Abstract
A myriad of products exist to adorn and maintain the skin, hair, and nails. These products possess sophisticated formulations that can play a role in the maintenance of these structures, but are also capable of inducing or exacerbating disease. Skin care products consist of cleansers, moisturizers, and cosmeceuticals while hair care products consist of shampoos, conditioners, and styling products. Nail care products are used primarily for adornment. For cosmetics and cosmeceuticals, common themes are the need to keep the anatomic structure clean, the need to maintain the water content within the structure for physiologic purposes as well as for beautification, and the need to produce appearance alterations based on fashion trends and personal expression. This chapter examines cosmetics and cosmeceuticals from both a functional and a fashionable standpoint.
Keywords
facial foundation, lipstick, blush, eye shadow, mascara, shampoos, conditioners, styling products, nail polish, nail sculptures, functional cosmetics and moisturizers
- ▪
Colored cosmetics and skin care products have an important role in the prevention of dermatologic disease and the maintenance of skin health
- ▪
Hair is a non-living structure whose appearance and behavior can be improved via the use of shampoos and conditioners
- ▪
Nail cosmetics primarily adorn the nails, but improper use can lead to nail disease
- ▪
Cosmeceuticals are non-prescription products designed to improve the functioning of the skin, primarily by targeting the aging process
- ▪
Skin, hair and nail care products have a profound impact on these structures, and they should be part of the working knowledge of every dermatologist
Introduction
Cosmetics and skin care products are assuming an increasingly important role within dermatology as the sophistication of raw materials and the resulting formulations provide for the development of products that impact the functioning of the skin. It was traditionally thought that the stratum corneum was a non-living, biologically inert layer of the skin upon which skin care products and cosmetics impinge. It was also thought that the stratum corneum was a complete barrier unaffected by the application of non-prescription topical agents. An improved understanding of stratum corneum function, primarily obtained through the use of non-invasive bioengineering techniques, has demonstrated that the stratum corneum can be dramatically influenced by non-prescription topical agents, and that these agents can indeed penetrate the stratum corneum and influence skin function.
Recognition of the biologic importance of the stratum corneum to skin health led to the development of a new category of skin care product, referred to as the cosmeceutical . A cosmeceutical is a scientifically designed, useful product intended for external application to the human body that has desirable aesthetic effects and meets rigid chemical, physical and medical standards . Even though many cosmeceuticals currently exist for use on the skin, hair and nails, there is no regulatory description that acknowledges the current scientific sophistication of these formulations. Rather, a cosmetic is defined by the US Federal Food, Drug and Cosmetic Act, written in 1938, as “articles intended to be rubbed, poured, sprinkled, or sprayed on, introduced into, or otherwise applied to the human body or any part thereof for cleansing, beautifying, promoting attractiveness, or altering the appearance”, without affecting structure or function .
Cosmeceuticals are now a reality due to the ever expanding dermatologic knowledge base, which has rendered obsolete the prior outdated clear distinction between cosmetics and drugs . It is somewhat bewildering to realize that water is a cosmeceutical. Water profoundly influences the structure and function of the viable epidermis. Many substances can function as cosmeceuticals if entry into and through the stratum corneum is facilitated via the use of penetration enhancers, such as propylene glycol, isopropyl myristate, or pyrrolidone derivatives. Propylene glycol profoundly alters the barrier characteristics of the stratum corneum, while isopropyl myristate is capable of penetrating into the lipid bilayer of cell membranes. Pyrrolidone derivatives interact with both keratin and stratum corneum lipids to drive substances into the skin. These enhancers are commonly found in cosmetic formulations; however, improved understanding of skin physiology allowed recognition of their profound effects on the skin, which were previously unknown.
Discussion
Skin Care Products
The three basic categories of skin care products are cleansers, moisturizers, and astringents. Cleansers are designed to remove sebum, desquamating corneocytes, bacteria, fungi and environmental dirt from the face and body, while leaving the intercellular lipid barrier intact. Astringents are actually a subset of cleansers designed to supplement the failure of the cleanser to perform its intended function. Moisturizers are designed to minimize the barrier damage induced by cleansing. Thus, these three skin care products work together to balance the hygiene needs of the skin with the important task of preserving barrier function.
