Fig. 18.1
After burn trauma in the upper segment of the left calf, the patient had recurrent ulcers for more than 10 years; the pathological examination showed skin squamous cell carcinoma
2.1.2 Surgical Treatment and Wound Repair
Currently the surgery is the preferred method for treatment of malignant skin tumor [1–4]. For the prevention of postoperative recurrence, the range of the surgical resection should be large enough, which is directly related to the prognosis of the patient and the recovery of the local appearance and function. It is generally required that when skin squamous cell carcinoma is resected, the distance between the incision and the lesion margin should be greater than 1.0–2.0 cm. At the same time, the depth of resection of skin squamous cell carcinoma should be determined according to the depth of tumor invasion.
The repair of wound after tumor resection should follow the sequence for repair of soft tissue defects, the direct suture is considered firstly, and the second consideration involves skin transplantation, local flap, muscle flap, or fascial flap combined with skin grafting, distal flap, and free flap. The distal flap should be carefully selected, which has the possibility to metastasize the tumor to the donor site. The flap is preferably selected in the pretibial area or plantar weight-bearing area, the tissue flaps available to be selected by the former for repair include the retrograde fasciocutaneous flap with sural nerve, posterior tibial artery perforator flap, gastroecnemius myocutaneous flap, gastrocnemius muscle flap, or soleus muscle flap combined with skin grafting, and the medial plantar skin flap is preferably selected by the latter [5].
It is recommended that the prophylactic or selective lymph node dissection is not performed in high-risk patients. For the palpable lymph nodes, if the biopsy confirms the presence of lymph node metastasis, the lymph nodes should be removed. There is still no conclusion on whether the guided sentinel lymph node biopsy is implemented in those patients with high risk of lymph node metastasis.
In short, the early and accurate diagnosis of skin squamous cell carcinoma requires the rich experiences of the clinicians and the support of the pathological diagnosis, thereby reducing the cases of misdiagnosis and missed diagnosis. The timely treatment is very important for the prognosis of the patient.
2.1.3 The Fasciocutaneous Flap with Nutrient Vessels of Sural Nerve and Small Saphenous Vein
The fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein is widely used due to the fact that it doesn’t damage the main blood vessels, the survival rate of the skin flap is high, and most donor sites can be directly sutured. In 1992, Masquelet et al. carried out anatomical studies on the calves in perfused fresh corpses and found that the nutrient arteries of the saphenous nerve, superficial peroneal nerve, and sural nerve not only feed their accompanying nerves but also gives off a number of cutaneous branches into the superficial fascia on the superficial surface of the nerve. These nutrient arteries may be an artery and may also be an arterial network woven by small arteries. Moreover, these arteries are also anastomosed with the perforators of the well-known deep arteries. Based on this discovery, they put forward the concept of neurocutaneous island flap and use it in repair of soft tissue defects of the calf, of which the retrograde fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein has attracted more widespread interest.
- 1.
Surgical design: The retrograde fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein is the neurocutaneous flap taking the sural nerve nutrition blood vessels as the supply vessels; the axis line of the skin flap is the connecting line between the Achilles tendon and the midpoint of the lower boundary of the popliteal fossa; the axis point can be set on the axis line at 5–10 cm above the lateral malleolus. The upper boundary of the skin flap does not exceed the junction of the upper and middle third of the posterior calf. To ensure the blood supply of the skin flap, most physicians will make the pedicle of the skin flap into the nerve and fascia pedicle with deep and superficial fascias, and the pedicle width is not less than 3 cm; therefore, this skin flap is also called as retrograde sural nerve fasciocutaneous flap. Since the nutrient vessels of the sural nerve are anastomosed with perforating branches of the peroneal artery at the ankle level, Doppler detector is used to detect around the designed axis point before surgery; sometimes the echo of blood flow can be heard; at the moment, the axis point should be changed to the site with the echo of blood flow as far as possible, in order to ensure the blood supply of the skin flap (Fig. 18.2).
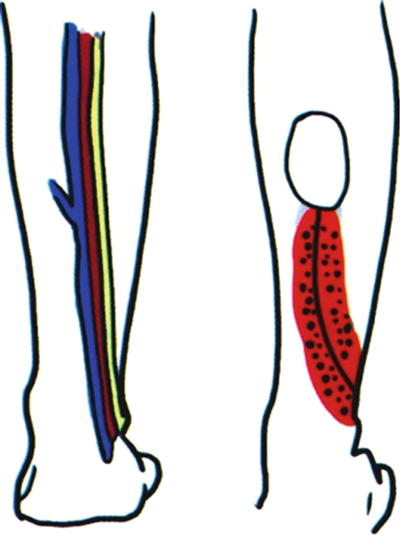
Fig. 18.2
Design of sural nerve and its nutrient vessels and skin flap
- 2.
