Disorders in the Newborn
Margarita Larralde
Paula C. Luna
Maria Eugenia Abad
Andrea Lorena Salavaggione
SCLEREMA NEONATORUM
Definition and Epidemiology
Sclerema neonatorum (SN) is a severe form of panniculitis characterized by diffuse hardening of the skin and subcutaneous tissues.1,2 SN is an extremely rare disorder mostly seen in critically ill preterm newborns in the setting of a wide variety of comorbidities like sepsis, congenital heart disease, pneumonitis, enteritis, hypothermia, hypocalcemia, and developmental anomalies.1,2,3,4,5
Etiology
Premature newborns have a higher ratio of saturated (stearic and palmitic acids) to unsaturated (oleic acid) fatty acids in their adipose tissue when compared with term healthy neonates. High concentration of saturated fat is associated with a high melting point and a low solidification point, a tendency to harden, and fat crystallization with temperature fall.2,4,5
Clinical Presentation
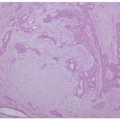
SN usually occurs in the first week of life but can develop immediately after birth or as late as several weeks of life. It is characterized by a hardening and thickening of the skin that begins on the thighs, buttocks, and trunk (Figure 2-1). The process rapidly progresses with diffuse woody induration of large body areas, resulting in difficulties with respiration, feeding, and movements. Fat-free areas like palms, soles, and genitalia are not affected. The prognosis is poor.1,2,3,5
Histologic Findings
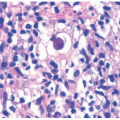
SN is characterized by a lobular lymphohistiocytic panniculitis1 (Figure 2-2). The epidermis and dermis are normal-appearing. The adipose tissue undergoes partial degeneration and formation of needle-like crystals with a radial arrangement toward the adipocytes. There is no significant necrosis or marked inflammation in the majority of cases. Some can have a thickening of the fibrous septa. Occasional multinucleated giant cells are present.1,2,3,4,5,6
Differential Diagnosis
Subcutaneous fat necrosis of the newborn (SCFN) shows a more pronounced inflammatory infiltrate. Admixed eosinophils are frequently seen. The crystals are seen in the adipocytes and macrophages. Case reports showing overlapping features of both SN and SCFN have been reported.7,8,9,10
 FIGURE 2-1. Sclerema neonatorum. |
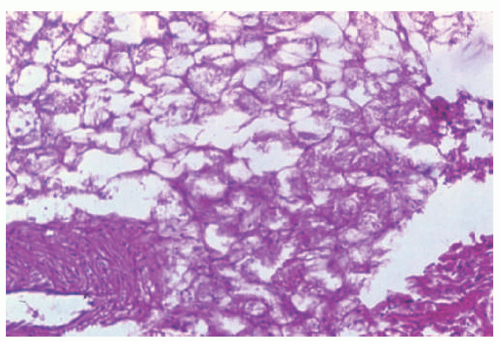 FIGURE 2-2. Sclerema neonatorum. The adipose tissue undergoes partial degeneration and formation of needle-like crystals with a radial arrangement toward the adipocytes. Courtesy of Dr. JW Patterson. University of Virginia. |
The other main differential diagnosis is scleredema. This occurs more frequently in preterm infants, usually during the first week of life, and is characterized by generalized firm, pitting edema, which is more common in lower extremities and manifests with an increase in the volume of the affected part. It is often preceded by cold injury, vomiting, diarrhea, or other acute infections. Body temperature is usually abnormal and the infant is apathetic. Histologically, there is a lobular panniculitis with the absence of vasculitis. There is a rich infiltrate of lymphocytes and histiocytes, and marked dermal edema. The edema can also extend to the adipose tissue and sometimes skeletal muscle.11
CAPSULE SUMMARY
SCLEREMA NEONATORUM
SN is a severe form of panniculitis characterized by a diffuse hardening of the skin and subcutaneous tissues. SN usually occurs in the first week of life but can develop immediately after birth or as late as several weeks of life. SN is characterized by a lobular lymphohistiocytic panniculitis. The adipose tissue undergoes partial degeneration and formation of needle-like crystals.
SUBCUTANEOUS FAT NECROSIS OF THE NEWBORN
Definition and Epidemiology
Subcutaneous fat necrosis of the newborn (SCFN) is a rare, transient, and self-limiting lobular panniculitis. SCFN usually affects term and postterm babies in the first week of life, with few cases developing as late as 6 weeks of age.12,13 Maternal risk factors to develop SCFN include preeclampsia, gestational diabetes, smoking or exposure to passive smoking, calcium channel blockers intake, and cocaine abuse. Neonatal risk factors include hypothermia, perinatal asphyxia, meconium aspiration, umbilical cord prolapse, obstetric trauma, and Rh incompatibility.7,8,14 SCFN was reported in 1% to 3% of newborns who underwent whole-body cooling for birth asphyxia.15,16,17
Etiology
Perinatal asphyxia induces blood shunt from skin to the brain and heart, leading to impaired tissue perfusion and local hypoxia. Neonatal fat tissue has a relatively high concentration of saturated fatty acids with a high melting point that predispose to solidify and crystallize under cold injury, resulting in adipocyte necrosis and subsequent formation of granulomatous inflammation.4,14,18,19
Clinical Presentation
SCFN is characterized by multiple indurated, erythematous, or violaceous painful nodules and plaques located on the cheeks, back, shoulders, extremities, and buttocks (Figure 2-2A-C). The anterior trunk is typically spared. Some lesions may become calcified or fluctuant with drainage of liquefied fat. Lesions resolve spontaneously within a few weeks, leaving in some cases atrophy, fibrosis, scarring, or necrosis. Although SCFN is a benign condition with an excellent prognosis, complications such as transitory hypoglycemia, hypertriglyceridemia, thrombocytopenia, and hypercalcemia have been reported.7,8,9,18
Histologic Findings
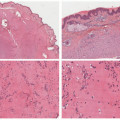
Biopsies of SCFN are characterized by a lobular panniculitis with a diffuse and brisk inflammatory infiltrate within the fat lobules (Figure 2-4). Necrosis of the adipocytes results in crystal formation and small granulomata surrounding the inflammatory cells.5,14,15,16,17,18,20,21,135,136,137,138,139 The crystals are needle-shaped and are present within the adipocytes and histiocytes. Abnormal eosinophilic granules can be present.22,140 Older lesions can show dystrophic calcification. Some cases can show a very rich acute neutrophilic inflammatory infiltrate and can mimic an infectious process. In the latter, neutrophilic represented more than 75% of the cells in the infiltrate.23,141
Differential Diagnosis
The main differential diagnosis is with SN. Subcutaneous fat necrosis of the newborn shows a more pronounced inflammatory infiltrate. Admixed eosinophils are frequently seen.
 FIGURE 2-3. Subcutaneous fat necrosis. A, Extensive erythematous plaque over the back of a term newborn. B, Erythemo-edematous plaque over the back and shoulder. C, Well-circumscribed plaque over the shoulder. |
CAPSULE SUMMARY
SUBCUTANEOUS FAT NECROSIS
This is a rare, transient, and self-limiting lobular panniculitis. SCFN usually affects term and postterm babies in the first week of life, with a few cases developing as late as 6 weeks of age. It is characterized by multiple indurated, erythematous, or violaceous painful nodules and plaques located on the cheeks, back, shoulders, extremities, and buttocks. Biopsies of SCFN are characterized by a lobular panniculitis with a diffuse and brisk inflammatory infiltrate within the fat lobules. Necrosis of the adipocytes results in crystal formation and small granulomata surrounding the inflammatory cells.
Milia and Miliaria
MILIA
Definition and Epidemiology
Milia is a common condition of the newborn that may be due to several causes can be found alone or associated with other diseases. These lesions affect up to 83% of newborns. Milia is a common condition of the newborn that may be due to several causes, can be found alone or associated with other diseases, and affects up to 83% of babies.
Etiology
Milia is divided into primary milia (when occurs spontaneously) or secondary milia (when develops after healing of a previous skin condition). Lesions usually appear and
disappear spontaneously during the first month of life. In some cases, milia may be more persistent.20
disappear spontaneously during the first month of life. In some cases, milia may be more persistent.20
 FIGURE 2-4. Subcutaneous fat necrosis of a newborn. Biopsy shows a lobular panniculitis (A). Necrosis of the adipocytes results in crystal formation and small granulomata surrounding the inflammatory cells (B and C). The crystals are needle-shaped and are present within the adipocytes and histiocytes (D). Digital slides courtesy of Path Presenter.com. |
Clinical Presentation
The clinical lesions of milia include pearly, superficial, firm papules that mainly affect the nose, cheeks, chin, and forehead (Figure 2-5A and B).21,22 Lesions can vary from a single cyst to hundreds, and also vary in size, with larger lesions usually affecting foreskin, areolae, scrotum, and labia majora.23 When milia are numerous and persistent, different types of genodermatoses should be considered (Figure 2-6).20,24 A large congenital, milia-like, papule in the midline anterior neck (Figure 2-7) has been recently reported by Walsh et al25 as “MANIC (Midline Anterior Neck Inclusion Cyst);”
it is postulated to be a forme fruste of a midline fusion developmental defect. The histology is indistinguishable from large milia.
it is postulated to be a forme fruste of a midline fusion developmental defect. The histology is indistinguishable from large milia.
 FIGURE 2-5. Milia. A, Multiple pinpoint white papules over the face and one isolated lesion on the chest. B, Scattered white papules over the face. |
 FIGURE 2-6. Profuse congenital facial milia in a baby with Basan syndrome. |
Histologic Findings
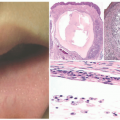
It is thought that primary milia arise from the pilosebaceous units and the secondary forms from the sweat ducts. These two subtypes can be distinguished on the basis of the histopathologic findings. Primary milia resemble small follicular cysts derived from the follicle infundibulum (Figure 2-8). The cysts are lined by atrophic squamous epithelium that contain a granular cell layer and show loose keratin contents. Secondary milia are also cystically dilated spaces, but are lined by ductal epithelium (eccrine). Serial sectioning can easily demonstrate the connection of the cysts to the sweat duct in most cases.24,26,27,28,142
Differential Diagnosis
Differential diagnostic considerations will include vellus hair cysts. Those can also be multiple, and only rarely present in the newborns or shortly thereafter.29,143 The vellus hair cysts show a similar lining epithelium, but contain vellus hairs admixed with the loose keratinous debris. Apocrine hidrocystomas can also be multiple and be present in a congenital fashion.30,144 The difference is that the lining shows plumped columnar epithelioid cells with apocrine decapitation.
 FIGURE 2-7. Midline anterior neck inclusion cyst. |
CAPSULE SUMMARY
MILIA
Milia is a common condition seen in the newborn population that may be due to several causes. It can occur in isolation, or be associated with other conditions. These lesions may affect up to 83% of newborns. Primary milia resemble small follicular cysts derived from the follicle infundibulum. Secondary milia are also cystically dilated spaces, but are lined by ductal epithelium (eccrine).
MILIARIA
Definition and Epidemiology
Miliaria is a term used to describe the obstruction of the eccrine ducts that may occur at different levels of the apparatus. Although it may appear at any age, it is particularly frequent in neonates, affecting around 1% to 15% of newborns, especially in warm climates.
Etiology
Miliaria is caused by the extravasation of sweat into the skin because of obstruction and rupture of the eccrine duct. It can be classified into miliaria crystallina or sudamina (with the obstruction located at the stratum corneum) and miliaria rubra, which is caused by a deeper type of obstruction (intraepidermal) with secondary local inflammation. Miliaria profunda is extremely rare in neonates and is the deepest type of miliaria.26,27
Clinical Presentation
In miliaria crystallina, lesions are fragile, pinpoint, clear, superficial vesicles over a noninflammatory skin, affecting mainly the forehead and upper trunk appearing during the first week of life.27 Miliaria rubra lesions are erythematous nonfollicular papules, pustules, and vesicles. It usually affects the face, neck, and trunk during the second week of life (Figure 2-9).
Miliaria profunda shows a great amount of inflammation, and lesions are deeply situated in the dermis and are intensely red.
