Key Words
breast reconstruction, implant, delayed, two-stage, muscle coverage
Disclosure : The authors have no financial interest to declare in relation to the drugs, devices, and products mentioned in this article.
Introduction
Implant-based breast reconstruction can also occur in a two-stage delayed approach after the primary mastectomy has been completed. Traditionally, delayed breast reconstruction often involves autologous tissue options due to the association with adjuvant radiation and the subsequent need for distant healthy tissue to recreate the breast. However, the use of tissue expanders in a two-stage approach can also be performed safely with appropriate patient selection especially if the patient does not need postoperative radiation.
Some women may choose to forego any decision for breast reconstruction prior to their oncologic surgery or may change their mind later. In these cases, the patient can be served with a two-stage total muscle coverage implant-based reconstruction.
In this chapter, the authors will describe tissue expander–based delayed breast reconstruction with total muscular coverage during the first-stage procedure. Emphasis will be placed on surgical technique, as well as highlighting key concepts in delayed implant-based breast reconstruction.
Indications and Contraindications
The delayed approach to two-stage implant-based breast reconstruction is indicated for patients who are, in general, good candidates for implant-based procedures. These include relatively thin patients and patients requiring bilateral reconstruction ( Fig. 13.1 ). The success and outcome of delayed implant-based reconstruction depends less on a reliable native soft tissue envelope since, due to the delayed nature of the reconstruction, the remaining mastectomy skin flaps have benefited from a delay phenomenon, making them more robust and reliable. Importantly, total muscular coverage relies on intact pectoralis major and serratus muscles as part of the reconstruction.

Furthermore, delayed reconstruction can serve a valuable role if immediate reconstruction is threatened by compromised mastectomy flaps, which risk prosthesis exposure or extrusion. If an autologous option is not possible, then a delayed two-stage implant-based reconstruction can be performed if the patient desires implant-based reconstruction.
On the contrary, relative contraindications to implant-based reconstruction include severe radiation changes or poor native skin for coverage of the implant. Other relative contraindications include obesity, smoking, and poorly controlled medical co-morbidities such as diabetes. Additionally, the senior author does not proceed with delayed implant-based reconstruction if the pectoralis major muscle has been resected or significantly traumatized. In cases of radiation or damaged pectoralis muscle, the senior author prefers a pedicled latissimus dorsi myocutaneous flap with a tissue expander for the two-stage delayed breast reconstruction.
Preoperative Evaluation and Special Considerations
A thorough discussion should be had with the patient prior to undergoing delayed implant-based breast reconstruction. A careful physical exam must also be performed, and key factors highlighted, such as missing pectoralis major muscle or serratus anterior muscle, quality of overlying skin, and potential regional coverage options such as the latissimus dorsi muscle ( Fig. 13.2 ). Expectations must also be addressed, including initial or final breast shape and size. Patients should be counseled that delayed reconstruction in the setting of limited skin pliability can lead to a slower or difficult expansion process as well as result in a less natural shape of reconstructed breast, especially lack of a well-defined inframammary fold.