Surgical methods: The tourniquet is used to stop bleeding in the lower limbs. The skin, subcutaneous tissue, and deep fascia are incised according to the design. Between the deep fascia and the muscle membrane, the separation is performed from both sides of the skin flap to the central axis. In the proximal skin flap, the small saphenous vein and sural nerve are explored and ligated. The skin flap is lifted up from the near to the distant; the skin flap is formed into neural and fascial pedicled island flap; the skin flap is transferred to the receptor site through the tunnel between the skin flap and the receptor site (or the skin is incised). The donor site is directly sutured or is implanted with the intermediate-thickness skin graft.
- 3.
Typical cases
- (1)
Case I: The patient, male, 72 years old, had a chronic ulcer complicated with squamous cell carcinomas on the posterior side of the ankle of the left calf; the wound after skin flap resection was covered with the fasciocutaneous island flap with nutrient vessels of sural nerve and small saphenous vein (Fig. 18.3).
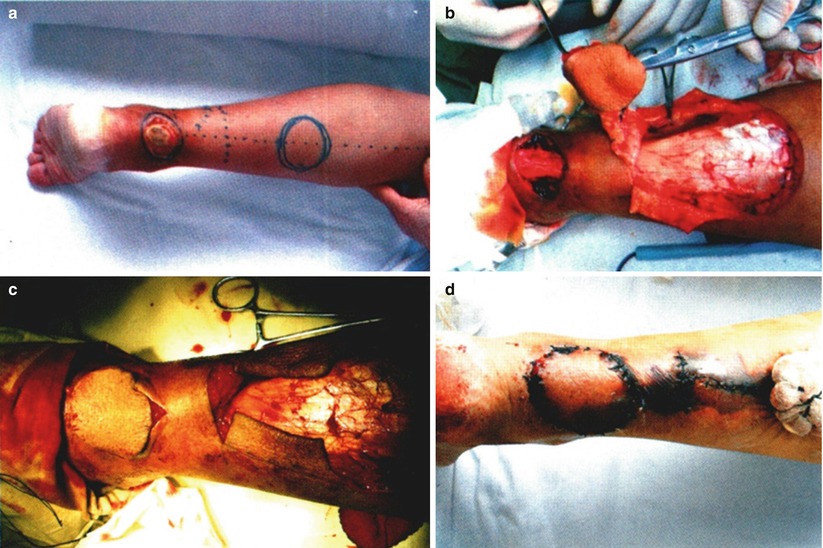
Fig. 18.3
Case I. (a) Skin flap design. (b) Lifted up the skin. (c) The skin flap was transferred into the receptor site. (d) At 1 week after surgery
- (2)
Case II: The patient, male, 54 years old, had squamous cell carcinoma above the medial malleolus of the left calf; the wound after tumor resection was covered with the fasciocutaneous island flap with nutrient vessels of sural nerve and small saphenous vein (Fig. 18.4).
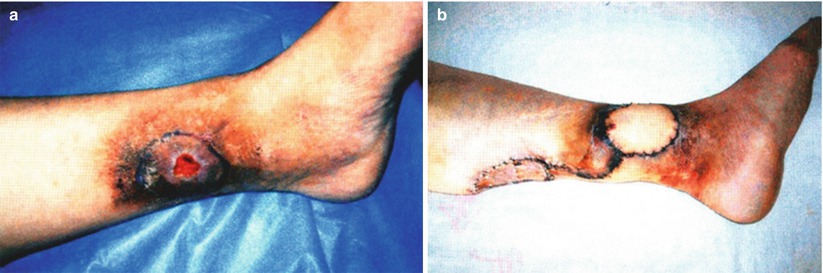
Fig. 18.4
Case II. (a) The lesion site of squamous cell carcinoma in the upper part of the left calf before surgery. (b) The wound was covered with the fasciocutaneous island flap with sural nerve
- (3)
Case III: Skin squamous cell carcinoma in the left popliteal fossa was treated with the extensive resection of the left popliteal fossa lesion plus the repair with free latissimus dorsi skin flap (Fig. 18.5).
