Fig. 18.1
The so-called H-zone of the face is a high-risk area in which the risk for tumor recurrence is about double compared to other regions, irrespective of therapy. The malignancy may grow with silent outgrowths in the dermis, along the perichondrium, the periosteum, and the nerve sheaths
18.2 Patient and Tumor Selection
Before treatment of a malignant tumor, a primary decision must be made concerning the aim of the therapy, namely, cure or palliation. The second decision will be which type of treatment will be the most appropriate in this particular patient. The age and state of health of the patient are important. The histopathological type of tumor, the size of the lesion, and its location are other factors of importance in the choice of therapy.
It is always important to choose the most convenient and safe treatment. Cryosurgery is only one of different therapeutic possibilities.
18.3 Equipment
Liquid nitrogen is the only effective cryogen in the cryosurgical treatment of malignant tumors [17]. In routine clinical practice, liquid nitrogen spray equipment has become the most frequently used device. The most popular units are small handheld, metal or plastic vacuum flasks with four spray tips, with diameters ranging from 0.375 to 1 mm (labeled A, B, C, and D). The author always uses a handheld Cry-Ac (Brymill Corp., New York, USA) with nozzle B.
Additional equipment used in cryosurgery includes cryoprobes, spray-limiting cones of various sizes, protective items, temperature-monitoring devices (not used by the author), stopwatches, ring curettes of different sizes, scissors, punch, scalpel or razor blade, electrosurgical unit, local anesthetic, and hemostatic agents (50 % iron chloride solution) [18]. The equipment used by the author is seen in Fig. 18.2.

Fig. 18.2
The equipment used in the treatment by curettage-cryosurgery
18.4 Techniques of Cryosurgery
The aim when treating a malignant tumor must be that the first treatment should be the final one. In the treatment with cryosurgery, the tumor has to be frozen sufficiently so that no malignant cells persist.
During the first decades of modern cryosurgery (1960–1970), the goal was a tissue temperature of −20 to −25 °C at the base of the tumor. However, during recent decades, there has been a trend toward a more aggressive treatment with lower temperatures in the range between −40 and −60 °C and a greater use of debulking techniques [19–22]. The freezing time depends on the technique used. With a spray freezing intermittently, about 60 s is needed; with the spot freeze method, about 30 s is needed; and after a thorough curettage, an even shorter freeze time will be adequate for a 1 cm lesion [5, 21–26]. For a larger tumor, the freeze time will increase. In a malignancy larger than 2 cm, the freezing may be divided and applied in sections of the tumor [27]. A double, sometimes even a triple, freeze-thaw cycle should always be performed. This is especially true for tumors in high-risk areas such as the nose and ears.
To register the exact temperature (−50 to −60 °C), some cryosurgeons employ thermocouples at the base of the tumor. Temperature measuring is especially useful for deeper tumors and those in critical locations [28].
Many cryosurgeons do not measure the temperature because an interrelationship exists between the freeze time, the lateral spread of freeze, and tissue temperature, and the adequacy of treatment is based on these [5]. The author uses a special cryosurgery chart with registration of total freeze time, lateral spread of freeze (should be ≥ 5 mm), halo thaw time (should be ≥ 60 s), and total thaw time [21].
Protection in the freezing of tumors close to the external ear canal and the nostrils is needed, and soft cotton is appropriate.
18.5 Indications of Cryosurgery
In general, depending on the cryosurgical technique used, most BCCs – except the morphoeiform types and the recurrent BCCs with secondary sclerosis – are effectively treated by cryosurgery [21–26]. Many SCCs – especially well-differentiated SCCs arising in actinic keratosis and SCCs in situ – are also well suited for cryosurgical treatment [28, 29]. Those tumors overlying cartilage on the nose and ears are often most suitable for cryosurgery, even if they are located in high-risk areas. Cartilage and bone are resistant to freezing injury, and the architecture of the organ is preserved [30, 31].
Unfortunately, the tumors in these areas are often clinically ill defined and thus unsuitable to be treated by cryosurgery alone [29]. However, provided most of the tumor could be removed by curettage and the limits demarcated by a “heavy-handed curettage” [32], cryosurgery would be a suitable therapy, even if any tumor extensions were left behind [20–22]. These remaining outgrowths will then be erased by the freezing with liquid nitrogen in a double freeze-thaw cycle without destroying the stromal framework (Fig. 18.3a–c). A great advantage of cryosurgery on the nose and ears is that stromal tissues such as the cartilage and bone are less cold sensitive than cellular elements [30, 31]. In the healing process, these tissues will serve as a framework [31]. Besides, BCC very rarely invades cartilage or bone [33].
