Fig. 5.1
Sprayed LN exits, forming a conical pattern. This cone will have a height (h) which corresponds to the distance from the tip opening to the skin, a radius (r) which is the distance from the center of the freezing area towards the periphery, and a side length (s)
Once LN reaches the skin surface, the freezing front advances horizontally on the skin surface as well as vertically (in depth) following an isotherm pattern (Fig. 5.2). Isotherms are temperature zones of equal temperature; the isotherm pattern in skin freezing will have a center where the temperature is the lowest, and the temperature at the periphery where it will be the highest.
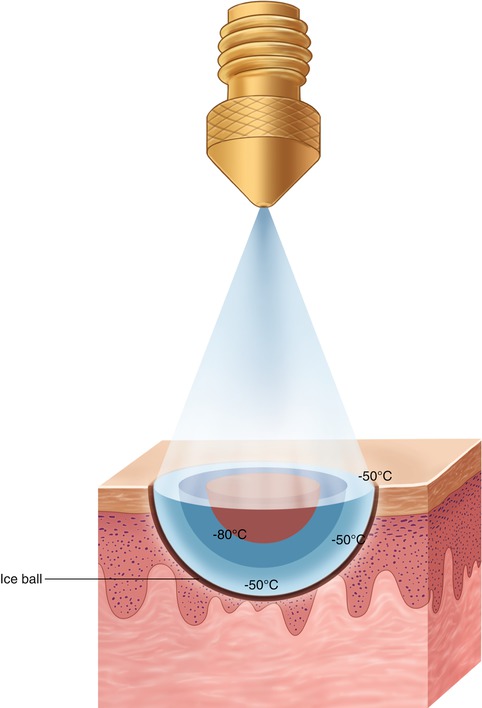
Fig. 5.2
Superficial freezing front extends radially. In depth, it does so in approximately a half sphere with concentric isothermal rings
There are three important points to keep in mind when using the spray technique:
1.
Tip diameter. The amount of released LN will depend on the diameter of the tip opening. Larger openings release more LN. Choose small openings for delicate, superficial freezing and whenever you need to be sure to freeze a small and well-defined lesion (like a lentigo). Large openings are used to freeze large tumoral masses or extended large lesions. A small opening will result in a slower freezing. It will take longer to freeze a lesion (Fig. 5.3).
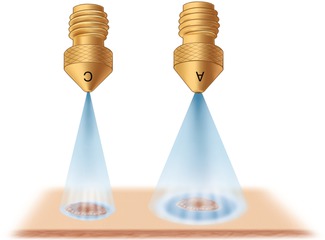
Fig. 5.3
Diameter of aperture. For nozzles placed at the same distance, perpendicular to the skin and different apertures, the larger aperture will release more LN. Freezing will be faster, larger in superficial surface and deeper
2.
Distance. The distance between the releasing tip and the lesion is very important. Since air is a bad conductor, the farther away you spray, the less freezing you will achieve. Furthermore, the spray angle is not constant for larger h (distance to the skin). Since spray coverage will depend on the spray angle, the distance has to be maintained constant. Keep this in mind and always work at the same distance from the subject (Fig. 5.4).
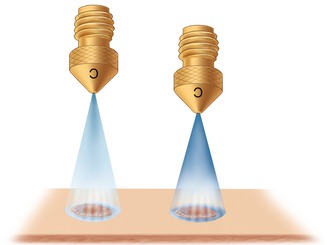
Fig. 5.4
Distance from the skin. For two nozzles with the same aperture, both spraying perpendicular to the surface, the more distant one will freeze less
3.
Inclination. The cone of LN released from a unit parallel to the skin will be spherical. Instead, if the unit is not kept parallel to the skin, it will be an oblique cone. A tilted spraying will result in an irregular freezing: the side closer to the skin will have a lower temperature and therefore experience larger destruction, while the other end will have a higher temperature (less destruction) (Fig. 5.5).
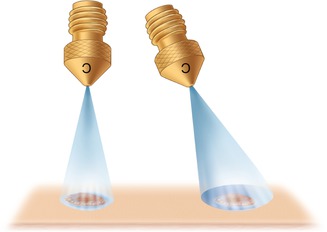
Fig. 5.5
For two nozzles that share the same size of aperture and distance but different positions (one perpendicular to the skin surface and the other tilted), freezing of the tilted spray will cause irregular freezing (colder in the area close to the opening and warmer at the distal extreme)
As LN hits the skin and freezing begins, the skin turns white. With pendular movements (Fig. 5.6), whiteness appears in every area the LN has reached, giving a false freezing front. Pendular movements are used for very superficial freezing, as is the case in cryopeelings. It is a good idea to delineate in advance with a marker the lesion and the margins because freezing (ice whiteness and the edema) can blur the margins.
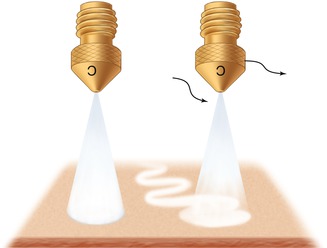
Fig. 5.6
Spraying turns the surface skin white. By freezing without moving the unit, freezing will spread from the center outward. With swinging or brush movements, the skin turns white but for a shorter period since freezing is very superficial
For spray freezing where one needs to guarantee a regular freezing front, it is necessary to maintain a stable freezing at the center and allow it to expand towards the periphery. Maintain the same distance and the same position. This technique has also been called the time spot freeze [2].
Having more than one nozzle helps adjust to different needs. For instance, there is a spray nozzle called advance acne aperture (Brymill®). It produces a spray pattern which appears flat and elongated. It is used for acne lesions, and it is particularly useful for cryopeelings.