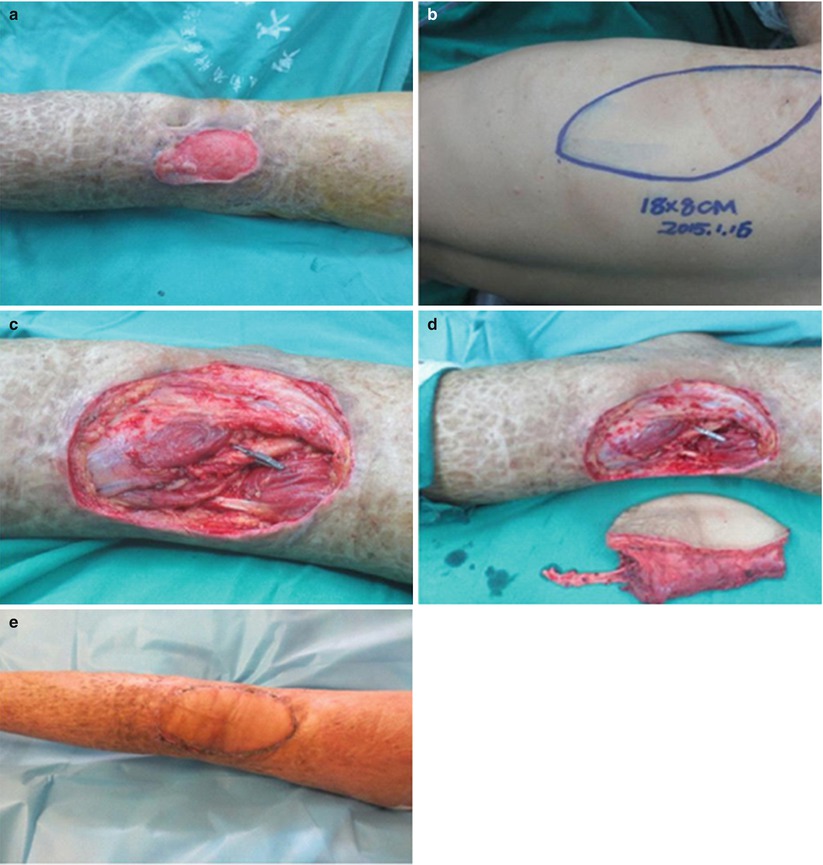
Fig. 18.5
The patient with skin squamous cell carcinoma in the left popliteal fossa. (a) Before surgery. (b) Design of latissimus dorsi myocutaneous flap. (c) The tissue defect after extensive resection of the left popliteal fossa lesion. (d) The extensive resection of the left popliteal fossa lesion plus the repair with free latissimus dorsi skin flap was carried out. (e) The patient was reexamined at a month after surgery
- (1)
- 4.
The advantages and disadvantages of the skin flap: The main advantages of the retrograde fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein are that the blood supply is reliable, the rotating radian of the skin flap is large, the surgical operation is simple, and there is no damage to the well-known vessels.
The main disadvantage of this skin flap is the discomfort caused by the lateral foot numbness after surgery. But the follow-up carried out by Costa-Ferreira et al. showed that both the lateral foot numbness and the nerve edema have been improved at 12 months after surgery. Another disadvantage is that it does not apply to the wound with a larger area. Ayyappan et al. extended the upper boundary of the skin flap to the upper one third of the posterior calf and designed the oversized fasciocutaneous flap with sural nerve with the maximum area of 17 × 16 cm. We also carried out a trial on this, but an oversized fasciocutaneous flap with sural nerve with an area of 18 × 6 cm was mostly necrotized due to venous congestion with infection, and therefore, we believe that before there is enough evidence suggesting that the sural nerve artery can provide nutrition for the skin flap with super large area, one should be careful to use the oversized fasciocutaneous flap with sural nerve.
2.2 Malignant Melanoma
The malignant melanomas only account for 5% of the annually diagnosed skin cancers, but the mortality rate accounts for 75% of all skin cancers. Due to wide development of health education work, the level of awareness for the hazards of malignant melanoma in the masses is greatly improved; when the primary tumor is still confined to the skin, many patients have obtained the diagnosis and treatment. Malignant melanoma most commonly occurs in the skin of the lower limbs in women. In Asia, it often occurs in the plantar skin or the nail bed.
