Fig. 10.1
The nose can be divided into three parts according to its deep bone supports
One aim of the nasal repair and reconstruction is to provide a functional, open, and moist airway, which means that not only the external airway but also internal nasal valve must remain open. The nasal limen within the nasal cavity is an integral part of the airway in the middle dome, and in here, the lateral nasal cartilage and the septal cartilage join together at a 10–15° angle. When reconstructing this area, providing a sufficiently thin lining structure is very important, because it can not only keep the airway open but also provide appropriate vascular beds for any cartilage grafts to reconstruct the bony framework of the nose. The scars in the nasal limen or nostril area within the nasal cavity affect the nasal ventilation. In general, the difficulty level of nasal reconstruction increases with the structural complexity of the nasal lining. If there is no enough nasal lining, the reconstructed nose will inevitably shrink.
Another factor in the analysis of nasal defect structure that needs to be considered is different skin thicknesses in the upper and lower part of the nose. The skin in the upper two thirds of the nose is thin, with a thickness of about 1300 μm, and it is smooth and has movability; the lower one third of the nose is thick, with an average thickness of about 2400 μm, and it is rich in sebaceous glands and is adhered with the deep structures (Table 10.1).
Table 10.1
The thicknesses of the skins in the upper and lower part of the nose and the different parts of the body
Location | Skin thickness | Location | Skin thickness |
|---|---|---|---|
Nasal dorsum | 1300 μm | Supraclavicular area | 1800 μm |
Nasal lobule | 2400 μm | Submental area | 2500 μm |
Retroauricular area | 800 μm | Nasolabial groove | 2900 μm |
1.3 Subunit Principles
The concept of facial aesthetic unit was firstly proposed by Gonzalez-Ulloa in 1956. He stressed that when the facial wounds are repaired, the repair should be performed according to the aesthetic unit, and the aesthetic unit is determined based on the skin thickness, histological features, and characteristics of the hidden scar in the border area [1].
In order to better, more accurately repair this unique tissue, proposed the subunit principle for nasal repair and reconstruction, which was a new and improved specification [2]. They expanded the principles of Gonzalez-Ulloa on the facial aesthetic unit in facial repair, and the nose is divided into six subunits: nasal dorsum, nasal tip, nasal columella, nasal sidewall, soft triangle, and nosewing (Fig. 10.2). They further put forward that if the defect area in the nasal tip or nosewing is more than 50%, the entire subunit should be removed, and the final scars will be hidden in the shade or at the junction of neighboring subunits. At present, the clinical assessment of the nasal defect and the surgical repair also take this as the basis of theoretical guidance. Therefore, understanding the anatomic and histologic characteristics of the nasal substructure is the key to accurately repair the tissue of the nasal substructure and restore the morphology of the specific facial organ.
Fig. 10.2
Subunit principles for nasal repair
Recently, Singh, Bartlett, and Rohrich et al. reported that they proposed further improvements on the subunit principles; in addition that the defect area is assessed in both aspects of subunits and different layers (skin, supporting structure, and lining), it should also take into account other factors, such as skin color, texture, thickness, and extent of photochemical damage. They suggested that nasal repair and reconstruction should be performed based on the individual patients and the different local soft tissues, the location and range of the defect, and the patient’s past medical history should be taken into account. All these can affect the complexity of the repair surgery. Of which, the selection of repair method by the patient is one of the main influencing factors, and especially the people in the eastern population are often reluctant to have additional scars left on their faces. Therefore, the application of forehead flap is often limited.
1.4 The Principles for Nasal Repair
- 1.
- 2.
The nasal subunit principles proposed by Burget and Menick should be taken as the guiding principles for nasal repair and reconstruction, but under the premise of reserving the skin color, texture, and nasal contour, it is not usually necessary to strictly adhere to the nasal subunit principles.
- 3.
In the selection of methods for repair and reconstruction, the specific conditions of individual patients should be considered, not only their disease, skin color, and texture but also the defect range. It is not necessary to strictly comply with the subunit principles.
- 4.