Cleansers
The development of soaps designed to cleanse the skin has been the single most important advance in decreasing disease worldwide. Even though soap is ubiquitous in the developed world, one of the main goals of global health organizations is to introduce the concept of cleansing with soap to regions of the world where contagious diseases run rampant. In basic chemical terms, soap is a fatty acid salt resulting from a reaction between a fat and an alkali . The soap solubilizes sebum and environmental dirt, such that it can be rinsed away with water. The mechanics of rubbing the soap over the skin with the hand or a bathing implement results in the physical removal of desquamating scales, bacteria and fungi from the skin surface. In high-income countries, where bathing has become a daily ritual, excessive use of soap has resulted in dermatologic conditions such as xerotic eczema. This has led to the development of cleansers with skin conditioning benefits that are chemically not true soaps, and they are referred to as detergents.
Cleansers, whether formulated as bars or liquids, can be divided into three basic types: soaps, syndets and combars ( Table 153.1 ). True soaps are composed of long-chain fatty acid alkali salts with a pH of between 9 and 10. This alkaline pH raises the pH of the skin following cleansing, resulting in stratum corneum barrier disruption and the resultant feeling of tightness following bathing. Alkalinization of the skin disrupts the natural acid mantle, which may be significant in dermatitic skin. Recognition of the need to preserve skin pH at 5.4 led to the development of syn thetic det ergents, known as syndets, such as sodium cocoyl isethionate. Syndet cleansers, also known as beauty cleansers, contain less than 10% soap and are designed with a pH of 5.5–7.0 in order to minimize cutaneous alkalinization . The third type of cleanser, known as a combar, is composed of an alkaline soap to which surface active agents with a pH of 9–10 have been added. Combars are milder cleansers than true soaps, but induce more thorough cleansing than syndets. For example, true soap is a good cleansing choice for excessively oily or dirty skin, while a combar is a good cleanser for normal skin with a moderate amount of environmental dirt. Syndets would be the least damaging to the cutaneous barrier in persons with xerosis or any form of dermatitis.
| CATEGORIES OF CLEANSING PRODUCTS | ||
|---|---|---|
| Product type | Composition | Product examples ®, ™ |
| Bar soap | True soap in bar form; pH 9–10 | Ivory Bar Soap (Procter & Gamble) |
| Cashmere Bouquet (Colgate-Palmolive) | ||
| Syndet bar cleanser | Synthetic detergents (no soap), in bar form; pH 5.5–7 | Cetaphil Bar (Galderma) |
| Dove Bar (Unilever) | ||
| Olay Quench Moisturizing Bar (Procter & Gamble) | ||
| Syndet liquid | Synthetic detergents, in liquid form; pH 5.5–7 | Dove Liquid Soap (Unilever) |
| Olay Foaming Face Wash (Procter & Gamble) | ||
| Combar soap | Combination of true soap and synthetic detergent; pH 9–10 | Dial Bar Soap (Dial Corporation) |
| Irish Spring Bar Soap (Colgate-Palmolive) | ||
| Body wash | Emulsion system applied with a puff, allowing synthetic detergent cleansing combined with enhanced skin moisturization and emolliency | Aveeno Daily Moisturizing Body Wash (Johnson & Johnson) |
| Cetaphil Skin Restoring Body Wash (Galderma) | ||
| Dove Deep Moisture Body Wash (Unilever) | ||
| Olay Sensitive Body Wash (Procter & Gamble) | ||
| Lipid-free cleanser | Cleans without fats; may contain glycerin, cetyl alcohol, stearyl alcohol, sodium lauryl sulfate and, occasionally, propylene glycol | Aquanil Cleanser (Person & Covey) |
| CeraVe Cleanser (Valeant Consumer Products) | ||
| Cetaphil Gentle Skin Cleanser (Galderma) | ||
| Cleansing cream | Waxes and mineral oil with detergent action from borax | Noxzema Original Deep Cleansing Cream (Unilever) * |
| Pond’s Cold Cream * | ||
| Astringent/toner | Alcohol-based product that may contain witch hazel, salicylic acid or glycolic acid | Clarifying Lotion 2, 3, 4 (Clinique) |
| Moisturizing astringent/toner | Glycerin-based humectant moisturizer | Clarifying Lotion 1 (Clinique) |
| Exfoliant cleanser | Glycolic acid- or salicylic acid-containing cleanser | Oil-Free Acne Wash (Neutrogena) |
| Abrasive cleanser | Polyethylene beads or other small particles within the syndet cleanser | Clinique 7 Day Scrub Cream |
| Olay Age Defying Daily Renewal Skin Cleanser (Procter & Gamble) | ||
The many brands of cleansers currently on the market fall into one of the three aforementioned groups, yet there must be something unique, for marketing purposes, about each cleanser. The unique aspects of each cleanser are created through the addition of specialty additives ( Table 153.2 ). Common cleanser additives include various fragrances as well as foaming agents designed to alter the aesthetics of the lather, but the most dermatologically relevant additives are antibacterial agents. The most widely used antibacterial in both bar and liquid cleansers used to be triclosan , but is now benzalkonium chloride. Triclosan works by blocking lipid synthesis within the bacterial cell wall, thus decreasing the skin biofilm bacteria count and reducing odor. However, in 2016, triclosan was banned in the US as an ingredient in consumer antiseptic washes.