2.2.1 Clinical Manifestations
The early clinical symptoms of skin melanoma can be summarized as ABCDE rule; this rule helps to identify the lesions similar to malignant melanoma, namely, A. asymmetry, B. irregular margin, C. uneven color, D. the lesion with diameter and pigment spot diameter of more than 5–6 mm can be considered suspicious, and E. uplift. The only disadvantage of this rule is that the speed of melanoma development, namely, the trend of significant change occurring within weeks or months, is not taken into consideration. Therefore, attention should be paid to the growth and variation trend of pigment spots.
In addition, any pigmented lesions have satellite lesions; the color intensity is increased or decreased, there exists itching, bleeding, rapid tumor growth, hair loss or hair growth, all suggesting that the cell proliferation within the lesion is active; sharp vigilance should be maintained at this point.
Any suspected lesions require surgical resection and pathological examination, so as to definitely diagnose the suspected cases and accurately determine the thickness of the tumor, thus providing the basis for further treatment.
The advanced patients usually present with larger black tumor body in plantar skin surface. Part or all of the tumor body protrudes out of the skin, or the skin is ulcerated with a prolonged healing and has black exudates. The patients cannot walk and see the doctor mostly due to the influence of the tumor body. Most patients still have no enlarged lymph nodes in the groin.
2.2.2 Pathological Classification and Prognosis
The study found that the thickness of the skin invaded by the malignant melanoma is closely related to the prognosis. At present, there are mainly two methods of classification according to the melanoma thickness:
- 1.
Clark classification: Clark divided the malignant melanoma into five stages according to different depths of the skin invaded by the tumor: (1) Stage I: Intradermal melanoma – it will not be metastasized and is benign. (2) Stage II: The tumor body penetrates through the basilar membrane. (3) Stage III: The tumor body is full of dermal papilla and invades into the reticular dermis. (4) Stage IV: The tumor body infiltrates the reticular dermis. (5) Stage V: The tumor body invades into subcutaneous fat.
- 2.
Breslow classification: Breslow accurately measured the thickness of the tumor in the slice through the optical micro-measurement to classify the malignant melanomas: (1) Stage I: The thickness of the tumor body is less than 0.75 mm. (2) Stage II: The thickness of the tumor body is 0.76–1.50 mm. (3) Stage III: The thickness of the tumor body is 1.51–3.99 mm. (4) Stage IV: The thickness of the tumor body is greater than 4 mm.
The thicknesses of invaded skins are different; thus, the opportunities of lymph node metastasis and systemic metastasis as well as the prognoses are different.
In terms of the opportunity of lymph nodes and systemic metastasis, when the depth of skin invaded by the tumor is degree I, the incidence rate of regional lymph node metastasis is 2%–3%, and the distant metastasis rate is almost zero; when the depth of skin invaded by the tumor is degree II, the lymph node positive rate is 25%, and the distant metastasis rate is 8%; when the depth of skin invaded the tumor is degree III, the lymph node positive rate is 57%, and the distant metastasis rate is 15%; when the depth of skin invaded by the tumor is degree IV, the lymph node metastasis rate is 62%, and the distant metastasis rate is about 72%.
In terms of prognosis, when the lesion thickness is less than 1 mm, the resection and cure rate is over 99%, 5-year survival rate is 89%–95%; when the lesion thickness is between 1 and 4 mm, 5-year survival rate is 63%–89%; when the lesion thickness is greater than 4 mm, 5-year survival rate is 7%– 63%.
2.2.3 Surgical Treatment and Wound Repair
The surgical resection is still the preferred treatment; the surgical safety margin of the resection depends on the thickness of the tumor body (Table 18.1), but the current evidence-based medical evidence still supports that a safety margin of 2 cm is enough. Whether the wound margin after resection of the tumor body has residual tumor cells can be determined with the method of Mohs surgery.
Table 18.1
The reference range for resection of the tumor body of malignant melanoma tumor
The thickness of the tumor body (mm) | The resection range of the normal tissue outside the tumor body (cm) |
|---|---|
In situ | 0.5 |
≤1 | 1 |
1–2 | 1–2 |
2–4 | 2 |
≥4 | 2–3 |
The resected tissues include the tumor and its surrounding tissue; the depth reaches the deep fascia. Under the condition that the pathological examination confirms no tumor cells on the deep surface of the superficial fascia of the resected tissue block, the deep fascia should be retained; the retained deep fascia can be taken as the barrier for invasion of the tumor into the deep layer.