The similar tissue principle of tissue repair in plastic surgery should be followed during surgery, and the similar tissues are used as substitutes. In the selection of local skin flap, forehead flap, and free skin flap, the approximation of skin thickness and texture and the similarity of morphology are important factors to take into consideration.
- 5.
In nasal repair and reconstruction, the precise planning and meticulous surgical operation can achieve both functional and aesthetic effects of the defect repair.
2 Reconstruction of the Nasal Covering Tissues
2.1 Repair of Small-Area Defect
Small nasal defects can be repaired with many methods, including skin transplantation, local skin flap, and composite transplantation. The local skin flaps in nasal, buccal, or forehead area are usually the best matches in the skin color and texture.
2.1.1 Skin Graft Transplantation
For the small and superficial nasal defects, the skin graft transplantation is a simple method with few complications. The skin in the lower one third of the nose is thick and contains more fat. In comparison, the skin in the upper two thirds of the nose is thinner and movable and contains less fat. These basic reference markers are very important.
For the defects in the thinner and flatter upper two thirds of the nose, the repair with full-thickness skin graft is a better method. The most commonly used donor sites of the skin flaps include preauricular and retroauricular skins, supraclavicular area, and the forehead area. However, the pigmentation of skin graft and the possible occurrence of a bright and smooth appearance and the secondary contracture in the process of healing often limit its clinical application.
2.1.2 Local Skin Flap
- 1.
Banner flap. The banner flap was proposed by Elliot (1969). The method is suitably used in the upper part of the nose, where the skin tissue is relatively loose.
The method is to design the single triangular flap or banner flap along the cutting line of the defect; the skin flap is designed horizontally, which will be conducive to the closure of the donor site. The scars can be hidden within the stripe lines, and both sides of the nose are kept relatively symmetrical. This skin flap can be used for repair of the defects with a diameter of less than 1.2 cm in any part of the nose (Fig. 10.3).
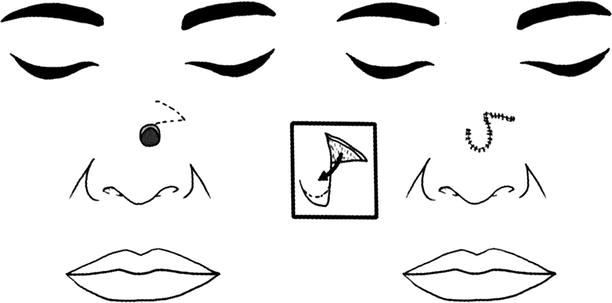
Fig. 10.3
Banner flap
When the skin flap is harvested, its pedicle is equivalent to the diameter of the defect, and its length should exceed one third of the diameter of the defect. The adequate dissociation is performed on the layers such as under the muscle and perichondrium and above the periosteum, in order to facilitate rotation of the skin flap, and then the skin flap is inserted into the defect area; at the moment, the small triangle at the distal end is usually removed.
- 2.
Bilobed skin flap. The bilobed skin flap is commonly used in the repair of the defects in the lower one third of the nose and is also used for repair of the defects in nasal dorsum or nasal side. This skin flap is only used to repair the defects with a diameter less than 1.5 cm, and it is needed to use the tissues in the two thirds of the nose.
Firstly proposed by Esser and Zimary, the method is to design a bilobed skin flap with a total rotation angle of 180°. But this design is flawed, and it will lead to a significant projection of “orecchiette” or appearance of a protuberance in the position of the pivot point; after its removal, the base and pedicle of the skin flap will be narrowed, and thus the blood supply of the skin flap will be affected.