| SPECIALTY SOAP FORMULATIONS | |
|---|---|
| Type of soap | Unique ingredients |
| Superfatted soap | Increased oil and fat, representing up to 10% |
| Castile soap | Olive oil used as main fat |
| Deodorant soap | Antibacterial agents |
| French milled soap | Additives to reduce alkalinity |
| Floating soap | Extra air trapped during mixing process |
| Oatmeal soap | Ground oatmeal added (coarsely ground to produce abrasive soap; finely ground for gentle cleanser) |
| Acne soap | Sulfur, resorcinol, benzoyl peroxide and/or salicylic acid added |
| Facial soap | Smaller bar size, no special ingredients |
| Bath soap | Larger bar size, no special ingredients |
| Aloe vera soap | Aloe vera added to soap, no special skin benefit |
| Vitamin E soap | Vitamin E added, no special skin benefit |
| Cocoa butter soap | Cocoa butter used as major fat |
| Nut or fruit oil soap | Nut or fruit oils used as major fat |
| Transparent soap | Glycerin and sucrose added |
| Abrasive soap | Pumice, coarse oatmeal, maize meal, ground nut kernels, dried herbs or flowers added |
| High impact soap | Strong, high-concentration fragrance added to scent skin after cleansing |
| Soap-free soap | Contains synthetic detergents (syndet bar) |
Another important dermatologic need with regard to skin cleansing is minimization of skin barrier dysfunction. Unfortunately, surfactants cannot distinguish unwanted sebum and oil-soluble dirt from intercellular lipids. Thus, increases in transepidermal water loss are typically noted in direct proportion to the cleansing ability of the cleanser. An attempt to provide cleansing and barrier restoration in the same product has led to the development of body washes. Since body washes are liquids, incorporating both hydrophilic and lipophilic ingredients emulsified into a single phase, it is possible to cleanse and moisturize simultaneously while allowing for rinsing away of the surfactants. Body washes must be used with a puff to introduce both water and air into the cleanser emulsion in sufficient quantity to allow cleansing and moisturization to occur. The syndet detergents, primarily ammonium laureth sulfate, solubilize oil-soluble dirt into the rinse water for removal during the cleansing phase when the body wash concentration is high and the water concentration low, while occlusive moisturizing substances (e.g. petrolatum) and emollients (e.g. soybean oil) are left behind to retard transepidermal water loss and improve skin smoothness during the rinse phase when the body wash concentration is low and the water concentration is high.
Other cleanser variants for persons with dry, dermatitic skin include lipid-free, non-foaming cleansers and cold creams. These products are excellent at removing cosmetics and low levels of environmental dirt. Lipid-free cleansers are non-foaming, soap-free liquid products applied to dry or moistened skin, rubbed to produce minimal lather, and rinsed or wiped away. They possess low surfactant capabilities, and they can only remove bacteria through mechanical means, yet they are important in persons with barrier disruption . The classic cleanser for dry, dermatitic skin is cold cream, which combines the effect of a lipid solvent, such as wax or mineral oil, with detergent action from borax . However, not all formulations of cold creams contain borax.
Occasionally, a dermatologic need arises for specialty cleansers designed to offer a skin benefit beyond pure removal of sebum and environmental dirt. For example, it may be desirable to induce corneocyte disadhesion in older patients requiring an exfoliant cleanser. This can be accomplished through the addition of chemical exfoliants, such as salicylic acid or glycolic acid, to the cleanser formulations discussed previously. Exfoliant cleansers containing benzoyl peroxide or salicylic acid are sometimes used as an adjunct in topical acne treatment. Exfoliation can also be induced mechanically through the incorporation of fine abrasive particles (such as polyethylene beads, aluminum oxide, ground fruit pits, or sodium tetraborate decahydrate granules) in a liquid syndet cleanser to remove skin scale. Lastly, mechanical exfoliation can be encouraged through the use of specially woven face cloths, designed to remove skin scale without inducing epidermal damage.