The repair of wound after tumor resection should also follow the sequence for repair of soft tissue defects. Since the malignant melanoma occurs mostly in plantar base and foot bottom, if the tumor body is located in a non-weight-bearing zone, the skin transplantation is firstly considered, and the split-thickness skin graft plus packing pressure is more commonly used; if the tumor body is located in a weight-bearing zone, the skin transplantation cannot be considered, and the pedicled skin flap and free skin flap should be used for wound repair. One should be careful to select the distal skin flap, which has the possibility to metastasize the tumor to the donor site. Because the medial plantar skin flap is located in the non-weight-bearing zone of the arch of the foot between the head of metatarsal bone and calcaneus, its anatomical structure is similar to the covering tissue in the weight-bearing zone, with good blood supply and sensation. It is an ideal donor site for repairing the wound in the weight-bearing zone (especially the heel); therefore, the medial plantar skin flap is preferred for repair of the wound in this zone. For the wounds in the bottom of the heel and the posterior heel, the anterograde medial plantar island flap can be selected for repair. For the wound in the anterior margin of the foot bottom, the retrograde medial plantar island flap can be selected for repair. If it is difficult to repair, other skin flaps can be selected, such as the fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein, the fasciocutaneous flap with nutrient vessels of saphenous nerve and great saphenous vein, and free skin flap.
- 1.
Medial plantar skin flap
- (1)
Related anatomy: The posterior tibial artery is divided into the lateral plantar artery and the medial plantar artery at the bifurcation of the starting point of abductor hallucis, and the medial plantar artery runs frontward between the abductor hallucis and flexor digitorum brevis, is parallel to the flexor hallucis longus tendon, and has 2–9 branches with varying diameters along the way. Of which, at the base of the first metatarsal bone, there is a larger branch running obliquely toward the second and third toes on the anterior outer side, this branch crosses the arch of the foot by about 2 cm, is anastomosed with the branch of the common plantar digital artery of the second and third toes, and is indirectly connected to the arch of the foot. The vascular thickness varies greatly. After giving off this branch, the trunk of the medial plantar artery continues to run forward and gives off inward the first medial plantar digital artery near the first metatarsal head, and then this trunk is anastomosed with the first plantar metatarsal artery; it continuously runs forward into the common plantar digital artery between the first and second toes and is connected with the deep plantar artery from the dorsal pedal artery through the first plantar metatarsal artery, thereby participating in formation of plantar arterial arch jointly by the deep plantar artery and lateral plantar artery; this structure is constant (Fig. 18.6). The medial plantar artery and its branches have their accompanying veins all the way.

Fig. 18.6
The distribution diagram of plantar blood vessels
- (2)
Skin flap design: The undersurface of the first metatarsal bone is taken as the base point, namely, the junction area of the weight-bearing zone in the anterior margin of plantar area and the non-weight-bearing zone; a straight line is drawn toward the point of intersection of the medial plantar margin and the continuation line of the anterior margin of the medial malleolus; this line is taken as the central axis to design the skin flap; the distal medial plantar artery or the diagonal branch is selectively used as the pedicle, or both are used jointly; the skin flap area in adults generally does not exceed 8 × 4 cm. The distance from the rotation point to the most distal end of the skin flap should be slightly greater than the distance from the wound to the most distal end. The size and shape of the skin flap are similar to those of the wound, so that the skin flap after transfer can be sutured without tension.
- (1)
- (3)
Surgical methods:
- 1)
Repair of heel with medial plantar island flap through antegrade approach: The distal incision of the skin flap is made on the proximal side of the first metatarsal head, the superficial branch of the medial plantar artery is found at first, and sometimes it needs to be ligated at the distal end of the skin flap. It is separated with the surface of the myolemma of the abductor hallucis under the metatarsal fascia from far and near to the binding area of the superficial blood vessels and deep blood vessels. After the deep blood vessels are ligated, the main trunks of medial plantar vessels and their accompanying plantar medial nerves are dissected in the abductor hallucis and flexor digitorum brevis, the main trunks of the nerves are retained in the original place, but attention is paid to preserving the nerve branches issued toward the skin flap. The blood vessels are separated toward the proximal posterior tibial artery and vein to a sufficient length, and the nerves are separated between beams to obtain a sufficient length, and the surgical dissection is completed (Fig. 18.7). The skin between the pedicle and the receptor site is incised and is transferred to the plantar wound through open approach; it should be avoided that the vascular pedicle is distorted and compressed (Fig. 18.8).