In 1989, Zitelli proposed the optimal design method of the bilobed skin flap: the maximum rotation angle of each flap of the bilobed skin flap is 45–50°, and the total rotation angle is 90–100°. Along the margin of the defect, the Burow triangle included in the design is resected, then the first lobe of the skin flap is advanced downward, and the top point of the Burow triangle is taken as the pivot point of rotation of the bilobed skin flaps. The first lobe and the nearest defect have the same diameter; the second lobe is slightly narrower (it is generally 80% of the first lobe), but it must be ensured that the defect left after rotation can be closed directly, while the final incision should be made in the site with a minimum of tension to facilitate reducing the scar, generally in the lateral nasal wall. The skin flap is fully dissociated at the layers such as under the muscle, perichondrium, and periosteal surface, so as to ensure the blood supply of the skin flap. After the complete hemostasis of the wound is performed, the first lobe is rotated by 45–50° to cover the original wound, and then the second lobe is rotated by 45–50° to fill the defect left after rotation of the first lobe. The second donor site can be closed directly with absorbable suture lines (Fig. 10.4). Usually the rotating shaft should not be close to the margin of the nosewing and the lower eyelid to avoid distortions.
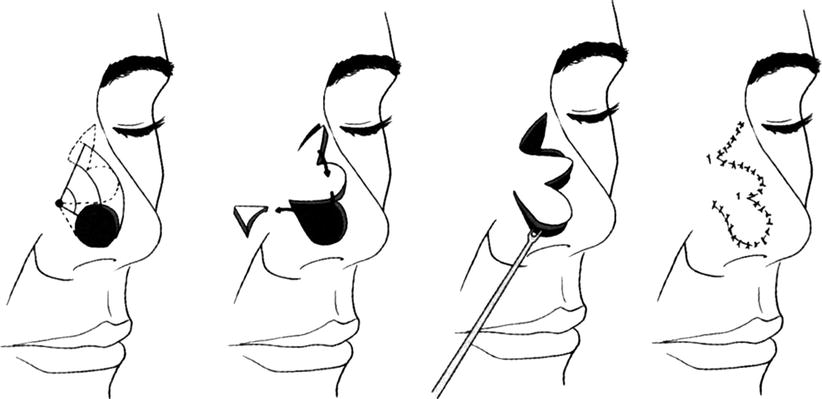
Fig. 10.4
Bilobed skin flap
Case I
The patient, female, 21 years old, had had a mass in the nosewing for 21 years, whose growth was accelerated for 1 year. The extensive resection of the mass was performed, and the adjacent bilobed skin flap was used for repair (Fig. 10.5). Postoperative pathology: intradermal nevus.

Fig. 10.5
Case I. (a) The intradermal nevus at the junction of the nasal tip and nosewing; the size was about 1.5 cm × 1.5 cm. (b) Design of bilobed skin flap, the inclined angle was 90–100°, and the second lobe skin flap was designed in the lateral nasal wall with relatively loose tissues, so as to facilitate the direct closure of the wound. (c) The bilobed skin flap was prepared after mole removal. (d) The bilobed skin flap was separated under the nasal muscles. (e) The bilobed skin flap was used to repair the wound in the nosewing
- 3.
Rhomboid skin flap. The rhomboid skin flap comes from the neighboring buccal area, and it was originally used for repair of defects in nasal sides. The first side of the skin flap is designed along the nasolabial groove, the other side is located at the margin of the defect, and the last side crosses the cheek. The skin flap is lifted up, and the extensive dissociation is performed in the subcutaneous layer. It is easy to advance the skin flap to cover the defect through adequate dissociation, and it is not necessary to perform the “orecchiette” resection (Fig. 10.6). The postoperative scar is located in the nasolabial groove, or in the folds of the nosewing, or at the junction of the nasal side and the buccal area. Because the tension line is not in the vertical direction, therefore, the possibilities of occurrences of the lower eyelid eversion and the elevation of the lip or nosewing margin are minimal.
