Suggested technique
Noninfectious conditions
Acne (cysts)
S
Alopecia areata
S
Benign pigmentary lesions: lentigines, lentigos simplex, solar lentigos, ephelides
S
Dermatofibroma
P, SO
Ingrowing toenail
P, S
Granuloma annulare
P, S
Keloids
S, P, IL
Lichen planus
S
Myxoid cysts
P, S, SO
Prurigo nodularis
S
Seborrheic keratosis
S
Sebaceous hyperplasia
P
Skin tags
T, S
Trigeminal neuralgia
P, S
Pearly penile papule
S, P
Vascular lesions (see Chap. 12)
P, S
Infectious conditions
Chromomycosis
S
Molluscum contagiosum
P, SO
Leishmaniasis
S
Larva migrans
P, S
Warts (see Chap. 9)
S, SO
8.2 Acne
Although cryosurgery is not a first treatment modality in acne cysts, it can be the sole alternative when dealing with patients with severe cystic forms of acne that cannot be treated either with oral or with topical medication. Such is the case in pregnancy [2].
Cold has an initial inflammatory effect, but 24–48 h after freezing the lesion an anti-inflammatory effect becomes evident and a faster reabsorption of the lesion occurs. A superficial spraying for 5–7 s is usually enough: freezing beyond the margin of the lesion is not necessary. In order to avoid LN insufflations, spraying before draining the lesion is advisable.
8.3 Rhinophyma
Cryosurgery has been an excellent option [3–5] for rhinophyma where good cosmetic results have been reported. Two or three freeze-thaw cycles of 15–30 s separated by 1 min are recommended. Sessions can be repeated every 2 weeks for up to seven sessions [6]. Another alternative is to shave the excess tissue (previous local anesthesia) using electrosurgery and later deep spray, freezing the base of the lesion.
8.4 Alopecia Areata
Some authors report the use of cryosurgery in alopecia areata. LN can be applied either by cotton swab technique [7] or by superficially spraying the lesion until the skin turns slightly pinkish red. No blister should be induced. Besides the slight discomfort from cold, pain is not a major complaint. Apparently it works by inducing local vasodilation or even by cold immunomodulation.
8.5 Benign Pigmentary Lesions: Lentigines, Lentigos Simplex, Solar Lentigos, and Ephelides
Freezing for 5–7 s, using a superficial spray technique (open method), until the whole pigmented area and an additional 1–2 mm margin are included in the treatment zone is recommended [8].
The aim is to cause a sloughing of the superficial pigmented epidermis. No destruction of melanocytes occurs because freezing is very light. Likewise, recurrence can occur if no proper sun protection follows treatment, just as it occurs with any other surgical treatment of pigmented lesions. Lentigos in the dorsum of the hand leave very satisfactory results although the patient must be warned that the complete healing process can take over a month. Lentigos in the dorsum of the hands have to be spray-freezed for a few seconds each. The crusts can take up to a month to fall off and the pink residual spots can take up to 2 months.
Special consideration should be taken in darker skin types as even a light freezing can result in hyperpigmentation. Do not ever use it in melasma.
8.6 Dermatofibroma
Although it is possible to treat dermatofibroma with cryosurgery, this lesion has a deep dermal fibrous component that requires a deep freezing (contact/probe). In certain skin types, hyper- or hypopigmentation can make the result unsatisfactory. Lesions located on the legs require healing times that may exceed 2 months, making a simple excision with conventional surgery a better technique. Dermatofibromas that respond well to a cryosurgical treatment include lesions that are small, not too elevated, and nonpigmented lesions located above the waistline [9].
8.7 Ingrown Toenail
Ingrown toe nail or onychocryptosis is related to congenital or to acquired defect of the toenail (inadequate shoes or improper nail cut). This condition might be present at birth but frequently makes itself evident in early adulthood. In patients with congenital conditions in whom the presence of granulomas is persistent or recurrent, a partial or total surgical nail removal or a surgical ablation of laterals and/or distal nail folds is the best therapeutic approach. A conservative approach is an option for those granulomas that are present in acquired cases. Cryosurgery is an excellent option that avoids the need for conventional nail surgery. If skin infection is present, a previous topical antibiotic is recommended. One cycle of cryosurgery with a previously frozen probe (closed method) or one cycle of LN spraying (open method) with a 1 mm margin is usually enough to destroy the granuloma. Combination treatments (cryosurgery plus matrixectomy) have been reported with good results [10].