The open technique is ideal in:
Superficial flat lesions, like lentigos solaris
Dome-shaped or thick lesions, such as seborrheic keratosis or small keloids
Superficial freezing for cryobiopsy (Chap. 7)
Irregular tumoral masses where the irregularity of the surface would not enable probe use
The open technique should be avoided in:
Protruding skin lesions (like skin tags). Freezing elongated lesions with the open technique will cause an unnecessary rim of healthy skin to freeze, with a resulting hypo- or hyperpigmented spot.
In orifices (nose, mouth).
In vascular lesions unless you freeze in an intermittent manner and allow the freezing front to advance slowly until it reaches the bottom (see the discussion of the pyogenic granuloma technique in Chap. 12).
5.2.1.1 Advantages
It tends to be quicker and less laborious than other techniques.
It is especially convenient in multiple lesions, such as seborrheic keratosis.
Since there is no contact, there is no risk of sticking on the surface and over-freezing. Once the spraying stops, thawing begins.
It is ideal when treating irregular bulky tumors that cannot be curetted.
Since there is no contact, it is the safest technique. There is no contact with blood or other secretions.
5.2.1.2 Disadvantages
Swinging the unit as you freeze can cause false freezing fronts and yield the wrong impression of having frozen the whole lesion at the expected temperature.
Distance and tilting is operator dependent and will change the outcome of a procedure.
Its initial impact on the skin, once freezing starts, can startle the patient.
Peri lesional LN spattering is possible which might cause discomfort.
5.2.2 Semi-open Technique
It is as a variation of the spraying technique [3] in which the released spray is constrained into one area. The limits are set by a rubber cone, the opening on a lexan plate, or an otoscope disposable specula tip (Fig. 5.7). Metal cones should never be used because they are excellent conductors of cold and they will get stuck to the surface, causing addition destruction.
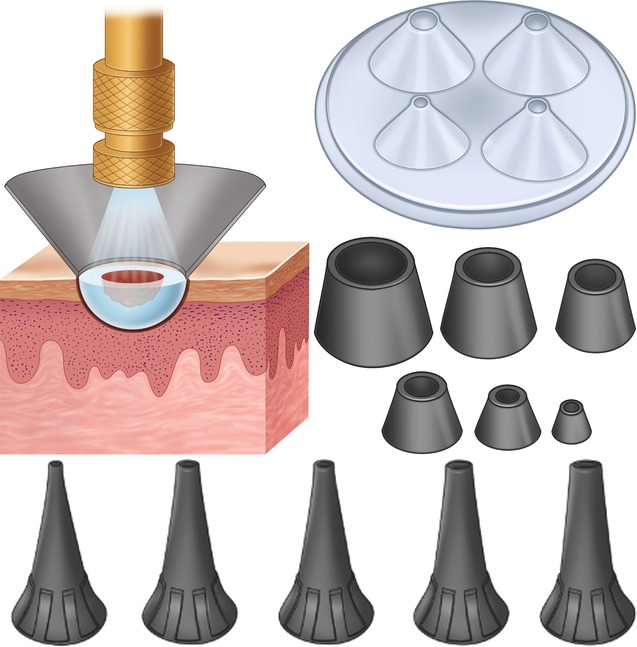
Fig. 5.7
Sprayed LN can be confined with lexan plastic plates, rubber cones, or otoscopes
Concentrating LN in a limited area will cause faster and deeper freezing.
The opening of the attachment has to fit the lesion. If it is too large, you will be freezing unnecessary healthy skin. If it is too small, the entire lesion will not be included.
It is the ideal for:
Small warts or molluscum contagiosum
It should be disregarded if:
You do not have a cone of the correct size or the cone or aperture on the lexan plate.
5.2.2.1 Advantages
Freezing is faster.
It is less painful. Part of the pain sensation might be caused by the splashing (spattering) of the LN drops over the healthy skin. This problem is reduced by having the lesion restrained within the cone. Part of the pain is also believed to be due to sputtering caused by LN “boiling” from liquid to gas [3].
Children are distracted by the presence of the lexan plate or specula. They seem to tolerate the procedure better. It sometimes gets stuck for a few seconds and that amuses them.
Costrainers are usually easily available.
5.2.2.2 Disadvantages
Need to have the proper constrainer that adjust to the size of the lesion.
It is limited in use to lesions of up to 6–8 mm.
There is no visibility of the superficial freezing front.
5.2.3 Close or Probe Technique
This technique is performed by using probes, which are closed-circuit systems into which LN travels from the unit and finally exits through a rubber hose [4].
They are built with metal and some are Teflon-coated to reduce the risk of sticking to the surface of the lesion. Freezing is constant, not dependent on the operator because they contact the skin. Distance is not an issue because it is also a constant given by the size of the probe. Since metal is an excellent conductor of cold, probes freeze very fast, and the freezing front is deeper than the one obtained by spray freezing (Fig. 5.8a, b).
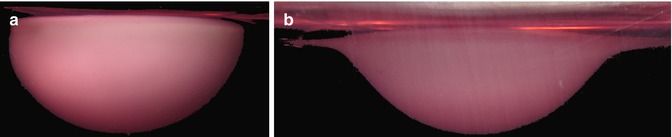
Fig. 5.8




(a) Freezing with a probe will cause a half sphere freezing ball. (b) With the spraying technique, the shape is more like a hat: deep in the center and thinner at the periphery. The final depth in probe freezing is deeper (4 × 2) than in spray freezing (4 × 1.5)
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
