Fig. 19.1
Different-sized chalazion forceps that can be used to stabilise the tissue

Fig. 19.2
Cone squeezed to an oval to fit the extension of the tumour
A clear plastic Jaeger lid plate is inserted in the eye fornix to protect the eyeball. There are different types of these plates on the market, but it is important that the plate should be thick enough to well isolate the underlying tissues (the eye) during the treatment (Fig. 19.3). Depending on the site of the tumour, the plate is placed vertical in tumours in the central parts of the upper or lower eyelids and horizontal in tumours that are medial or lateral (Fig. 19.4). The plate should be slightly lifted from the globe during the treatment, thus pressing the eyelid towards the cone and further ensuring that no leaked nitrogen can reach the eye (Fig. 19.5). If the tumour is situated far medial (e.g. covering the area above the lacrimal sac), the plate can be placed horizontally on top of the closed eyelid.



Fig. 19.3
Plastic Jaeger lid plate thick enough to protect the underlying tissue
Fig. 19.4
Lid plate positioned horizontally to protect the eye while treating the medial part of both the upper and lower eyelids
Fig. 19.5
Lid plate lifting the eyelid against the neoprene cone
The liquid nitrogen coolant, stored in a handheld thermos, is sprayed into the rubber cone. To avoid freezing the fingers that hold the cone, a space with air should be left in the fingertips of the gloves (Fig. 19.6). It is important to freeze without interruption to ensure the freezing is reproducible. The freezing should continue until a small brim of frozen tissue is observed all around the outer border of the neoprene cone. A typical freeze time to achieve the desired extension of iced tissue is 20–30 s of constant freezing. The cone is left until it loosens spontaneously from the skin. The halo, corresponding to the 3 mm mark of the wall of the cone, should be allowed a thaw time exceeding 60 s (Fig. 19.7a, b). The frozen area is left to thaw completely. Two freeze–thaw cycles are carried out. If the halo thaw time is less than 60 s, a third cycle is performed.

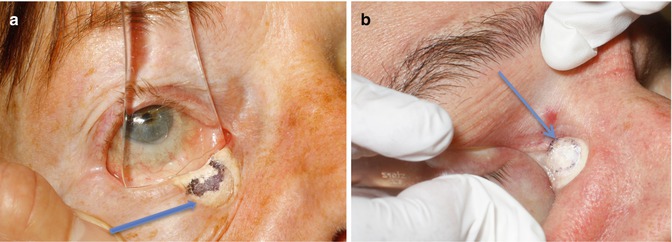
Fig. 19.6
Liquid nitrogen sprayed in the cone; observe the residual air in the fingertips of the glove
Fig. 19.7
The halo thaw time is the time measured from cessation of freezing to the point at which the thawing has reached any part of the inner aspect of the mark of the cone; in the figures, this is pointed out by the arrow (a, b)
After the treatment, an antibiotic ointment is placed in the eye.
19.3 Patient Information
Patients are carefully informed about the procedure. It is particularly important to inform patients about excessive postoperative swelling and oozing of tissue fluid. There are more local reactions in larger tumours than in small ones (Fig. 19.8a, b). Usually, there is little pain. Patients are told that it looks worse than it feels. The swelling may be misinterpreted as infection by those not familiar with its appearance. Antibiotic ointment should be applied in the eye for as long as there is a crust. Patients are encouraged to allow the treated area to get damp during showering, because this facilitates the loosening of the crust, which will then be replaced by a smaller one. The healing period is about 1 month in tumours of 10 mm size. Patients are told about the risk of conjunctival overgrowth and hypo- or hyperpigmentation in the treated area.
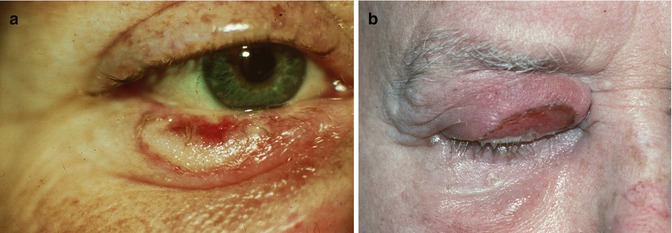
Fig. 19.8




Reaction after 1 week in a small tumour (a) and in a large tumour (b)
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