Regarding the expansion process, attention is paid to the lower pole. Specifically, it will be important to choose a tissue expander that can preferentially expand the lower pole more. Surgical planning will also assist in redefining a new inframammary fold that is at the appropriate location. When using traditional tissue expanders, the placement of the tissue expander must be lower than the actual level of the inframammary fold in reference to the contralateral side so that the expansion for the lower pole can be optimized.
It is also important to emphasize need for total muscular coverage of the implant. In this manner, the pectoralis major muscle, serratus anterior muscle, as well as fascia of the rectus abdominis should be present. This will ensure that in cases of skin breakdown no implant is directly exposed. However, this also poses a risk for high-riding implants from the forces exerted by the overlying muscles. Patients must be informed of these risks as well as the postoperative discomfort and soreness that will result from the above-noted dissection.
Surgical Techniques
Relevant Surgical Anatomy
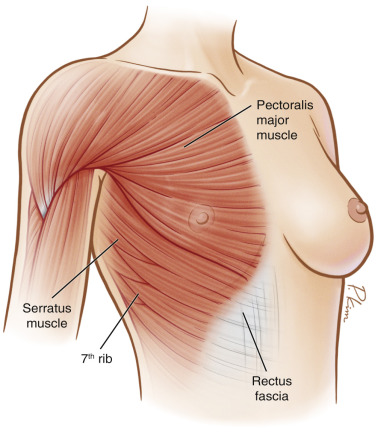
Total muscular coverage requires dissection to raise the pectoralis major muscle as well as the adjacent serratus anterior and the rectus abdominis fascia ( Fig. 13.3 ). The pectoralis major muscle has origins from the medial half of the clavicle, the sternum, the costal cartilage from the first to sixth ribs, and from the aponeurosis of the external oblique muscles. The fibers insert into the bicipital groove of the humerus. The blood supply is from the thoracoacromial artery which lies on the deep surface of the muscle. The serratus anterior muscle originates from the first through eighth ribs and has multiple slips that insert into the medial edge of the scapula. The rectus abdominis fascia lays inferior to the pectoralis muscle. The fascia can be dissected off the muscle belly in order to provide inferior implant coverage.
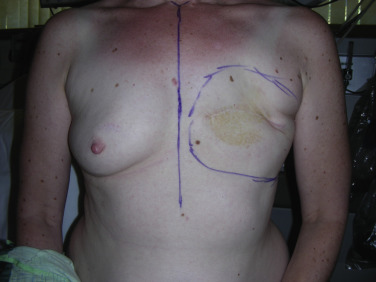
Preoperative Markings
On the morning of surgery, the patient is seen and marked in the standing position. The anatomic landmarks include the sternal notch, midline, and proposed new inframammary fold and lateral border of the breast as well as the breast “footprint” ( Fig. 13.4 ). Specific attention must be paid to the placement of the new inframammary fold as intraoperative dissection and subsequent expansion relies on the proper recreation of the fold. Several options of expanders are available, but the final decision is made by the plastic surgeon intraoperatively after the new breast total muscle pocket is created. This ensures that each patient receives a reconstruction tailored to her individual needs.
Intraoperative Markings
The borders of the breast as well as its “footprint” will be transposed inside on top of the chest wall and muscles to help recreate the implant pocket. The two key areas are the inframammary fold and anterior axillary line, as this will require dissection of the serratus anterior muscle and rectus fascia in order to define the fold and lateral extent of the new breast. The transposed markings will also serve to guide muscle elevation and submuscular pocket dissection.
Details of the Procedure
The surgical exposure for delayed implant-based reconstruction is created through the prior well-healed mastectomy scar. However, only a portion of the original incision may be used during the reconstruction ( Fig. 13.5 ). Prior to incision, the incision is infiltrated with 1% lidocaine with epinephrine. The procedure begins by making the incision through the skin and subcutaneous tissue down to the prepectoral fascia. Using sharp dissection and lighted retractor, the skin flaps are elevated to the borders of the pre-marked breast border to create the soft tissue envelope ( Fig. 13.6 ). Next, the lateral border of the pectoralis major muscle is identified and from here, the muscle is raised. Again, be sure to achieve adequate hemostasis from any perforating vessels during this dissection. Care must be taken with dissection underneath the pectoralis major muscle to avoid injury to the thoracoacromial artery. It is also wise to avoid cautery dissection directly on top of the ribs, as this will lead to increased postoperative pain.


Attention is then turned to the anterior rectus abdominis fascial sheath, which is elevated from the muscle belly. Take this dissection inferiorly and as low as possible using the proposed pre-marked inframammary fold as guide. Remember, the expander is ideally placed 1–2 cm below the inframammary fold to allow for maximal expansion in the lower pole of the breast. Next, the serratus anterior muscle is identified and dissected from the chest wall from anterior to posterior along the chest wall. This dissection defines the lateral extent of the submuscular pocket.
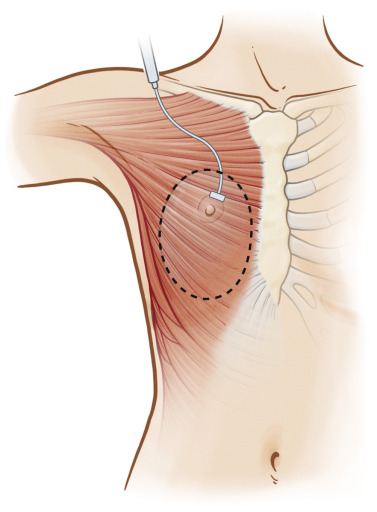
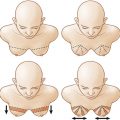
The pocket is then irrigated thoroughly with triple antibiotic solution in the standard fashion. The appropriate size of a medial high tissue expander is selected and placed within the submuscular pocket with a no-touch technique. The expander should be placed as low and medial as possible ( Fig. 13.7 ). Closure of the muscular pocket is taken by suturing the anterior border of the serratus anterior to the lateral border of the pectoralis muscle with 3-0 Vicryl sutures in an interrupted figure-of-eight fashion ( Fig. 13.8 ). Intraoperative fill volume of methylene blue injectable saline depends on clinical assessment of the skin envelope and muscle pocket. The initial volume can be between 60 and 180 cc. Of note, this is less than in the case of immediate reconstruction due to constraints from the tighter soft tissue envelope. The goal is to decrease dead space while maintaining healthy skin flap perfusion to avoid skin flap necrosis.
Related posts:
 Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Fat Grafting as an Adjunct Procedure in Breast Reconstruction
Fat Grafting as an Adjunct Procedure in Breast Reconstruction
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