The development of novel detergents and cleansing specialty additives has created a confusing plethora of consumer products, yet the goal remains the same: to allow adequate skin hygiene without barrier damage. Our next concern is the discussion of moisturizers, designed to replace skin sebum and natural moisturizing factors in instances where the stratum corneum barrier has been damaged from exuberant cleansing.
Moisturizers
The term “moisturizer” is somewhat misleading to the consumer, who assumes that the cream or lotion actually puts moisture or water back into the skin . Moisturizers do not put water back into the skin externally, nor do they get incorporated into the intracellular lipids. Moisturizers simply attempt to retard transepidermal water loss and create an optimal environment for restoration of the stratum corneum barrier . The optimal water content for the stratum corneum is between 10% and 30%, depending on the measurement technique employed, and moisturizers can function to raise the cutaneous water content through occlusion or humectancy via a variety of active agents ( Table 153.3 ) .
| DIFFERENT TYPES OF MOISTURIZERS | ||
|---|---|---|
| Moisturizer type | Composition | Product examples ®, ™ |
| Oil only | Petrolatum | Vaseline petroleum jelly (Unilever) |
| Oil-in-water emulsion | Water, petrolatum | Eucerin Cream (Biersdorf) |
| Polymer-based | Water, polyglycerylmethacrylate, petrolatum | Cetaphil Cream (Galderma) |
| Vegetable oil and wax | Castor oil, corn oil, ozokerite, beeswax, paraffin, carnauba wax | Lip Moisturizer (Neutrogena) |
| Glycerin-rich | Water, glycerin, petrolatum | Norwegian Formula Hand Cream (Neutrogena) |
| Curél Daily Moisture Original Lotion (Kao Brands Company) | ||
| Dimethicone and ceramides | Water, petrolatum, dimethicone, ceramides | CeraVe (Valeant) |
| EpiCeram (PuraCap Pharmaceutical) | ||
Occlusive moisturizers prevent evaporative water loss to the environment by placing an oily substance on the skin surface through which water cannot penetrate, thus replenishing the stratum corneum moisture by water movement from the lower viable epidermal and dermal layers . There are many different classes of chemicals that can function as occlusive moisturizers , for example, hydrocarbon oils and waxes (petrolatum, mineral oil, paraffin, squalene), silicones (cyclomethicone, dimethicone), vegetable oils (castor oil, corn oil, grape seed oil, soybean oil), animal oils (mink oil, emu oil), fatty acids (lanolin acid, stearic acid), fatty alcohols (lanolin alcohol, cetyl alcohol), polyhydric alcohols (propylene glycol), wax esters (lanolin, beeswax, stearyl stearate), vegetable waxes (carnauba wax, candelilla wax), phospholipids (lecithin), and sterols (cholesterol, ceramides) .
The most effective occlusive moisturizer is petrolatum, since it reduces transepidermal water loss by 99% . Total occlusion of the stratum corneum is undesirable, since transepidermal water loss is the cellular signal that initiates barrier repair and the resulting synthesis of intercellular lipids . Complete cessation of transepidermal water loss results in no barrier repair, allowing water loss to return to its pretreatment level once the complete occlusion has been removed . Petrolatum allows barrier repair while permeating throughout the interstices of the stratum corneum .
Another technique for rehydrating the stratum corneum is the use of humectants. Humectants are substances that attract moisture; they include glycerin, honey, sodium lactate, urea, propylene glycol, sorbitol, pyrrolidone carboxylic acid, gelatin, hyaluronic acid, and some vitamins and proteins . The body utilizes hyaluronic acid and other glycosaminoglycans in the dermis as biologic humectants to prevent desiccation of the skin. Humectants can only hydrate the skin from the environment when the ambient humidity exceeds 70%. Consequently, rehydration of the stratum corneum generally occurs by water that is attracted from the deeper epidermal and dermal tissues. Most moisturizers combine both occlusive and humectant moisturizing ingredients, since water drawn by a humectant to a damaged stratum corneum barrier will be lost to the atmosphere unless trapped by an occlusive . Humectants also help to improve the smoothness of xerotic skin by inducing corneocyte swelling and minimizing voids between the desquamating corneocytes .