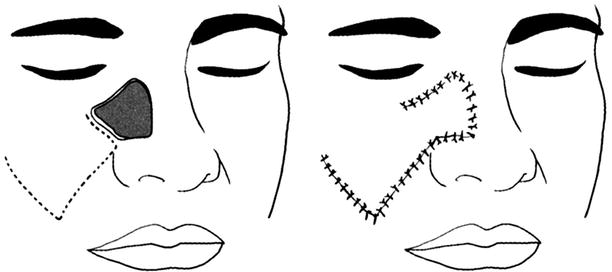
Fig. 10.6
Rhomboid skin flap
The buccal tissue can also be used as a simple advancement flap for nasal defect repair. Incise the skin to the subcutaneous layers at the nasolabial groove, the adequate dissociation is performed at 2.5 cm above the buccal area adjacent to the defect and the skin flap is advanced to cover the defect in the nasal side, and the donor site is closed directly. The buccal advancement flap can also be used in combination with other flaps for total nasal reconstruction, such as the median forehead flap.
Case II
The patient, female, 70 years old, had had a mass in the right face beside the nose for 2 years. The extensive resection of the mass in the right face beside the nose was performed, and the adjacent facio-buccal skin flap was advanced for repair (Fig. 10.7). Postoperative pathology: highly differentiated squamous cell carcinoma.

Fig. 10.7
Case II. (a) Paranasal squamous cell carcinoma in the right face. (b) Intraoperative extensive resection, the pathological examination showed that the periphery and base were negative; the wound was about 2.5 cm × 2 cm. (c) Design of the incision of the advancement flap in buccal area. (d) The range for subcutaneous dissociation of the skin flap. (e, f) The lateral and positive profiles at 1 year after surgery
- 4.
The advancement flap of the nasal dorsum. The advancement flap of the nasal dorsum (Rieger method) is suitably used for repair of the defects in the nasal tip and the distal nasal dorsum with a diameter of less than 2 cm. Typically, the skin flap is used to repair the defect with a distance of at least 1 cm from the nosewing margin which can’t be lower than the nasal tip point. If the repair site is too distal, it will lead to postoperative nasal tip rotation or nosewing traction.
Rieger method: The incision line travels from the outside of the defect, extends along the junction of nasal side and buccal area upward to the area between the eyebrows, and stops near the contralateral inner canthus (downward to the inner canthal ligament); after skin flap harvesting, a random rotation skin flap with a long lateral pedicle is formed. The proximal end of the skin flap is lifted up at the subcutaneous level in the areas above bilateral internal canthi, then the separation is performed forward under the muscular layer to the distal end of the skin flap, and then the skin flap is advanced to the appropriate position and is sutured. The defect between the eyebrows after skin flap advancement is closed directly, and the complete dorsum nasal flap is formed into a V-Y advancement flap (Fig. 10.8).
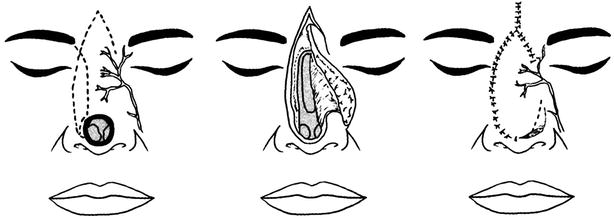
Fig. 10.8
The advancement flap of the nasal dorsum (V-Y advancement flap)
Marchac and Toth improved the random advancement flap of Rieger into an axial pattern skin flap based on the angular artery branch issued near the inner canthus. Such design makes the pedicle become narrow, so that the mobility of the skin flap is greater.
After that, Ercocen designed the complete dorsum nasal island flap based on bilateral angular arteries, and the donor site between the eyebrows is closed with the V-Y method. Such skin flap is easy to be advanced to cover the defects in the nosewing margin, the distal nasal dorsum, nasal tip, and soft triangle and the range of 2–3 cm above the nasal columella.
- 5.
Nasolabial flap. The nasolabial flap is the primary technology used in repair of the nosewing defects with a diameter of less than 2 cm. It can also be used to reconstruct the nasal columella and can be used as the donor site of the nasal lining tissues [4].