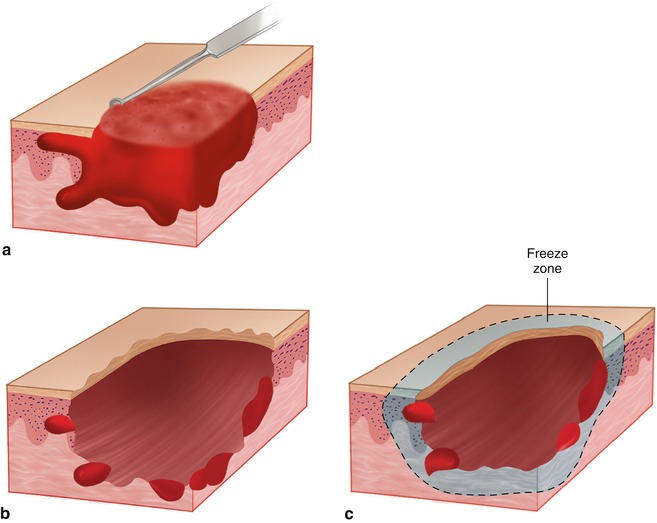
Fig. 18.3
A general outline of curettage-cryosurgery of a nonmelanoma skin cancer. (a) Curettage. (b) After a thorough curettage, there are still tumor extensions left behind not reached by the curettes. (c) Freezing with liquid nitrogen with a lateral spread of freeze of ≥5 mm in a double freeze-thaw cycle will erase any remaining tumor offshoots
18.6 Contraindications of Cryosurgery
There are no absolute contraindications for cryosurgery except known cold intolerance. Morphoeiform and sclerotic recurrent BCCs are unsuitable for this therapy because the fibrosis does not permit a proper “feeling” of the curettage. Many aggressive tumors in difficult areas, such as the nasolabial fold and the inner canthi and pre- and postauricular fold, are preferably treated with other methods for higher cure rates and better cosmetic results [34].
18.7 Patients
After clinical examination and measuring of the visible size of the tumor, one or more punch biopsies are taken for verification of the diagnosis. Based on the histopathological findings, the morphoeiform tumors are always referred for MMS, and selected tumors of other types are treated by curettage-cryosurgery (CC). According to the present definition, morphoeiform BCC includes fibrosing, sclerosing, and scirrhous types of BCC.
18.8 Author’s Method
18.8.1 Curettage-Cryosurgery
A thorough curettage using ring curettes (Thiemann, New York, USA) is performed under local anesthesia (mepivacaine-adrenaline 10 mg/ml + 5 μg/ml). At first, a large curette (no.3) is used to remove the bulk of the tumor and then a medium-sized one (no.2), and finally a small curette (no.1) is used to remove any extensions of the malignancy. The curettage material is also sent for histopathological examination, and sometimes the findings are more aggressive than the original one [35]. After meticulous curettage, the tumor is often found to have wider lateral extension and greater depth than expected, and one has to be particularly thorough when treating malignancies in the nasolabial folds, in the inner canthi, and in the pre- and postauricular sulci. The curettage is performed according to the technique described by Strum and Leider [32]. Sometimes undermined edges have to be cut off by a pair of scissors. A cotton stick dipped in 50 % iron chloride solution is used for hemostasis.
Freezing is carried out with a maximal continuous spraying of liquid nitrogen (−196 °C) using a handheld Cry-Ac (Brymill Corp., New York, USA) with the nozzle held as horizontally as possible and, in general, with the patient sitting. By using the vertical position, the problem of liquid nitrogen flowing on the lesion is avoided, and the spraying becomes more standardized. The tumor area is most often, especially on flat surfaces, demarcated by a neoprene cone of appropriate size. The spray tip, size B, is moved in circular motions over the treatment zone, at about 1 cm distance, until the lateral spread of freeze has reached a minimum of 5 mm outside the tumor border or 1–1.5 mm outside the neoprene cone. The skin is always well fixed to the underlying bone by the freezing in spite of the “ballooning” of the local anesthesia. For tumors overlying cartilage on the nasal ala or the pinna of the ear, the freezing continues until the opposing side is frozen.
The goal of the freezing is a fast cooling rate and a slow thawing rate [5]. The procedure is always repeated a second time.
On a special tumor chart registration of the freeze time (10–25 s, depending on the tumor size), the lateral spread of freeze (≥5 mm), the halo thaw time (at least 60 s), and the complete thaw time (2–5 min) are done but no thermocouples are employed. A therapeutic sequence of curettage-cryosurgery of a clinically ill-defined BCC on ala nasi is seen in Fig. 18.4a–e. The same procedure of a BCC on the dorsal aspect of an ear is seen in Fig. 18.5a–e. All treatments are performed at a single outpatient visit.
