Dermatitis (eczema) refers to a heterogeneous group of disorders that share similarities in clinical appearance and histopathologic findings, but may have very different etiologies. Eczema originates from a Greek word meaning “to boil.” Acute dermatitis often appears vesicular (like water boiling on the skin), whereas chronic dermatitis may be red, scaly, and lichenified. Pruritus is a common symptom of all types of dermatitis.
The 2 major types of contact dermatitis are irritant contact dermatitis and allergic contact dermatitis. These reactions are not mutually exclusive, and may occur simultaneously in a particular patient. For example, contact allergy to a glove chemical may complicate irritant hand dermatitis due to irritating soaps used for hand washing. Furthermore, one substance may act as both an irritant and an allergen; a patient may have an allergic reaction to a preservative in a liquid soap as well as having an irritant reaction to a detergent in a soap. Common allergens include urushiol (eg, poison ivy), nickel, fragrances, preservatives, topical antibiotics (eg, neomycin, bacitracin), and paraphenylenediamine (eg, black hair dye). Common irritants include water, soap, industrial cleansers, and frictional forces.
Irritant contact dermatitis is the most common form of contact dermatitis. It is estimated that irritant contact dermatitis represents approximately 80% of occupational contact dermatitis. Occupations at high risk include those involving repeated exposure to water and/or soap (wet work) such as health care workers, janitorial services, and food industry employees or those involving exposure to solvents such as machinists.1
Irritant contact dermatitis is a nonimmunologic response to chemicals or physical agents such as friction that disrupt the normal epidermal barrier. Strong irritants include acids and alkalis, whereas weak irritants include soaps and cleansers. Damaged skin lacks the proper oils and moisture, thus allowing irritants to penetrate more deeply and cause further damage by triggering inflammation. Any condition that impairs skin barrier function, such as atopic dermatitis or asteatotic dermatitis/dry skin, is a risk factor for developing irritant contact dermatitis.
Irritant contact dermatitis typically develops weeks after exposure to weak irritants such as hand soap or immediately after exposure to strong irritants such as bleach. It may affect any individual, given sufficient exposure to irritants, but those with a history of atopic dermatitis are at higher risk because of disruption of the normal epidermal barrier. Pruritus, pain, and burning are common symptoms.
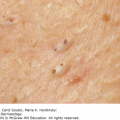
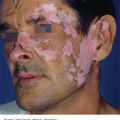
Irritant contact dermatitis is often well demarcated with a glazed appearance, but there may also be erythema, swelling, blistering, and scaling. Initially, irritant reactions are usually confined to the site of contact with the irritant. The most common locations are hands, forearms, eyelids, and face (Figures 8-1, 8-2, 8-3).