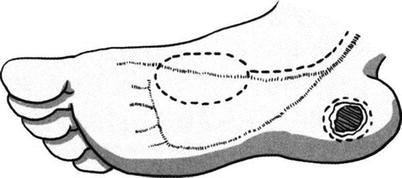
Fig. 18.7
Anterograde medial plantar island flap

Fig. 18.8
The medial plantar island flap was used to repair heel wound through antegrade approach. (a) The melanoma in the heel before surgery. (b) The incisal margin of the tumor and the medial plantar island flap was designed before surgery. (c) After resection of the lesion, the medial plantar island flap was transferred anterogradely to repair the wound. (d) At 2 weeks after surgery
- 2)
Repair of anterior plantar margin with medial plantar island flap through retrograde approach: The proximal lateral margin of the skin flap is incised at first; the dissection is carried out at the surface of the myolemma of the abductor hallucis from the near to the distant until the superficial branches of the medial plantar blood vessels enter into the skin flap. Then the bilateral margins of the skin flap are incised, as well the skin flap is dissected and dissociated at the surface of the myolemma of the abductor hallucis (Fig. 18.9). Then the skin at the distal side of the skin flap is incised; attention is paid to finding the superficial branch vessels and retaining their surrounding fascia and loose subcutaneous tissue; the pedicle is dissected without exceeding the proximal side of the first metatarsal head. The superficial branch of the artery is occluded at the proximal end with a vascular clamp for 5 min; when the blood supply of the skin flap is good, the proximal blood vessel is cut off; and the surgical dissection is completed. The skin between the pedicle and the receptor site is incised and is transferred to the plantar wound through open approach; it should be avoided that the vascular pedicle is distorted and compressed (Fig. 18.10).
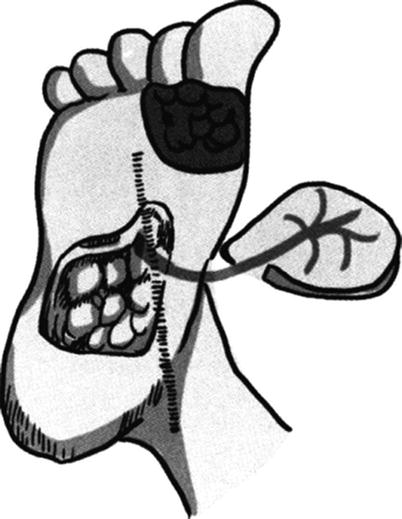
Fig. 18.9
Retrograde medial plantar island flap
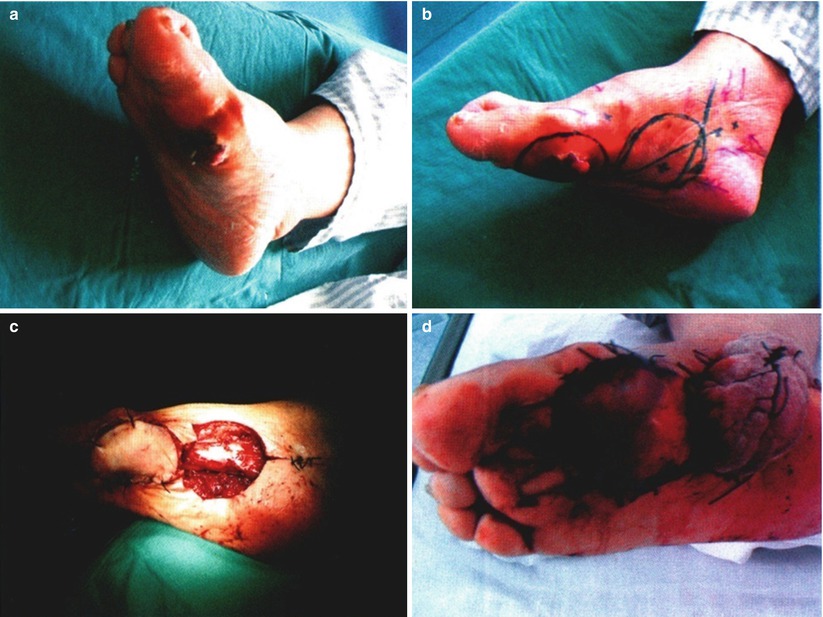
Fig. 18.10
The plantar medial plantar island flap was used to repair the wound in the anterior margin of the foot bottom through retrograde approach. (a) The plantar melanoma before surgery. (b) The incisal margin of the tumor and retrograde medial plantar island flap were designed. (c) After lesion resection, the medial plantar island flap was transferred retrogradely to repair the wound. (d) At 1 week after surgery
- 1)
- (4)
The advantages and disadvantages: The advantage of medial plantar skin flap is that the use of skin flap with a structure consistent with that of plantar skin to repair the heel and the plantar weight-bearing zone can achieve the curative effects of good wear resistance, compression resistance, sensation, and elasticity. The disadvantage is that the venous return of the skin flap venous is poor, attention should be paid to avoiding injuring the veins, and some soft tissues around the blood vessels are preserved as much as possible to ensure venous return; the plantar subcutaneous tissue is more dense and inflexible and has a larger pressure on the pedicle after its transfer; attention should be paid to suture tension and the pressure of the bandaging; if necessary, some subcutaneous tissues may be cut off appropriately; the retrograde transplantation makes this skin flap lose nerve sensation.
