Oral cavity is easily accessible
The moisture of the mouth and the soft tissue favor the rapid spread of ice ball
Possibility of using a local cream for anesthesia
Ease of postoperative follow-up and possibility of reapplication in case of residual disease
Minimum risk of postoperative bleeding
Postoperative infections are rare
Complications are rare
Healing is good
Cure rates are high
Table 10.2
Cryosurgery in benign oral diseases
Disease | Indications | Freezing time |
|---|---|---|
HPV disease (Warts, condylomata acuminata, papillomas, focal epithelial hyperplasia) | + + + | 10–20 s |
Fibroma | + + | 15–20 s |
Mucocele | + + | 10–20 s |
Pyogenic granuloma (as long as it is a confirmed diagnosis) | + | 20–30 s |
Venous lake | +++ | 15–30 s |
Palatal papillary hyperplasia | + | 30 s |
Melanocytic macules of the lower lips | ++ | 3–5 s |
Lymphangioma | ++ | 15–20 s |
Hemangiomas (mostly small) | +++ | 15–20 s |
Familial acanthosis nigricans | +++ | 15–20 s |
Median lip fissure | + | 10 s |
10.4 Cryosurgical Techniques for Oral Cavity
Generally, for a lege artis cryosurgical procedure, a proper diagnosis, a good understanding of the basic principles of cryosurgery, a written consent from the patient, adequate illumination, use of sterilized equipment (probes, tips), and a chronometer are required.
For cryosurgery with LN as cryogen, we use the dipstick technique, the open (spray) or semi-open (cone) technique, and mainly the close (probe) technique [2].
Selection of the candidate lesion, its location in the oral cavity, its size, and the number of lesions are critical for a favorable result.
Selection of cryogen (liquid nitrogen vs. nitrous oxide) depends on several reasons. In general, nitrous oxide (NO) is preferred for benign oral lesions. Selection of a cryogen will depend on the experience of the cryosurgeon, availability of cryosurgical equipment, and location, size, and infiltration of the lesion. For instance, in lesions on the lips and posterior oral cavity, both cryogens can be used. For lesions located in the posterior oral cavity NO is used (better control of the technique, avoidance of the liquefaction of LN). For small and superficial lesions, nitrous oxide is preferred. For example, NO is used for superficial mucoceles in children, while LN–CryoProbe technique is preferred for venous lake in the lips [9, 10].
10.5 Cryosurgery as First-Choice Treatment in the Oral Cavity [4, 5, 7, 11, 12]
There are a number of lesions where cryosurgery stands as the first choice of treatment. It gives extremely satisfactory results in less than a week with almost no scar. The postoperative procedure is very simple, and no local anesthesia is required. It is an office procedure that takes very little time. The treatment protocol is suggested in Table 10.3.
Table 10.3
Treatment protocol
Name |
Address |
Date |
Clinical photograph (before treatment) |
Diagnosis |
Location and size of the lesion |
Histologic examination (if needed) |
Technique |
Freezing and thaw time |
Cryogen used |
Complications |
Follow-up |
Clinical photograph (after treatment) |
The lesions are:
1.
Venous lake
2.
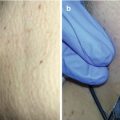
Small hemangiomas (Fig. 10.1a–c)

Fig. 10.1
(a) Hemangioma on the right buccal mucosa. (b) Treatment with close (probe) technique, freezing time: 15 s; double freeze-thaw cycles. (c) 1 year later
3.
Lymphangioma
4.
Get Clinical Tree app for offline access

Mucocele (Figs. 10.2a–d and 10.3a, b)

Fig. 10.2
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Theoretical Principles of Immunocryosurgery
Theoretical Principles of Immunocryosurgery
 Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions




(a) Mucocele on the lower lip. (b) Close technique (probe), freezing time: 15 s; double freeze-thaw cycles. (c) 1 year later. (d) 4 years later
Related posts:
Preoperative Care for Cryosurgery
Theoretical Principles of Immunocryosurgery
Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
Cryosurgery for Warts
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree