Dermatofibroma
Adriane M. Boyle
I. BACKGROUND
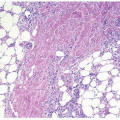
A dermatofibroma (benign fibrous histiocytoma) is a benign growth of dermal fibroblasts. Dermatofibromas are common and are often overlooked by patients as they mimic nevi and other benign skin growths. Their cause is unknown, but they are thought to arise from an antecedent arthropod bite, folliculitis, trauma, or other inflammatory insult. Multiple dermatofibromas may occur in association with lupus or immunosuppression.
II. CLINICAL PRESENTATION
Dermatofibromas most frequently occur in young- to middle-aged adults and are more common in women. They are typically located on exposed areas of the extremities, especially the legs, but can occur on the torso and the head. Although often asymptomatic there can be associated pruritus or pain, and they typically do not continue to grow after reaching a stable size. Prior history of trauma or arthropod bite in the area may be reported by the patient but is not required for the diagnosis.
Physical examination of a dermatofibroma is often diagnostic and reveals a very firm, brown to red-brown, <1 cm, round papule or nodule (Fig. 10-1). Uncommon variants include multiple clustered dermatofibromas in children, and a giant dermatofibroma mimicking a malignant tumor. As dermatofibromas are frequently hyperpigmented, they can be confused with more concerning pigmented lesions such as atypical nevi and melanoma (Fig. 10-2). Clues to help the clinician differentiate dermatofibromas from other lesions include the firmness of the lesion upon palpation, the “dimple” sign (Fig. 10-3), and a typical dermoscopic pattern of a central white patch with peripheral pigment network. Infrequently overlying sebaceous hyperplasia may be noted, and if located in an atypical site for sebaceous glands, this can be a clue to the diagnosis of dermatofibroma.1
III. WORKUP
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