- (1)
Design methods and transfer modes of the nasolabial flap: There are two design methods for the nasolabial flap: (1) as random flap, its blood supply comes from the subdermal vascular network; and (2) as axial flap, its blood supply comes from the angular artery and the branch of the facial artery. Its transfer mode also includes two types:
- 1)
Transfer of pedicled island flap: Design the nasolabial island flap or perforator skin flap; design an ellipse which is two times longer than the defect along the nasolabial groove. Taking into account the postoperative scarring and contracture, the size of the skin flap should exceed 1 mm compared with the defect in any direction. The skin flap is harvested from the distal to the proximal end; attentions are paid to avoid damage to the levator labii superioris and the intramuscular perforators. The proximal pedicle skin can be completely retained as a narrow bridge or be completely cut open, and only the subcutaneous pedicle is retained to maintain the blood supply of the skin flap. The skin flap has enough mobility to be able to rotate about 150° to repair the nosewing defect, and the donor site is closed through separation and advancement of adjacent buccal tissues. The pedicle is cut off 3 weeks later; the skin flap after being lifted up is trimmed thin and shaped and is inserted to form the base of the nosewing. If it is a full-thickness defect, it is necessary to harvest cartilage from the nasal septum or auricle for transplantation, and the reconstruction of nosewing support must be included. If the natural junction of the base of the nosewing and the face is not destroyed, it should be protected during surgery, because it is difficult to reconstruct the groove. For the full-thickness defect of the nosewing, the distal end of the skin flap can be folded as the lining and is sewn onto adjacent nasal mucosa.
- 2)
Reversed nasolabial flap: It is used most suitably to repair the full-thickness defect in the lateral nosewing; the defect with a size of three fourths of nosewing can be repaired by this method. The blood supply of the skin flap comes from the facial artery, the infraorbital artery, and the perforating branches of the ophthalmic artery, which converge together near the base of the nosewing. Based on such rich blood supply, when the skin flap is harvested, its base width is 10–15 mm, and its length can reach four times the width. The skin flap is marked at the lateral side of the defect, crossing the nasolabial groove; the position of the base of the skin flap is made as close as possible to the nosewing defect. The skin flap is incised from the distal end and is lifted up toward the proximal end, and the subcutaneous fat layer (2 ~ 3 mm) is retained. It is noted to protect the medial subcutaneous pedicle. After being lifted up, the skin flap is transferred and overturned into the defect area, the inner surface of the skin flap is sutured close to form the lining, and then the distal end of the skin flap is folded on its own surface to form the nosewing margin, which is trimmed and then inserted (Fig. 10.9). The transplanted nasal alar cartilage is inserted between the reverse folded layers. When the second-stage surgery is performed, the base of the nosewing is moved to the medial side with V-Y advancement to create a better contour of the junction of the nose and face. The nasolabial flap has a natural tendency to shrink in the long term, which is useful in the reconstruction of the nosewing, so that the reconstructed nosewing is more natural and realistic.
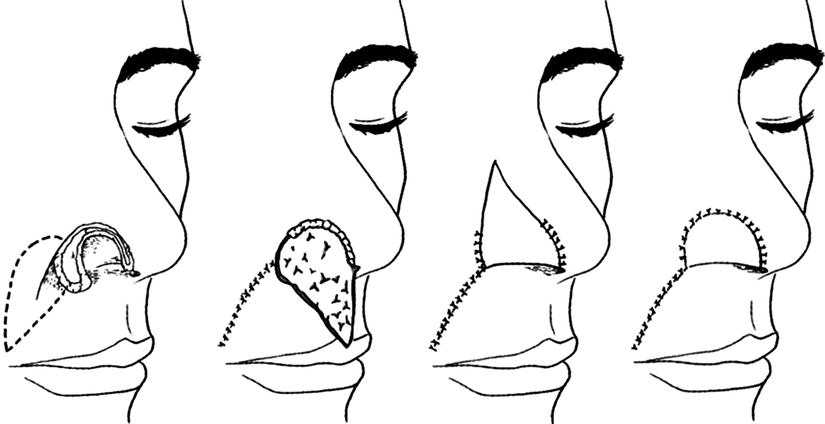
Fig. 10.9
Reversed nasolabial flap
- 1)
- (2)
A typical case:
- 1)
Case III: The patient, male, 45 years old, had had a mass in the left nosewing for 5 years. The patient underwent the extensive resection of the mass and the repair with nasolabial flap (Fig. 10.10).