- 2.
The fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein: The skin flap design, surgical method, and the advantages and disadvantages can be read in the preceding part of the text.
Case III: The patient had the malignant melanoma in the heel with huge ulceration; the heel after tumor resection was repaired with the fasciocutaneous flap with nutrient vessels of the sural nerve and small saphenous vein (Fig. 18.11)

Fig. 18.11
Case III. (a) The melanoma in the heel with huge ulceration. (b) The fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein was designed before surgery. (c) After the wound was repaired with the fasciocutaneous flap with nutrient vessels of sural nerve and small saphenous vein. (d) At 2 weeks after surgery
2.2.4 Treatment of Lymph Nodes
- 1.
Treatment of regional lymph nodes: The treatment of the regional lymph nodes is still controversial; a retrospective study suggests that the elective lymph node dissection (ELND) is beneficial to increase the survival rate, while another prospective study does not obtain such in conclusion. Generally it is believed that if there are no clinical signs of regional lymph node metastasis, the thickness of the tumor body is less than 1.5 mm; it is inappropriate to carry out ELND; when the thickness of the tumor body is more than 1.5 mm, or the cytology and histology examinations confirm the presence of local lymph node metastasis, the lymph node dissection should be carried out. If the primary lesion is near the lymph nodes, the tumor body and major lymph node should be dissected together. For example, the malignant melanoma in the mid-thigh and the inguinal lymph nodes needs to be removed together. Conversely, if the lesions are below the knee joint, they cannot be treated in this way. But the examination shows that lymph nodes in the site of femoral canal contain tumor cells; it is often required to carry out deep femoral lymph nodes dissection. If the examination confirms the presence of distant metastases, it is not recommended to carry out routine lymph node dissection.
- 2.
Treatment of sentinel lymph nodes: In 1991, the researchers in UCLA (University of California, Los Angeles) injected the isosulfan blue into lower limb skin of the cat. They found that the injection sites are different and the first colored lymph nodes are different, for example, if the injection is performed in the inner thigh, the central group of the inguinal lymph nodes are always colored, while if the injection is performed in the lateral thigh, the lateral group of the inguinal lymph nodes are always colored. Thereby the concept of the sentinel lymph nodes is proposed. The sentinel lymph nodes refer to the lymph nodes reached firstly by the malignant tumor cells breaking away from the primary location.
During surgery, the dyes are intradermally injected near the malignant melanoma, and the firstly stained lymph nodes are found according to the direction of the dye drainage. The immunohistochemistry and (or) PCR examination is carried out for the resected lymph nodes; the detection rate of lymph node micrometastasis can be increased by 40%. The best way to get the sentinel lymph nodes is to carry out preoperative and intraoperative subcutaneous injections of the radioactive tracer technetium-99 m, combined with intraoperative dye tracing; the combination of two factors makes the sentinel lymph node-positive detection rate increased to 95% while making its false negative rate reduced to less than 1%. For positive sentinel lymph nodes, the elective lymph node dissection is performed; if the pathological section examination confirms that the lymph nodes have no tumor cells, then it is believed that other lymph nodes also have no tumor cells. The advantage of this approach is that whether lymph node metastases exist can be revealed, and thus, it is not required to carry out lymph node dissection, which reduces the blindness of the elective lymph node dissection and its secondary damage; meanwhile the pathologist is allowed to carry out multiple stainings for the lymph nodes to increase the diagnostic accuracy.
