Large, full-thickness calvarial defects present a series of significant reconstructive challenges involving a range of techniques, including local and free flaps. Occasionally these conventional methods may not be possible due to technical, or patient, factors. Artificial dermis is already widely used in burns surgery and is increasing in oncological reconstruction. We believe that artificial dermis coupled with split-thickness skin grafting provides an excellent option for closure of these defects when other techniques are not appropriate.
The successful use of artificial dermal substitute has been well reported in the management and reconstruction of burns, and is becoming more common in general reconstruction and after oncological resection. Studies have documented the use of artificial dermis for partial and full-thickness soft tissue scalp defects, and one institution has described the use of Integra Bilayer Matrix Wound Dressing directly onto dura.
We present the case of a 91-year-old lady with a history of four separate skin tumours of the scalp over the period of ten years, each of which underwent excision and differing methods of reconstruction. Two of these tumours necessitated full-thickness calvarial excision and resurfacing with either split skin grafting alone, or with split skin grafting and dermal substitute. We have found that artificial dermis along with split-thickness skin grafting provides an excellent option for closure of full-thickness calvarial defects. It offers an extra layer for dural protection and gives a better cosmetic result, whilst avoiding the invasive nature and prolonged recovery of other techniques.
Case report
A 91-year-old lady presented with a seven-month history of recurrent basal cell carcinoma (BCC) on the vertex of the scalp following excision some years previously. This patient had a history of three other skin tumours of the scalp, all of which required operative treatment and reconstruction over the last ten years.
The first tumour, approximately ten years ago, was a noninvasive BCC of the left frontal scalp. This was completely excised and the area resurfaced successfully using a split skin graft. The second tumour was an adherent, locally invasive squamous cell carcinoma (SCC) of the right frontal scalp which was excised along with the outer table of calvarium. The defect was covered with a split skin graft directly to the inner calvarial table with good results.
Five years ago, in 2005, the patient underwent extensive surgery for a further infiltrative SCC on the right parietal scalp with bony involvement. The tumour was excised along with the full-thickness of the calvarium and closed using a split-thickness skin graft directly on to dura. The procedure pre-dated the introduction of artificial dermis in oncological reconstruction, and the presence of a skin graft and scarring from prior scalp surgery meant that local flap reconstruction was not practical.
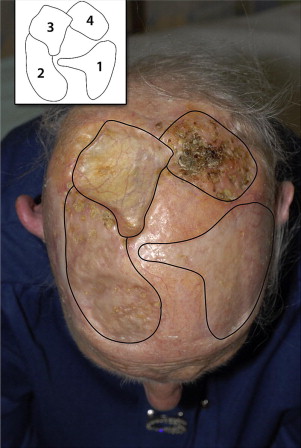
Physical examination revealed a nodular cutaneous lesion approximately 4 × 4 cm with irregular edges, crusting and telangectasia on the vertex of the scalp, to the left of mid-line. There was also a 5 × 5 cm discoid defect to the right of mid-line from the earlier SCC excision and reconstruction, and two further defects over the frontal region from previous surgery ( Fig. 1 ). Tissue biopsy of the left-sided parietal lesion confirmed the presence of recurrent BCC and a cranial bone biopsy deep to the lesion revealed extensive bony infiltration with tumour penetrating almost the full thickness of the calvarium. A computed tomography (CT) head scan was performed which demonstrated the previous calvarial defect and showed no evidence of intracranial contrast-enhancing lesions.
Related posts:
 Stiffening of Human Skin Fibroblasts with Age
Stiffening of Human Skin Fibroblasts with Age
 Physiology of Skin Aging
Tissue Engineering of Skin
Management of Split Skin Graft Donor Sites–Results of a National Survey
Physiology of Skin Aging
Tissue Engineering of Skin
Management of Split Skin Graft Donor Sites–Results of a National Survey
 Management of Wounds with Exposed Bone Structures using an Artificial Dermis and Skin Grafting Technique
Skin: Histology and Physiology of Wound Healing
Management of Wounds with Exposed Bone Structures using an Artificial Dermis and Skin Grafting Technique
Skin: Histology and Physiology of Wound Healing
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


