. It is also thought to enhance re-epithelialization of graft donor sites, with a reported increase in healing rates of 25–45% . One disadvantage of film dressings is that they are difficult to place properly, requiring uniform tension on the film to prevent wrinkling and its adherence to itself (similar to what is experienced with Saran™ Plastic Wrap). As the film usually only adheres to intact skin, a 1–2 cm application margin is recommended. In addition, due to shearing forces, it is best to avoid using films on thin or fragile skin.
Films may adhere to the wound as drying progresses, thereby risking disruption or stripping of the newly formed epithelium that is not yet tightly bound to the underlying dermal layer. It is also possible to traumatize newly grafted skin tissue during dressing changes. For these reasons, it is advisable to allow the film dressing to remain in place until it spontaneously falls off, which occurs after 1–2 weeks . Any wrinkling of the film during placement can create a conduit for bacterial penetration and leakage of wound exudate. It is therefore recommended that for exudative wounds the film have a complete 2–3 cm adhesion margin to prevent this leakage.
Another disadvantage of film dressings is that they are non-absorbent; therefore, wound fluid can accumulate under the dressing layer, especially with highly exudative wounds. This is often the case during the first 7–10 days after the creation of a wound, with the adherent properties of film dressings making frequent changing undesirable.
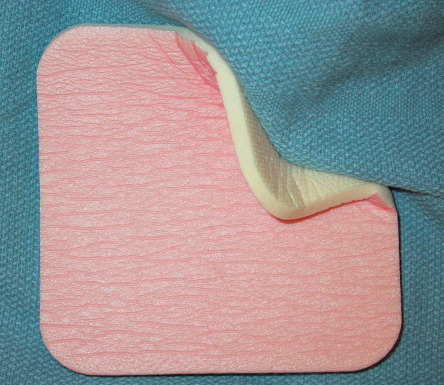
Foams
Polymer foams are semi-occlusive, bilaminate, and polyurethane- or silicone-based dressings. They consist of a hydrophilic foam with a hydrophobic backing, which can prevent leakage, provide a barrier against bacterial penetration, and provide the moist environment afforded by films, but with the addition of some absorbency ( Fig. 145.6 ). The inner layer is composed of an absorbent, gas-permeable polyurethane foam mesh, which lies adjacent to the wound. The outer layer is a semipermeable, non-absorbent membrane composed of polyurethane, polyester, silicone or Gore-Tex ® , surrounded by a polyoxyethylene glycol foam. This layer protects against outside bacterial contamination to some extent and against the drying out of the underlying layers.
Foam dressings are typically non-adherent, thereby requiring secondary dressing layers to ensure secure placement with a good seal. The quality of the seal is important to prevent leakage, desiccation, and problems with adherence. There are, however, some foams available with an adhesive surface, usually surrounding a central absorptive core. Ideally, once a foam dressing has absorbed some amount of exudate, it should be able to retain that fluid, even if exposed to pressure. Some brands are described as having such a quality.
Advantages/disadvantages
Although very absorbent, there is a limit to the amount of wound exudate this type of dressing can absorb. Therefore, it should be changed every 1–3 days. The permeability of foams to both gas and water vapor makes them suitable for mild to moderately exudative wounds, although there are brands designed for heavily exudative wounds.
Silicone-based rubber foams, known as silastic foams, are composed of a silicone mixture to which a stannous octoate catalyst has been added. This type molds and contours to the shape of the wound and therefore can be used for packing cavities or deep ulcers such as pilonidal sinuses. The additional advantages are absorbency, non-adherence, increased comfort for the patient, a tendency to be less expensive, and dressing changes that do not generally require skilled nursing care .
The disadvantages of foam dressings are the inability to use them with dry wounds, their opacity, which prevents visual monitoring of the wound, and the need for frequent changing, perhaps as often as every day. Infrequent changing could risk incorporation of the dressing material into the wound itself. There is also the possibility of an undesirable drying effect of the wound if drainage is insufficient to maintain a moist environment.