In summary, remoisturization of the skin must occur in four steps:
- •
initiation of barrier repair (see Ch. 124 )
- •
alteration of surface cutaneous moisture partition coefficient
- •
onset of dermal–epidermal moisture diffusion
- •
synthesis of intercellular lipids .
Moisturizers attempt to increase stratum corneum water content through the principles of occlusion and humectancy. The discovery of aquaporin 3 channels in the skin and their modulation by glycerin and urea has increased research into osmotic cell balance as another mechanism for moisturization.
Astringents
Occasionally, patients use skin care products that either correct the deficiencies of the cleanser or supplement the effects of the moisturizer. These products are known as astringents or toners (see Table 153.1 ). They are used after cleansing but before moisturizing, and they are left on the face following use. Astringents are usually liquids wiped over the face with a cotton ball. Originally, astringents were intended to remove soap scum left behind on the face from the use of lye-based soaps and hard water. If left behind, this soap scum could cause irritant contact dermatitis. The original astringents were fragranced isopropyl alcohol or propylene glycol solutions designed to remove oil-soluble residue. The development of synthetic detergents and treated water has made this original intent obsolete, yet astringents remain popular.
Currently, astringents are used to remove the oily residue left behind after cleansing of the face with lipid-free cleansers or cleansing creams, discussed previously. Oily complexion astringents are formulated to remove any remaining sebum from the face following synthetic detergent cleansing or to deliver keratolytics, such as salicylic acid, glycolic acid or witch hazel. Some astringents designed for dry skin contain a humectant liquid moisturizer, such as propylene glycol or glycerin, and skin soothing agents, such as allantoin, guaiazulene or quaternium-19 . A complete cosmetic-counter facial treatment routine involves a cleanser followed by an astringent and then a moisturizer. Once the skin has been prepared in this manner, colored cosmetics are applied.
Colored Facial Cosmetics
Colored facial cosmetics are intended to adorn the eyes, lips and cheeks with color for the purposes of creating a fashionable appearance, highlighting certain desirable features, and camouflaging facial flaws. Colored cosmetics are of importance to the dermatologist for their role in maintaining skin health, inducing dermatitis, and camouflaging surgical defects.
Facial foundations
Formulation
Facial foundations are the first cosmetic applied to the face following the use of a moisturizer and are basically pigmented moisturizers worn for 8 hours or longer before removal. Consequently, this class of colored facial cosmetics has the greatest impact on the integrity of the skin. Facial foundations are available for every complexion type and skin color, fulfilling the needs listed in Table 153.4 .
| FUNCTIONS OF FACIAL FOUNDATION |
|
There are four basic facial foundation formulations: oil-based, water-based, oil-free, and water-free or anhydrous forms . Oil-based products are designed for dry skin, while water-based products can be adapted for all skin types. Oil-free formulations are used in oily skin foundations, while anhydrous forms are extremely long-wearing and used for camouflage or theatrical purposes.
Oil-based foundations are water-in-oil emulsions containing pigments suspended in oil (e.g. mineral oil) or lanolin alcohol. Vegetable oils (grape seed, coconut, sesame, safflower) and synthetic esters (isopropyl myristate, octyl palmitate, isopropyl palmitate) may also be incorporated. The water evaporates from the foundation following application, leaving the pigment in oil on the face. This creates a moist skin feeling, especially desirable in dry complected patients. Because the color is fully developed within the oily phase of the formulation, oil-based foundations do not shift color as they mix with sebum. These foundations are easy to apply, since the pigment can continue to be spread over the face for up to 5 minutes, prior to setting.
Water-based facial foundations are oil-in-water emulsions containing a small amount of oil, in which the pigment is emulsified, and a relatively large quantity of water. The primary emulsifier is usually a soap, such as triethanolamine, or a non-ionic surfactant. The secondary emulsifier, present in smaller quantity, is usually glyceryl stearate or propylene glycol stearate. These popular foundations are appropriate for minimally dry to normal skin. Since the pigment is already developed in oil, this foundation type is also not subject to color drift. The amount of time the product can be moved over the face, known in the industry as playtime, is shorter than with oil-based foundations.
Oil-free facial foundations contain no animal, vegetable or mineral oils. They contain other oily substances, such as dimethicone or cyclomethicone. These foundations are usually designed for oily complected individuals, since they leave the skin with a dry feeling. Dimethicone is non-comedogenic, non-acnegenic and hypoallergenic, accounting for the tremendous popularity of this type of facial foundation formulation. Both water-based and oil-free foundations are usually packaged in a bottle.