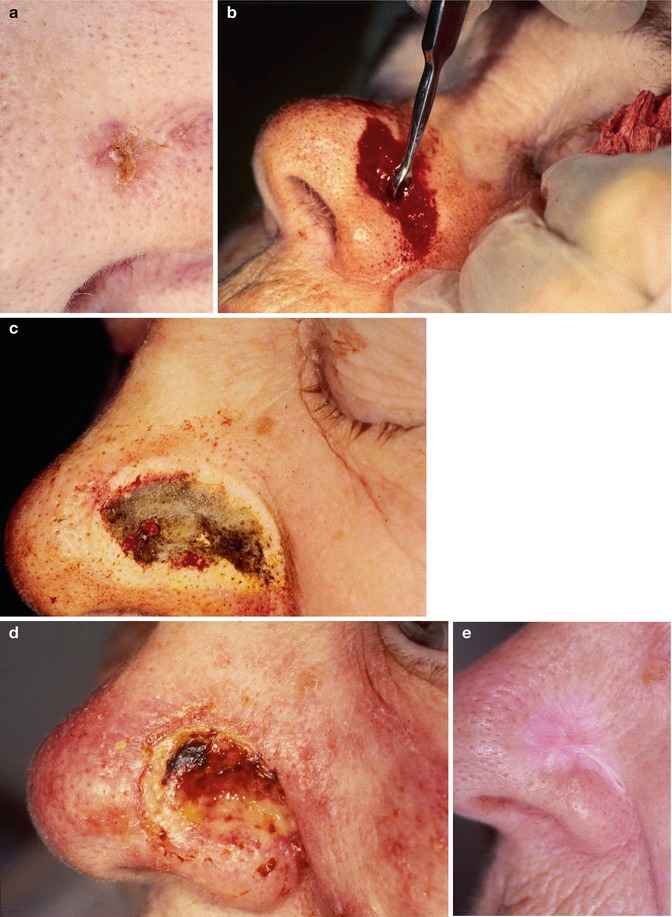
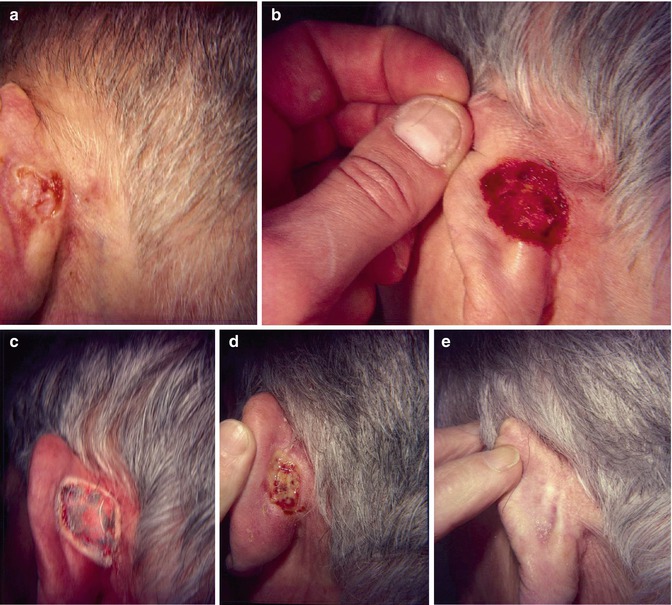
Fig. 18.4
Curettage-cryosurgery of a clinically ill-defined basal cell carcinoma on ala nasi. (a) Before treatment. (b) After a thorough curettage, the tumor is much larger than expected. (c) The tumor area is frozen with liquid nitrogen with a lateral spread of freeze of at least 5 mm. (d) The result after 2 weeks. (e) The result after 5 years
Fig. 18.5
Curettage-cryosurgery of an about 20 mm ulcerated BCC on the dorsal aspect of an ear. (a) Before treatment. (b) After a “heavy-handed” curettage with different-sized curettes, the diameter is 28 mm and four deeper cavities reaching the cartilage are seen. (c) Freezing with liquid nitrogen in a double freeze-thaw cycle. (d) Healing by secondary intention after 2 weeks. (e) The result obtained after 6 years
18.8.2 Complications
It is important to be aware of and inform the patient about the usual and expected postoperative tissue response. Written information about this is handed over to the patient. The incidence of complications is low. They may be classified as temporary or permanent. Pain during and immediately after cryosurgery is common. It may be quite intense but it is usually transient. Edema, especially periorbital, is also very common. However, infection rarely occurs. Of the permanent complications, the most common is hypopigmentation. Retraction of tissue and tissue defects as notching of ala nasi may be seen after treatment of tumors overriding the rim of ala. Notching of the ears may occur after treatment of malignancies overreaching the helix. Other complications are rare [34, 36].
Related posts:
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Theoretical Principles of Immunocryosurgery
Theoretical Principles of Immunocryosurgery
 Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