8.8 Granuloma Annulare
Single lesions of granuloma annulare sometimes disappear after biopsy. Sometimes this phenomenon is also observed when freezing a portion of the border of the lesion, using a probe or spraying LN directly into the lesion. It is an option in children with lesions that do not respond to topical treatment [11].
8.9 Keloids and Hypertrophic Scars
These scars are considered benign proliferations of fibrous tissue composed mainly of collagen. For keloids, the stimulus that triggers could be any type of trauma to the skin and may not even be present or evident. Keloids have an accelerated growth pattern and by definition occupy a much larger area than that of the corresponding area of trauma or initial stimulus. Keloids tend to grow, creating finger-like projections or pseudopods. In the case of hypertrophic scars, a history of trauma to the skin is present and the fibrous tissue becomes bulky, but generally it does not exceed the corresponding area of the initial trauma [12].
It is known that keloids are more common in people with darker skin phototypes, but they have been reported in all races. Keloids have a predilection to appear in certain anatomical regions such as ears, chest, shoulders, neck, and abdomen, among others [12].
Whichever method is used, the treatment of keloids is difficult and sometimes unrewarding due to the high recurrence rate. When treated with simple surgical excision, recurrence rates of approximately 55 % have been reported [12].
Cryosurgery has proved to be useful in the management of both keloids and hypertrophic scars. It has been observed in vitro that freezing human living skin modifies collagen synthesis by promoting the differentiation of keloid fibroblast into normal phenotype fibroblasts. Recurrence varies with reports, but better results are obtained when used in combination with intralesional steroids, which decreases collagen synthesis and increases its degradation [13, 14].
The form of application varies according to the size of the lesion and its anatomical location. In small lesions, an open method or spray can be used. Choosing an adequate tip that allows a sufficient cryogen flow is important to achieve a rapid and solid freezing. Repeat the procedure 2–3 times for better results. In large and bulky lesions and in certain anatomical regions such as ear lobes, a thick needle or cryoneedle can be inserted in and through the lesion. The needle is attached to a cryosurgery device directly or using a Luer-Lock adapter; as the cryogen passes through the needle, the freezing of the lesion occurs from the center to the periphery allowing a solid freezing, including the center of the lesion. A mild bleeding at the puncture sites might occur which can be controlled by applying pressure for a few minutes (Fig. 8.1a–c) [12, 13].
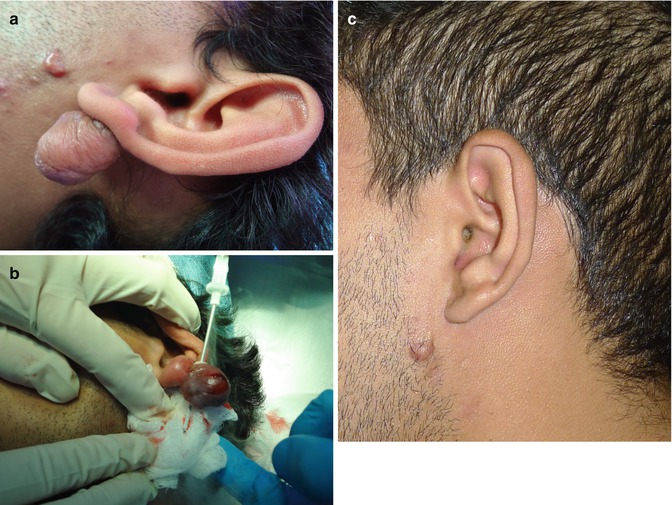
Fig. 8.1
(a) Large keloid on the earlobe. (b) Intralesional cryosurgery followed by corticosteroid infiltration. (c) End results
Using intralesional corticosteroids after the cryosurgery seems to warrant better results and diminishes the risk of recurrence. Some authors suggest that the benefit of using this combined treatment is due to the sum of the mechanisms of action of both therapeutic methods. However, it seems easier to infiltrate the corticosteroid into the fibrous tissue a few minutes (10–15 min) after the last freeze-thaw cycle, apparently due to keloid tissue edema. A higher volume of the drug can be injected into the tissue after the freezing compared with the amount that can be injected without a previous cryosurgery. Triamcinolone is the preferred corticosteroid; infiltration of the maximum amount of undiluted triamcinolone (10 mg/ml) that the tissue can sustain is advisable. Figueroa et al. reported 80–100 % reduction in 75 % of the lesions, 50–80 % reduction in 16 % of the lesions, and one patient with a recurrent lesion after 1 year of follow-up, using a technique that included shaving, cryosurgery with an open method, and intralesional steroid injections [15]. Zouboulis et al. reported an excellent response in 32.3 %, a good response in 29 %, and a poor response in 9.7 % of patients treated with a contact method with freeze-thaw cycles of 30 s and repeating the procedure every 20–30 days if needed; there were no recurrences [16].