Water-free , or anhydrous, foundations are waterproof. Vegetable oil, mineral oil, lanolin alcohol and synthetic esters form the oil phase, which may be mixed with waxes to form a cream. High concentrations of pigment can be incorporated into the formulation, yielding an opaque facial foundation. The coloring agents are based on titanium dioxide with iron oxides, occasionally in combination with ultramarine blue. Titanium dioxide acts both as a facial concealing agent and sunscreen. These products can be dipped from a jar, squeezed from a tube, wiped from a compact, or stroked from a stick. Water-free foundations are well suited for use in people who require facial camouflaging. They can be combined with a high-coverage powder foundation to increase the opacity of the cosmetic.
Application and cutaneous effects
Facial foundations must be evenly applied to create the optimal cosmetic appearance and achieve the secondary benefit of sun protection. The iron oxide pigment and other covering agents, e.g. titanium dioxide, zinc oxide and kaolin, are physical particulates that block both UVA and UVB radiation (see Ch. 132 ). A facial foundation without any added organic sunscreen ingredients, such as ecamsule, octyl methoxycinnamate, oxybenzone or avobenzone, usually has a sun(burn) protection factor (SPF) of at least 4. Facial foundations that have greater coverage in order to camouflage underlying pigmentation defects usually possess an SPF of at least 8. The inclusion of additional sunscreen agents to the facial foundation can raise the SPF to 15. Thus, facial foundation is an excellent, cosmetically elegant facial photoprotectant.
An even, cosmetically acceptable application of facial foundation begins with a proper color match to the skin at the jawline and application with the fingertips. A dab of foundation should be placed on the forehead, nose, cheeks and chin, and blended with a light circular motion until it is evenly spread over the entire face, including the lips. Finally, a puff or sponge should be used, stroking in a downward direction, to remove any streaks and to flatten vellus facial hair. Special care should be taken to rub the foundation into the hairline, over the tragus, and beneath the chin. Foundation should also be blended around the eyes, and it may even be applied to the entire upper eyelid if desired. The foundation should be allowed to set or dry until it can no longer be removed with light touch. If additional coverage is desired, a second layer of foundation can be applied.
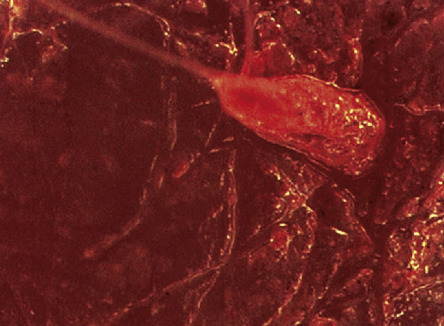
The most common adverse dermatologic effect related to the use of facial foundation is a condition patients describe as “breakouts”. Patients typically note small perifollicular papules 48 hours after using a new facial foundation. The appearance resembles that of acne; however, the 48-hour time course is inconsistent with a diagnosis of acne. This condition may represent a perifollicular irritant contact dermatitis, since facial foundations tend to migrate to the follicular ostia as they mix with eccrine secretions and sebum, which break down the cosmetic film ( Fig. 153.1 ). This observation may explain why facial foundations that have been found on clinical testing to be non-comedogenic and non-acnegenic cause acneiform eruptions in individuals with self-diagnosed sensitive skin. Overall, however, facial foundations are an infrequent cause of dermatologic problems.
Powders
One of the ways of preventing migration of facial foundation, improving its sun protective capabilities, and increasing oil absorption, is to apply powder over the foundation. Facial powders contain predominantly talc (hydrated magnesium silicate) and increased amounts of covering pigments. The covering pigments used in face powder are listed in order of increasing opaqueness in Table 153.5 . It is generally accepted that the optimum opacity is achieved with a particle size of 0.25 mcg. Black dermographism from earrings and rings can result when face powders contain ingredients, e.g. zinc oxide, that are harder than platinum, silver or gold.
| COVERING ABILITY OF FACE POWDER INGREDIENTS |
* Hardness greater than platinum, gold and silver so capable of producing black dermographism.
Facial powders usually also contain magnesium carbonate and/or kaolin (hydrated aluminum silicate) to absorb oil and perspiration. Full-coverage face powders with increased pigments and light-reflective particles are usually packaged as a cake in a compact and applied to the face with a puff, loose in a jar and dusted over the face with a brush, or stroked over the face from an automatic brush dispenser. These face powders with increased pigments can be used as a facial foundation and are known as mineral make-ups. They are recommended for persons with sensitive skin and rosacea as they contain no liquids, fewer preservatives, and fewer ingredients. As a result, there is decreased potential for allergic and irritant contact dermatitis. Specially pigmented powders are used to redden the cheeks, known as blushes, and to color the eyelids, known as eye shadows.
Facial blushes
Facial blushes are typically powders designed to simulate rosy cheeks, occasionally an unwanted finding in rosacea patients. Blushes have the same basic formulation as face powders, except for the presence of different surface characteristics that can vary from a matte dull finish, to a frosted shine, to a metallic glow, depending on current fashion trends . Some of the rough-edged particles designed to produce light reflection can cause irritation in people with sensitive skin. Powder blush can be used to absorb facial oil and blend the facial erythema of rosacea across the cheeks, as well as add color to a sallow face by dusting on the central chin, cheeks, nasal tip and forehead.
Eye shadows
Eye shadows are similar to powder blushes in formulation and surface characteristics, except that the color variation is broader, but limited in the US by the Food and Drug Administration (FDA) to the purified natural colors or inorganic pigments listed in Table 153.6 . Eye shadow can be used to camouflage misshapen eyes, provide sun protection to the upper eyelid, and minimize the appearance of unwanted periorbital pigmentation. Eye shadows are a common concern to dermatologists, since they may be responsible for eyelid dermatitis. They may contain the same light-reflective particles as blushes and cause pruritus of the eyelids due to irritant contact dermatitis until discontinued ( Fig. 153.2 ).
| PIGMENTS ALLOWED BY THE US FDA IN EYE SHADOW COSMETICS |
|

In one series, the North American Contact Dermatitis Group determined that 12% of cosmetic reactions occurred on the eyelid, but only 4% could be linked to eye make-up use . When allergic contact dermatitis is due to eye shadows, the most common culprits are the red pigments used in pinkish eye shadows. Unfortunately, it can be difficult to determine the etiology of allergic contact eyelid dermatitis with routine patch testing , since many substances can be transferred to the eye area by the hands, complicating the dermatologic evaluation . However, eye shadows are a rare cause of eye infections, since the dry powder cake does not support bacterial growth.
Mascaras
Mascaras are eyelash cosmetics, as opposed to eye shadows, which are eyelid cosmetics. Mascaras are designed to color, camouflage, elongate and thicken the eyelashes, which are the frame to the eyes. They must be carefully formulated to allow easy and even application without smudging, irritancy or toxicity. Some of the coloring agents employed include iron oxide to produce black, ultramarine blue to create navy, and umber, burnt sienna or synthetic brown oxide to create brown .
Most modern mascaras are formulated as liquids, then stored in a tube with a multitufted applicator brush or comb. The applicator is inserted into the tube between uses, providing numerous opportunities to inoculate bacteria into the cosmetic. The most dangerous bacterial infection is a corneal infection due to Pseudomonas aeruginosa , which can permanently diminish visual acuity . Staphylococcus epidermidis, S. aureus and fungal organisms may also proliferate in contaminated mascaras . Infections are more common if the globe is traumatized by the infected mascara wand. Even though mascaras contain antibacterials, it is still wise to discard all mascara tubes after three months and not allow multiple persons to use the same mascara tube .
There are several mascara formulations that are less likely to support bacterial and fungal growth ( Table 153.7 ). Mascaras are available as water- or solvent-based and as a water/solvent hybrid. Water-based mascaras are easily removed with water and less likely to cause eye area irritation, but the presence of water provides a welcome medium for bacterial growth. Solvent-based mascaras are manufactured without water, must be removed with a special cleanser, and are more irritating; however, they are less likely to support bacterial growth and are therefore the formulation of choice for individuals who are carriers of Staphylococcus or Streptococcus spp . The water/solvent hybrid mascaras are an attempt to provide a water-resistant cosmetic with the benefits of both.
| DIFFERENT TYPES OF MASCARA FORMULATIONS | ||
|---|---|---|
| Mascara formulation | Composition | Advantages/Disadvantages |
| Water-based | Waxes, pigments, resins | Easy to remove with water; runs with tearing; supports bacterial growth |
| Solvent-based waterproof | Petroleum distillates, pigments, waxes | Must be removed with solvent; waterproof; does not support bacterial growth |
| Water-resistant water/solvent hybrid | Oil-in-water emulsion, pigments | Removal with water and cleanser; resists running with tearing; less likely to support bacterial growth |
| Compressed cake | Pigments, talc | Removal with water; runs with tearing; least allergenic; does not support bacterial growth |
Another dermatologic side effect of the use of mascara is conjunctival pigmentation, resulting from the washing of mascara into the conjunctival sac by lacrimal fluid . This colored particulate matter can be observed on the upper margin of the tarsal conjunctiva. Histologically, the pigment is seen within macrophages and extracellularly in association with a variable lymphocytic infiltrate. Electron microscopy suggests that ferritin, carbon, and iron oxides are present within the tissues . Unfortunately, there is no treatment for the condition, which is usually asymptomatic.