Hydrogels
As their name implies, hydrogels are composed primarily of water – up to 96% of the content. This dressing type consists of a cross-linked hydrophilic polymer network composed of polyvinyl alcohol, polyacrylamide, polyethylene oxide or polyvinyl pyrrolidone; it is produced as sheets, amorphous gels (pre-mixed or dry), or as impregnated dressings ( Fig. 145.7 ). Hydrogels are semitransparent (allowing visual inspection of the wound), have a high absorptive capacity (between 100% and 200% of their volume), and are able to maintain a moist wound environment. This absorptive action is delayed in its onset and increases slowly as it provides for continuous, long-term absorption. Hydrogels are described as semi-adherent or completely non-adherent, depending upon the type, and therefore require a secondary dressing to hold them in place . The latter is necessary, as hydrogels provide a poor bacterial barrier and selectively permit Gram-negative organisms to proliferate .

In general, the sheet form of a hydrogel dressing is constructed by sandwiching the hydrophilic polymer between two removable thin sheets of polyethylene film, with some types containing a supportive inner gel mesh. For application to the wound, the film on the contact side is removed, leaving the outer film in place. With this mode of application, the dressing is semipermeable to gases (including oxygen) and water vapor. If the outer film is also removed, then the dressing becomes permeable to fluid as well; as a result, exudate can pass to a secondary gauze dressing. The polymer sheets can be removed easily without trauma to the wound bed.
The amorphous type of hydrogel is composed of a cornstarch-derived, polymerized compound that forms a gel upon hydration at the time of its use. It is available commercially in a powdered or pre-mixed form, is applied wet to the wound defect, requires a secondary outer dressing, and requires water application to the surface for removal.
Advantages/disadvantages
One significant advantage of hydrogel dressings is a reduction in postoperative pain and inflammation. Another is that hydrogels have been shown to accelerate the rate of wound healing when compared to traditional Telfa TM and gauze dressings. For example, the rate of re-epithelialization of split-thickness porcine wounds was 25–45% faster with hydrogels and 100% of the hydrogel-treated wounds healed by postoperative day 4 compared with 32% of open-air (control) wounds . Hydrogels have also been credited with faster healing rates in studies of dermabrasion and hair transplant donor and recipient sites, when compared to standard Telfa TM and Adaptic TM dressings .
Hydrogels are not recommended for infected wounds. In addition, the semi- or non-adherent nature of hydrogels often results in more frequent dressing changes than is needed with other occlusive dressings.
Alginates
Highly absorbent alginate dressings are composed of a natural, complex polysaccharide derived from various types of algae or kelp (seaweed). An extraction process produces a sodium salt form of alginic acid and, during a second step, sodium ions are exchanged for calcium, zinc, and magnesium. The end result is an alginate fiber; non-woven mats or twists of this fiber are then made into a dressing ( Fig. 145.8 ). Upon application of the dressing, a reverse ion exchange occurs between the calcium within the alginate fibers and the sodium from blood or the wound exudate. This results in the formation of a soluble sodium alginate gel that fills and completely covers the wound in a non-adherent manner, providing a moist wound healing environment. The extent and rate of gel formation depends on the amount of wound exudate. Alginate dressing materials also have hemostatic properties, believed to be the result of the release of free calcium by the fibers during the ion exchange. This release of calcium augments the clotting cascade, producing the hemostatic advantage.

Because alginate gel dressings are highly absorbent, they can remain in place at the wound site for several days at a time, thereby minimizing dressing changes. To secure an alginate dressing, a secondary dressing is required. A dressing change is indicated when the dressing has been in place for several days or when exudate soaks through to the secondary dressing . Removal of the dressing in a dried state can re-injure the wound.
Advantages/disadvantages
Alginate dressings are soluble and can be removed by saline irrigation, permitting less painful dressing changes. They have been shown to encourage wound healing and are metabolized by the body, should residual material remain at the wound. Despite concerns about the potential toxicity of alginates, they have been used for over 50 years without any commonly reported complications. However, removal of the secondary outer dressing is necessary to visually inspect the wound and to monitor for desiccation.