Skin biopsies are usually not diagnostic and are only helpful to rule out noneczematous conditions such as psoriasis. Skin scrapings for fungal elements or a scabies preparation will rule out those conditions.
Irritant contact dermatitis is a diagnosis of exclusion. The typical patient presents with pruritic or painful dermatitis beginning approximately 3 months after low-grade irritant exposure (eg, hand dermatitis in a nursing student) or shortly after exposure to a strong irritant or frictional exposure.
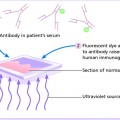
✓ Allergic contact dermatitis: This may appear identical to irritant contact dermatitis. Allergic contact dermatitis is diagnosed by patch testing.
✓ Atopic dermatitis: Individuals with atopic dermatitis usually have a personal or family history of atopic dermatitis (childhood eczema), allergic rhinitis, or asthma.
✓ Cutaneous fungal infections: Tinea infections present with annular plaques with a scaly border. Fungal hyphae causing tinea (corporis, manus, cruris, pedis) can be visualized on a potassium hydroxide (KOH) preparation from skin scrapings.
✓ Other eczematous skin conditions: Nummular dermatitis, dyshidrotic eczema, and lichen simplex chronicus.
✓ Uncommon conditions: Cutaneous T-cell lymphoma.
The management of irritant contact dermatitis is 2-fold:
| Irritant | Examples of Common Sources |
|---|---|
| Acids | Organic acids (eg, chromic, formic, hydrochloric, hydrofluoric, nitric, oxalic, sulfuric) |
| Alcohols | Antiseptics, waterless hand cleansers |
| Alkalis | Organic alkalis (eg, calcium oxide and potassium and sodium hydroxide) |
| Body fluids | Urine, feces, saliva |
| Concrete | Wet cement |
| Detergents | Hand soap, shampoo, dish detergents |
| Fiberglass | Insulation |
| Food | Fruit acids, meat enzymes, proteins, vinegar |
| Metal salts | Metal working, pulp, steel, and paper manufacturing |
| Physical agents | Temperature extremes, friction, humidity |
| Plastic resins | Unpolymerized monomers in plastic industries |
| Solvents | Turpentine, gasoline, kerosene, benzene |
Mild soaps and moisturizers listed in Table 8-2 should be used. For irritant hand dermatitis, vinyl gloves should be worn as a barrier to unavoidable irritant exposures such as dish soap and juice from citrus fruits. Cotton gloves over a heavy emollient such as petroleum jelly overnight may also be helpful.2 Each water exposure should be immediately followed by application of an emollient to prevent dehydration of the skin and restore the normal skin barrier. For cracks and fissures, application of superglue as a sealant may also be helpful. Mid-potency topical corticosteroid ointments or creams may be used twice a day as needed to treat symptoms as adjunctive therapy to aggressive moisturization (Table 8-3).
Moisturizers
|
Cleansers
|
| Class | Potency | Generic Name | Trade Name Examples | Formulations |
|---|---|---|---|---|
| 1 | Superpotent | Clobetasol propionate | Temovate | Cream, gel ointment, solution 0.05% |
| 2-3 | High potency | Fluocinonide | Lidex | Cream, gel ointment, solution 0.05% |
| 4-5 | Medium-potency | Triamcinalone acetonide Fluocinolone acetonide | Synalar | Cream, ointment 0.1% Ointment 0.025% Cream, ointment 0.025% |
| 6 | Low potency | Fluocinolone acetonide Desonide | Derma-Smoothe FS Desowen | Oil, solution 0.01% Cream, ointment 0.05% |
| 7 | Least potent | Hydrocortisone acetate | Cortaid | Cream, ointment 1% and 2.5% |
Severe or persistent disease that does not respond to treatment.
National Eczema Association: www.nationaleczema.org/living-with-eczema/hand-eczema
The most common allergen causing allergic contact dermatitis in the United States is urushiol, found in poison ivy, oak, and sumac. Of individuals patch tested by specialists in North America, the most common allergens include:
Metals (eg, nickel 19%; cobalt 8%; chromate 5%)
Fragrances (eg, balsam of Peru 12%; fragrance mix 12%)
Preservatives (eg, quaternium-15 10%)
Topical antibiotics (eg, neomycin 10%; bacitracin 9%)3
Allergic contact dermatitis is a cell-mediated, delayed, type IV hypersensitivity reaction, resulting from contact with a specific allergen to which a patient has developed a specific sensitivity. There are 2 main steps in developing allergic contact dermatitis: induction and elicitation. During the induction phase, also known as sensitization, an allergen penetrates the epidermis and is processed by antigen-presenting cells (Langerhans cells, dendritic cells, and macrophages) and presented to T lymphocytes. This initial phase generally takes between 10 and 14 days. In the elicitation phase, reexposure to the allergen causes activation of circulating effector T lymphocytes, which produce cytokines resulting in an inflammatory response.4 Clinical manifestations usually occur within hours to days after allergen exposure. After removal of the allergen, allergic contact dermatitis typically persists for up to 3 weeks.
The patient usually complains of an intensely pruritic rash at the site of contact with the allergen.
Acute allergic contact dermatitis classically presents as papules and vesicles on an erythematous base (Figures 8-4 and 8-5).
Chronic allergic contact dermatitis may manifest as xerosis, fissuring, and lichenified eczematous plaques.


In general, allergic contact dermatitis occurs at the site of contact with the allergen. Nickel allergy usually results in dermatitis underlying nickel-containing objects (Figure 8-6) (eg, jewelry—earlobes, neck, wrists; belt buckles—umbilicus; cell phones—cheeks). However, dermatitis in certain sites, especially the eyelids and face, may result from contact to allergens on the hands (fingernail polish) or scalp (hair products). Table 8-4 lists common allergens at selected body sites.

| Body Site | Common Sources and Responsible Allergens |
|---|---|
| All locations | Topical preparations (bacitracin, neomycin, corticosteroids, preservatives, emulsifiers) Personal care products (preservatives, emulsifiers) |
| Face | Cosmetics, personal care products (emulsifiers, preservatives) Hair products (surfactants, fragrances, preservatives) Cell phones, eyeglasses, headsets (nickel) Consort/connubial contact from spouse/partner’s products |
| Eyelids | Cosmetics (emulsifiers, preservatives) Nail polish (toluene sulfonamide resin) Artificial nails (acrylates) Eyelash curlers, tweezers (nickel) Jewelry (gold—may cause a distant allergic contact dermatitis) Eye drops (active ingredients, preservatives) |
| Hands | Gloves (rubber accelerators, leather tanning agents) Hand soap/sanitizers (fragrance, antibacterial agents, surfactants) Tools/utensils (rubber, metals) Occupation-specific chemicals (eg, hairdressers—hair dye) |
| Neck, shoulders | Jewelry (nickel, cobalt, gold) Hair products (surfactants, fragrances, preservatives) |
| Feet | Shoes (rubber accelerators, leather tanning agents, glue ingredients) |
| Under clothing only | Clothing dye (disperse blue dyes) Clothing finishes (formaldehyde resins) |
Skin biopsies are usually not diagnostic and are only helpful to rule out noneczematous conditions such as psoriasis. Skin scrapings for fungal elements or a scabies preparation will rule out those conditions.
The key diagnostic features of allergic contact dermatitis are pruritic vesicles or scaly, lichenified plaques that correspond to the area of contact with the allergen.
Pruritus should always be present in allergic contact dermatitis. The presence or history of vesicles is helpful in confirming the diagnosis, although this is not solely specific for allergic contact dermatitis.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