Specialty mascaras are available for curling and elongating the eyelashes. These mascaras contain pigmented polymers that polymerize on the eyelash as they dry. The polymer then shrinks, curling the eyelash and placing a thin, long-wearing, pigmented film around the hair which thickens and elongates the lash. In addition, a prescription cosmeceutical containing bimatoprost 0.03% (Latisse ® ; originally indicated for the treatment of glaucoma) is available to elongate eyelashes via prostaglandin modulation (see Ch. 129 ) . Side effects include iris and eyelid pigmentation, which may be permanent.
Lipsticks
Lipstick is a lip cosmetic designed to frame the teeth. Traditional lipsticks are mixtures of waxes, oils and pigments in various concentrations to yield the characteristics of the final product. For example, a lipstick designed to remain on the lips for a prolonged period of time is composed of high wax, low oil and high pigment concentrations, whereas a product designed for a smooth creamy feel on the lips is composed of low wax and high oil concentrations . The waxes commonly incorporated into lipstick formulations are white beeswax, candelilla wax, carnauba wax, ozokerite wax, lanolin wax, ceresin wax and other synthetic waxes. Usually, lipsticks contain a combination of these waxes carefully selected and blended to achieve the desired melting point. Oils for pigment dispersion are then selected, such as castor oil, white mineral oil, lanolin oil, hydrogenated vegetable oils or oleyl alcohol, to form a film suitable for application to the lips .
Newer lipstick formulations contain long-wearing polymers that create a waterproof film over the lips that remains in place indefinitely until worn away with speech or eating. These long-wearing lip products can cause cheilitis, due to their non-moisturizing formulations. In addition, lip products are marketed that claim to plump the lips. These products contain irritants, such as capsaicin, that create a mild irritant contact dermatitis resulting in short-lived lip edema.
Certain common lipstick ingredients can cause problems in the sensitized patient . Castor oil, found in almost all lipsticks due to its excellent ability to dissolve bromo acid dyes, can cause allergic contact dermatitis . Even the bromo acid dyes, such as eosin (D & C Red No. 21), found in indelible lipsticks can cause allergic contact dermatitis . Other lipstick ingredients reported to cause allergic contact dermatitis include: waxes (e.g. propolis ), preservatives (e.g. propyl gallate , benzoic acid ), sunscreens (e.g. oxybenzone , benzophenone-3 ), colors (e.g. lithol rubine BCA [Pigment Red 57-1] ), fragrances (e.g. peppermint oil), vitamin E, and ricinoleic acid .
Facial cosmetics for camouflaging
All of the colored cosmetics previously discussed are used in combination for facial camouflaging purposes in order to minimize facial defects while accentuating attractive facial features. Camouflage cosmetics are used by paramedical aestheticians, dermatologists, plastic surgeons, and cosmetic consultants . Their successful use requires a well-formulated, quality product applied with the skill of a stage make-up technician and the artistic abilities of a painter . Facial defects requiring camouflaging are defects of pigmentation and/or contour .
Pigmentation defects represent abnormalities limited to the color of the skin, whereas contour defects are defined as areas where the facial skin is hypertrophic or atrophic, with textural changes due to the absence of appendageal structures. Table 153.8 lists examples of pigmentary abnormalities frequently encountered by dermatologists that arise from inflammatory disorders, systemic diseases, or extrinsic effects (e.g. sun exposure). Pigmentation defects or discolorations can be camouflaged either by applying an opaque cosmetic that allows none of the abnormal underlying skin tones to be appreciated or by applying foundations of complementary colors. For example, red discoloration can be camouflaged by applying a green foundation, since green is the complementary color to red. The blending of the red skin with the green foundation yields a brown tone, which can be readily covered by a more conventional facial foundation. Furthermore, yellow skin tones can be blended with a complementary-colored purple foundation to also yield brown tones.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