Fig. 10.10
Case III. (a) The benign tumor in the lateral nosewing, with a size of about 1 cm × 0.8 cm. (b) After tumor resection, the nasolabial flap with a pedicle in the upper part was adopted for repair. (c) After harvesting of the nasolabial flap, the donor site after slight dissociation was sutured directly and the scars were located within the nasolabial groove. (d) The nasolabial flap was transferred to repair the nosewing defect
- 2)
Case IV: The patient, male, 68 years old, had right paranasal basal cell carcinoma. The patient underwent the extensive resection and the repair with nasolabial facial artery perforator flap (Fig. 10.11).

Fig. 10.11
Case IV. (a) Right paranasal basal cell carcinoma. (b) After tumor extensive resection, the peripheral margins and the base were negative, and the remaining wound was about 2.5 cm × 1.5 cm. (c) The defect was repaired with the nasolabial facial artery perforator flap, the perforator vessel issued from the angular artery was observed during surgery, and the perforator vessel was dissociated. (d) V-Y advancement of nasolabial perforator flap was performed to repair the wound. (e) At 7 days after surgery
- 1)
- (1)
- 6.
Get Clinical Tree app for offline access
Auricular composite tissue flap. The non-pedicled auricular composite tissue flap transplantation is only suitable for repair of the nasal defects less than 1 cm2. Due to blood supply limitation, with the increase in volume of composite tissue, the transplantation survival rate gradually decreases. The auricular composite tissues can be obtained from the crus of helix, auricular margin, cavum conchae, or earlobe. The crus of helix is the commonly used donor site, because it can provide three-tier structure of the skin, skeleton support, and lining, and remaining scars are not obvious. The transplantation of the auricular composite tissue with a diameter less than or equal to 1 cm is often used for repairs of the nosewing full-thickness defect and the nasal columella defect; the composite tissue including crus of helix and retroauricular skin can be jointly harvested for one-stage repair of the nosewing full-thickness defect and the lateral nasal wall defect involving only soft tissue. Due to lack of blood supply, the area of the transplanted tissue cannot exceed 1.0 cm × 1.5 cm, limiting the further application of donor site of the tissue. In 1993, Julian J. Pribaz firstly reported that the vascularized auricular composite tissue was used to repair the nosewing defect [12]; in the same year, Tanaka Y. reported that the auricular composite tissue flap pedicled with the retrograde superficial temporal blood vessel pedicle was used to repair the nasal full-thickness defect [13]. In 1999, Bakhach Joseph used the communication network between the frontal branches of the superficial temporal blood vessel and the supraorbital vessels as well as the supratrochlear vessels to design the pedicled transfer of retrograde auricular composite tissue flap to repair the nosewing defect [14]. In 2008, Qian Yunliang and Zhang Yixin from Shanghai Ninth People’s Hospital reported that the auricular composite tissue flap including auricular and preauricular tissues which was pedicled with the superficial temporal vessel was used to repair the full-thickness defect in tissues of multiple nasal subunits in 63 patients, expanded the clinical application of surgical techniques, and got a very good therapeutic effect [15]. These research and clinical application break through the limitation on the transplantation area of the traditional nonvascularized auricular tissue, so that it becomes a reality that the auricular composite tissue is taken as the best donor site [16–21].
- (1)
The anatomical study of the auricular composite tissue flap: Houseman ND and Taylor GI carried out a study on blood vessel perfusion in head and neck area and found that the external ear has two sets of blood supply, the superficial temporal artery and the retroauricular blood vessel system which feed the anterior and dorsal part of the external ear. The superficial temporal artery penetrates out of the deep surface of the superficial lobe of the parotid gland in preauricular area, runs under the facial subcutaneous superficial fascia downward to the temporal region, and gives off several vascular branches at the upper crus of helix to feed the auricle; their blood supply range accounts for about the upper two thirds of the auricle.Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
 Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



- (1)