- 3.
Principles of lymph node dissection
- (1)
The regional lymph node dissection is sufficient.
- (2)
The involved lymph node must be completely removed.
- (3)
In general, the number of lymph nodes which are removed and examined is as follows: ≥10 in the groin, ≥15 in the armpits, and ≥15 in the neck.
- (4)
In the groin area, if the clinical finding shows that the number of metastasized superficial femoral lymph nodes is greater than or equal to three, the iliac fossa and obturator lymph nodes are electively dissected.
- (5)
If the pelvic imaging suggests or Cloquet lymph node is positive, it is required to carry out iliac fossa and obturator lymph node dissections.
- (1)
3 Malignant Tumors Derived from the Mesenchymal Tissue
The malignant tumors derived from the mesenchymal tissue, also known as soft tissue sarcomas, are the most common malignant tumors originating from embryonic mesenchymal tissue. These tumors are insensitive to chemotherapy; therefore, the surgery is still the main method of treatment, and the radiotherapy can be used as adjuvant therapy after tumor resection.
The soft tissue sarcomas are the malignant tumors of soft tissues, including the malignant tumors occurring in adipose tissue, fibrous tissue, muscle tissue, blood vessels, and peripheral nerve tissue. But in view of their distribution, the occurrence scope far exceeds the scope of the abovementioned tissues, for example, the leiomyosarcoma can occur in the skin; this is because the tumor body is derived from the blood vessels of the superficial vascular network or arrector pili muscle in the skin.
3.1 Epidemiological Characteristics
The incidence rate of soft tissue sarcoma is very low, accounting for about 1% of all systemic malignant tumors. The buttocks, thighs, and calves are high incidence areas of soft tissue sarcoma; the soft tissue sarcoma occurring in the three areas accounts for about 40%–50% of soft tissue malignant tumors in the whole body. This kind of tumors rarely has the possibility of canceration of benign malignant tumors. Most soft tissue sarcomas are sporadic.
So far no clear cause has been found. But the studies have found some certain inducing factors, for example, the exogenous rays have the potential to cause soft tissue sarcomas, the radiotherapy can increase the incidence rate of the soft tissue sarcoma by 50 times, the onset time is 3–15 years after radiotherapy, and once the disease onset occurs, the prognosis is poor. Another study found that AIDS patients are susceptible to Kaposi’s sarcoma, and the incidence rate is 310 times that of the general population; the incidence rate of angiosarcoma is also 17 times that of the general population. Some studies have also found that certain occupational causes such as long-term exposure to polyvinyl chloride, phenoxyacetic acid herbicides, and chlorophenol wood preservatives will also increase the incidence rate of soft tissue sarcoma. The dioxin, especially the tetrachlorodibenzodioxin, also has the potential to cause soft tissue sarcomas. The possibility of neurofibromatosis type I developing into malignant peripheral nerve sheath tumor is likely to be ten times higher than that in the general population.
Viewing from the layers where the disease onset occurs, if the deep fascia is taken as the boundary between superficial and deep layers, the soft tissue sarcomas occurring in the superficial layers account for about 15%, while the soft tissue sarcomas occurring in the deep layers account for 85%. Five common histological types include malignant fibrous histiocytoma, rhabdomyosarcoma, synovial sarcoma, liposarcoma, and fibrosarcoma, which totally account for 90% of all soft tissue sarcoma.
3.2 Biological Characteristics
3.2.1 Growth Pattern
The epidemiological characteristics show that the soft tissue sarcoma grows mostly in the deep tissues and usually shows a kind of eccentric growth and spherical enlargement. The compression zone and reaction zone appear around the tumor. The reaction zone presents mostly with tissue edema, neovascularization, and the formation of the pseudocapsule of the sarcoma. This pseudocapsule infiltrated by the sarcoma will be finally changed into the sarcoma and become a part of the sarcoma due to the ingrowth and development of the tumor buds. Then a new pseudocapsule is formed, and the above process is repeated. The pseudopodia, jumping tumor foci, or satellite nodules may occur within normal tissues outside the reaction zone and in the compression zone, and therefore in normal tissue of the incisal margin observed by the naked eye, the microscopic invasion of the malignant tumor is likely to have occurred. This process is repeated to form a multinodular tumor. It is clearly wrong to judge whether the tumor is resected completely or not only with the naked eye.
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
 Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