Histologic Findings
Miliaria is characterized by a disruption of the sweat ducts at various levels throughout the outflow tract with extravasation of the secretions (Figure 2-10). The specific
site of disruption is associated with a diversity of clinical and histologic findings.31,32,33,145,146,147 Miliaria crystallina is associated with the occlusion at the closest proximity to the surface epidermis. In this form, the secretion is present at the level of the acrosyringia within the stratum corneum. The result is the presence of acrosyringial spongiosis and intracorneal fluid collection. Inflammation is typically minimal or absent. When present, neutrophils are the predominant type of inflammatory cell. In Miliaria rubra, the secretion occurs in the intraepidermal portion of the eccrine duct. Spongiosis is more prominent, but dermal inflammation is also present. Miliaria profunda is the deepest form of this entity, occurring within the dermis. A lymphocytic infiltrate can be present. In rare occasions, large areas of miliaria profunda present as dermal plaques, and the histopathology includes a granulomatous reaction to the extravasated secretions.34,148
site of disruption is associated with a diversity of clinical and histologic findings.31,32,33,145,146,147 Miliaria crystallina is associated with the occlusion at the closest proximity to the surface epidermis. In this form, the secretion is present at the level of the acrosyringia within the stratum corneum. The result is the presence of acrosyringial spongiosis and intracorneal fluid collection. Inflammation is typically minimal or absent. When present, neutrophils are the predominant type of inflammatory cell. In Miliaria rubra, the secretion occurs in the intraepidermal portion of the eccrine duct. Spongiosis is more prominent, but dermal inflammation is also present. Miliaria profunda is the deepest form of this entity, occurring within the dermis. A lymphocytic infiltrate can be present. In rare occasions, large areas of miliaria profunda present as dermal plaques, and the histopathology includes a granulomatous reaction to the extravasated secretions.34,148
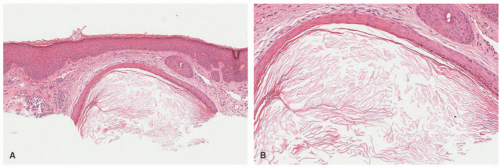 FIGURE 2-8. Milia: The cysts are lined by atrophic squamous epithelium that contain a granular cell layer and show loose keratin contents (A and B). Digital slides courtesy of Path Presenter.com. |
Differential Diagnosis
The spongiosis of miliaria is different from other spongiotic reactions, because it is typically more pronounced at the level of acrosyringium. However, when severe, it can be more diffuse and potentially mimic eczematous reactions. Erythema toxicum neonatorum (see below) can sometimes resemble miliaria clinically. Histologically, the former has intracorneal or intraepidermal pustules. Eosinophilic folliculitis can also resemble miliaria clinically, but it is associated with a follicular-based inflammatory infiltrate, with eosinophils extending into the hair follicle epithelium.
 FIGURE 2-9. Miliaria pustulosa over the back navel of a 3-month-old. |
CAPSULE SUMMARY
MILIARIA
Miliaria is a term used to describe the obstruction of the eccrine ducts that may occur at different levels. Miliaria is characterized by a disruption of the sweat ducts at various levels throughout the outflow tract with extravasation of secretions. The specific site of disruption is associated with a diversity of clinical and histologic findings.
ERYTHEMA TOXICUM NEONATORUM
Definition and Epidemiology
Erythema toxicum neonatorum (ETN) is a common, benign, and transient condition of healthy neonates. ETN is very frequent in full-term neonates, an incidence varying from 3.7% to 72%.29,30,31,32 There is no gender or racial predilection. Higher incidence rates are seen in term healthy neonates born after a normal pregnancy with a birth weight of over 2500 g.32 It is rarely seen in preterm infants with low birth weight.26
Etiology
The etiopathogenesis of ETN is still unclear. The identification of proinflammatory mediators aquaporin-1,