Gelling fibers (Hydrofibers)
Highly absorptive hydrofibers are another category of dressings with similarities to alginates. They are composed of carboxymethyl cellulose fibers that interact with wound fluid, turn into a gel, and aid in autolytic debridement . Gelling fibers are up to three times more absorbent than alginates . An additional advantage over alginates is their vertical uptake of wound fluid, thereby decreasing the risk of periwound maceration.
Hydrocolloids
Colloid is a Greek term for a two-phase system comprised of a uniform dispersion of one phase of matter (unfilterable small particles) into another phase of matter or matrix. Mutually attractive charges exist between the particles, which contributes to the diffusible properties of colloids. Colloids are characterized by the strength of attraction of the particles to the continuous medium and to the proportion of water within that medium. This property accounts for the absorptive and expansive capacity of colloid gels, which function as a semipermeable membrane. Gel swelling occurs because the particle concentration of the gel is usually higher than that of the surrounding medium, thereby drawing water from the surroundings into the gel.
Hydrocolloid dressings were first employed as ostomy products and are now available in multiple forms. The most commonly used hydrocolloid dressings (e.g. DuoDERM ® ) are available as sheets with an inner adhesive layer consisting of a hydrophilic colloid base that is a mixture of pectin, karaya, guar or carboxymethyl cellulose plus an adhesive containing polyisobutylene, styrene isoprene, or ethylene vinyl acetate ( Fig. 145.9 ). The outer layer is composed of a thin semipermeable material such as polyurethane. A gel is formed in the presence of wound exudate, and as a unit, the dressing is semipermeable to water vapor and gases .

Another type of hydrocolloid dressing is a synthetic, non-adherent, high-density plastic woven polymer (e.g. N-Terface ® ). Fluid is able to flow through this matrix to be absorbed by an overlying dressing without adherence to the new epithelial surface.
Advantages/disadvantages
When in sheet form, these dressings can be cut and conformed to the shape of the wound. They are waterproof and adhere directly; as a result, they do not require a secondary dressing. In addition, these dressings have a cushioning or pressure-relieving effect (especially at bony sites), which increases as the dressing absorbs exudate. The resulting colloidal gel that forms prevents the dressing from adhering to the wound base. Accumulation of the exudate itself in a moist, semipermeable environment becomes a source of phagocytic cells and endogenous enzymes. This feature, along with the gel, results in autolytic debridement that can be washed away with saline irrigation of the wound bed . Because hydrocolloids are impermeable to water, oxygen and carbon dioxide, they are popular “waterproof” dressings .
Due to their semipermeable outer barrier, hydrocolloids have also been shown to stimulate angiogenesis and increase the rate of healing by as much as 40% when compared to open-air controls. A comparison of hydrocolloids versus wet-to-dry saline gauze dressings in the treatment of decubitus ulcers found that hydrocolloids do not require as many dressing changes as traditional wound dressings. Although the cost of individual hydrocolloid dressings was greater than gauze dressings and the healing rates were the same, the savings were in the cost of nursing time. In addition, the dressing changes tend to be simple and painless for the patient .
Disadvantages of hydrocolloids include maceration of the skin surrounding the wound, a potential for irritant or allergic contact dermatitis (e.g. to adhesives), and the risk of forming excessive granulation tissue. Similar to alginate dressings, the end product of hydrocolloids is a thick, yellow–brown, foul-smelling gel resembling purulent discharge . The patient needs to be educated regarding the distinction.
Composites
The designs of occlusive dressings are constantly changing with the goal of improved and simplified care for a greater range of wounds. Several new types of composite dressings, which combine two or more types of semi-occlusive dressings into one product, are commercially available. They have three components: (1) a semi- or non-adherent layer that contacts the wound (like a hydrogel, hydrocolloid, foam or alginate; Fig. 145.10 ); (2) an absorptive layer; and (3) an outer layer (like a film with an adhesive border). This maximizes the efficiency and comfort of the dressing by expanding absorbency as well as lessening the chance of maceration . Other features include the lack of need for secondary retention dressings and better waterproof coverings, which enable the patient to shower or bathe.