An important tissue necrosis is an unavoidable event since a solid and complete freezing is of paramount importance in treating this kind of lesions. However, achromic and hypopigmented scarring of the skin may be present in the final cosmetic result. Notifying patients in advance of this postoperative possibility is very important.
8.10 Myxoid Cysts
Myxoid cysts (in hand or toes) can be treated with cryosurgery using LN spray [17] (open technique) or probe (closed technique) [18]. A double freeze-thaw cycle is recommended by some authors [19]. Local infiltrative or troncular block anesthesia is recommended. A small incision is made in the center of the lesion in order to drain its content-a viscous mucous-like material. It also confirms the diagnosis. A previously frozen probe or a warm probe (to help fix into place) is applied with pressure. Freezing should extend 1 mm beyond the borders of the lesion. Generally, one cycle is sufficient (Fig. 8.2a–d). Recurrences are possible.

Fig. 8.2
(a) Myxoid cyst on second toe of right foot. (b) Drainage of viscous content to confirm diagnosis. (c) One cycle deep probe freezing with 4 mm probe. (d) Four months later
8.11 Prurigo Nodularis
One cycle of LN superficial spraying is usually enough. It is an option used in other inflammatory conditions such as psoriasis and lichen planus among others [20].
8.12 Seborrheic Keratosis (SK)
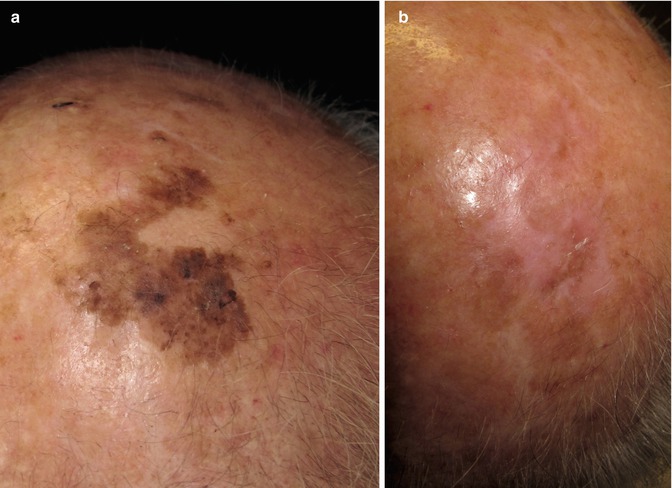
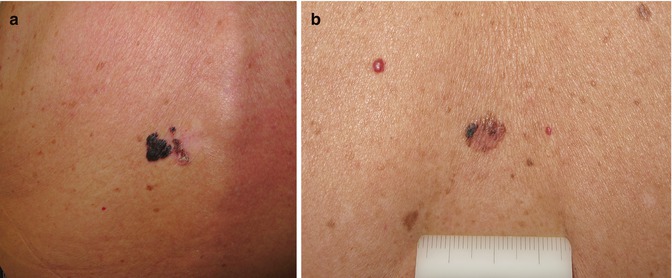
SK is probably the most gratifying lesion to treat with cryosurgery (Fig. 8.3a, b). In fact, cryosurgery stands as the first treatment option, and one can hardly think of any other surgical alternative that gives such results. Many lesions can be treated at once, with low cost and in a time-saving procedure to the patient. SK can have many presentations as far as morphology: thin, thick, large, small, and hyperpigmented. Sometimes, they can mimic malignancies (Fig. 8.4a) (as basal cell carcinomas or melanomas) and vice versa (Fig. 8.4b). This enhances the importance of having a correct diagnosis before freezing. Dermoscopy plays an important role in making the right choice with these patients, since dermoscopic characteristics of SK are distinctive and allow for a correct diagnosis in most of the cases. A biopsy is mandatory in cases when the clinician is unsure about the diagnosis.
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Role of Reflectance Confocal Microscopy in Cryosurgery
Role of Reflectance Confocal Microscopy in Cryosurgery
 Theoretical Principles of Immunocryosurgery
Theoretical Principles of Immunocryosurgery
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions




Fig. 8.3
(a) Seborrheic keratosis of the scalp. (b) Three months after treatment, one freeze-thaw cycle, open technique
Related posts:
Preoperative Care for Cryosurgery
Role of Reflectance Confocal Microscopy in Cryosurgery
Theoretical Principles of Immunocryosurgery
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
Cryosurgery for Warts
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