aquaporin-3, eotaxin, interleukin-1, interleukin-8, and psoriasin and nitric oxide synthases 1, 2, and 3 in the ETN infiltrate supports the current theory that ETN is an immunologic cutaneous response to microbial skin and hair follicles colonization from the first day of life.29,32,33
aquaporin-3, eotaxin, interleukin-1, interleukin-8, and psoriasin and nitric oxide synthases 1, 2, and 3 in the ETN infiltrate supports the current theory that ETN is an immunologic cutaneous response to microbial skin and hair follicles colonization from the first day of life.29,32,33
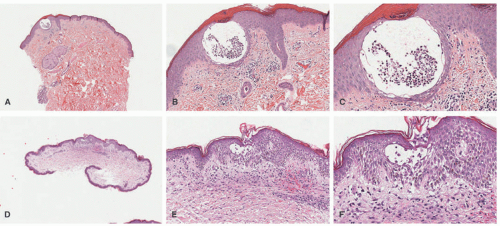 FIGURE 2-10. Miliaria crystallina is associated with occlusion at the closest proximity to the surface epidermis. In this form, the secretion is present at the level of the acrosyringia within the stratum corneum. Neutrophils are seen in the vesicle (A to C). In Miliaria rubra, the secretion occurs in the intraepidermal portion of the eccrine duct. Spongiosis is more prominent, and dermal inflammation is also present. (D to F). Digital slides courtesy of Path Presenter.com. |
Clinical Presentation
Skin lesions of ETN most commonly present at 24 to 72 hours of life, but can occur since birth to 2 weeks of age, resolving in 5 to 7 days without sequelae. The occurrence may occasionally be delayed for a few days in premature neonates.26,31 It is characterized clinically by asymptomatic erythematous macules and wheals (Figure 2-11), ranging from a few millimeters to several centimeters in diameter, centered by a papule or pustule (Figure 2-12). Lesions typically occur on the face, trunk, proximal limbs, and buttocks, whereas palms, soles, and genitalia are usually spared.26,31,34 Lesions can vary from few to several in number, and new ones may appear during the first few days of life as the eruption waxes and wanes; recurrences may occur in up to 11% of neonates.26,31
 FIGURE 2-11. Erythema toxicum neonatorum. Papules and erythema over the back of a newborn. |
 FIGURE 2-12. Erythema toxicum neonatorum. Erythema and overlying papules over the back of a boy. |
Histologic Findings
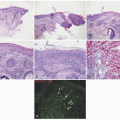
Biopsies of ETN show subcorneal or intraepidermal pustules of eosinophils, and a marked inflammatory infiltrate within the pilosebaceous unit, usually just deep to the dermal-epidermal junction. Inflammation in the dermis can also be present (Figure 2-13A to D). Scattered dermal eosinophils are seen. Some have suggested that ETN and transient neonatal pustular melanosis are closely related entities.35,36,149,150
CAPSULE SUMMARY
ERYTHEMA TOXICUM NEONATORUM
ETN is a common, early occurring eruption in full-term neonates characterized by asymptomatic erythematous macules and wheals, ranging from a few millimeters to several centimeters in diameter, centered by a papule or pustule. Biopsies of ETN show subcorneal or intraepidermal pustules of eosinophils, and a marked inflammatory infiltrate within the pilosebaceous unit.
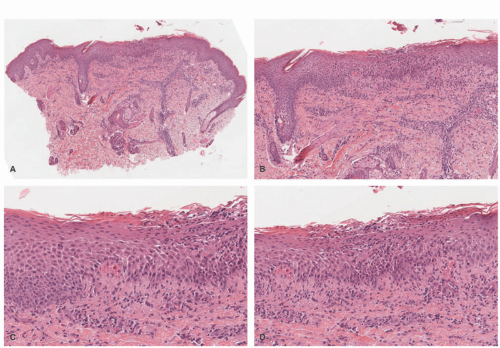 FIGURE 2-13. Erythema toxicum neonatorum. Biopsies show subcorneal or intraepidermal pustules of eosinophils and a marked inflammatory infiltrate within the pilosebaceous unit, usually just deep to the dermal-epidermal junction (A-D). Digital slides courtesy of Path Presenter.com. |
EOSINOPHILIC PUSTULAR FOLLICULITIS
Definition and Epidemiology
Eosinophilic pustular folliculitis (EPF) is an uncommon condition first described in adults mainly associated with HIV infection. Its pediatric variant, EPF of infancy, was first described by Lucky et al.35 It consists of intensely pruritic crusted papules affecting mainly the scalp. The infantile variant is typically not associated with HIV, but with different hypereosinophilic states. Few cases have been reported occurring since birth or in the first few days of life. It is more frequent in males than in females.
Etiology
The exact etiology of this condition remains unknown. Given its histologic similarities to ETN, it has been suggested that this entity might represent a severe and persistent type of ETN.36 A relation to hypereosinophilic states, as well as its manifestation in patients with hyper Immunoglobulin E (IgE) syndrome, has also been suggested in a few number of patients.
Clinical Presentation
It is characterized by the presence of 1 to 3 mm pustules and crusts on the scalp and face (Figures 2-14 and 2-15), but also on the trunk and extremities.35,36,37,38,39,40,41 Lesions typically appear in crops, with a waxing and waning course lasting from days to weeks; most severe cases might last several years, always healing without scarring.39 Most cases resolve completely by age 3. Pruritus or irritability is a very common feature, in more than 77 percent of patients. Peripheral eosinophilia is present in many patients. Because this eruption has been described in patients who later developed a hyper IgE syndrome, a close follow-up of these neonates is recommended.(41,42,43,44,45,46)
Histologic Findings
It is important to obtain an entire papule or pustule with associated follicle during a biopsy to ensure an adequate sample for histologic examination and diagnosis. Because eosinophilic folliculitis is a folliculocentric finding, one may need to do serial sections to catch the inflamed hair follicle (Figure 2-16). An examination of unexcoriated, fresh papulopustules shows an acute and chronic infiltrate of eosinophils and lymphocytes focused at the level of the follicular isthmus that may rarely progress to complete follicle destruction. One sees eosinophils along with scattered mononuclear cells and neutrophils in the pilar outer root sheath and sebaceous glands and ducts. Perifollicular and perivascular eosinophilic invasion can be observed. In some cases, eosinophilic flame figures are present.37,38,39,40
Differential Diagnosis
EPF must be distinguished from other infectious and noninfectious pustular disorders in childhood: ETN, transient pustular melanosis, scabies, miliaria pustulosa, infections, acropustulosis of infancy, arthropod bites, and Langerhans cell histiocytosis. ETN and TNPM (Transient Neonatal Pustular Melanosis) are not typically folliculocentric processes. Scabies can be easily distinguished by the presence of scabies mites. Miliaria pustulosa is associated with an acrosyringial pattern of spongiosis with subsequent superinfection. Acropustulosis of infancy is also similar to ETN in terms of lack of folliculocentrism and is more acral in distribution. Langerhans cell histiocytosis is often folliculocentric and can show a large number of eosinophils. The main feature of Langerhans cell histiocytosis is the presence of an atypical population of Langerhans cells (demonstrated by S100, CD1a, and Langerin immunostains) that is epidermotropic, a feature that is missing in EPF.
 FIGURE 2-14. Vesico pustules over the cheek of a patient with eosinophilic pustular folliculitis. |
 FIGURE 2-15. Widespread crusts and erosions over the scalp and erythematous papules over the back of a patient with eosinophilic pustular folliculitis who later developed a hyper immunoglobulin E syndrome. |
CAPSULE SUMMARY
EOSINOPHILIC PUSTULAR FOLLICULITIS
ETN consists of intensely pruritic crusted papules affecting mainly the scalp. The infantile variant is typically not associated with HIV, but with different hypereosinophilic states. It is characterized by the presence of 1 to 3 mm pustules and crusts on the scalp and face. Biopsies show a folliculitis with a predominance of eosinophils.
TRANSIENT NEONATAL PUSTULAR MELANOSIS
Definition and Epidemiology
Transient neonatal pustular melanosis (TNPM) is a very infrequent, benign, self-healing condition that mainly affects full-term neonates.47,48 It is thought to affect around 0.6% of Caucasians, with a higher incidence in African American newborns (4.4%).
 FIGURE 2-16. Eosinophilic pustular folliculitis with numerous eosinophils infiltrating into the hair follicle epithelium (A-C). Digital slides courtesy of Path Presenter.com. |
Etiology
The etiology of this condition is still unknown, but some authors have suggested it might be an early manifestation of ETN because of its clinical and histologic overlap.
Clinical Presentation
Three different types of lesions can be identified—pustules that easily break and leave a fine white collarette of scale, and a hyperpigmented macule. Lesions appear usually over a normal skin and can be found in clusters or scattered around different parts of the body, including genitals, scalp (Figure 2-17A to C), palms, and soles.49 The most important differential diagnoses include ETN, bacterial, viral, and mycotic infections, miliaria, and eosinophilic pustulosis. Under some circumstances, a clear-cut differentiation between TNPM and ETN might be really impossible.
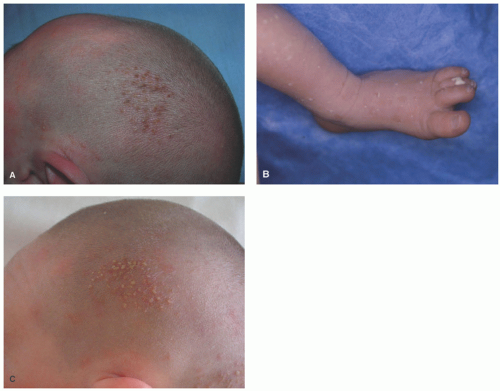 FIGURE 2-17. A, Transient neonatal pustular dermatosis—a crop of congenital pustules over the scalp of a term newborn. B, Evolution of lesions showing hyperpigmentation and scale 2 days later. C, The three coexistent states of transient neonatal pustular dermatosis: pustules, scaling, and hyperpigmentation. |
Histologic Findings
Differential Diagnosis
Differential diagnostic considerations include pustular psoriasis. The latter is very uncommon in neonates, and can be easily distinguished on the basis of the presence of other clinical findings. ETN is characterized by eosinophils in the pustules, as opposed to TNPM, where the main inflammatory cell is neutrophils in the pustules. Some authors consider that TNPM represent a precursor lesion to what rapidly evolves into ETN.35,41,50,51
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


