Key points
- •
Blepharoptosis, or ptosis, refers to the abnormally low position of the upper eyelid in primary gaze.
- •
Ptosis of the eyelid is usually secondary to involutional changes, or is congenital in nature, although a broader classification scheme has been developed ( Box 3.1 ).
Box 3.1
Classification of ptosis by etiology
Congenital ptosis
Myogenic
Neurologic
- •
Horner syndrome
- •
Cranial nerve III palsy
- •
Marcus Gunn jaw-winking syndrome
Syndromic
- •
Blepharophimosis syndrome
- •
Others
Acquired ptosis
Aponeurotic or involutional
- •
Attenuation, post-surgical, allergy, contact lens wear
Myogenic
- •
Myasthenia gravis
- •
Chronic progressive external ophthalmoplegia
- •
Myotonic dystrophy
Neurogenic
- •
Horner syndrome
- •
Cranial nerve III palsy
Mechanical
- •
Traumatic
- •
Pseudoptosis
- •
- •
Presenting symptoms range from cosmetic asymmetry to visual field loss.
- •
Identification of the underlying etiology and proper pre-operative measurements of margin reflex distance (MRD) and levator function (LF) are crucial for successful surgical repair.
- •
The modified Fasanella–Servat procedure offers an excellent, and adjustable, option for correction of mild-moderate ptosis and works well in combination with other aesthetic procedures.
Patient selection
Blepharoptosis of the upper eyelid is a common condition. It is classified by its etiology as congenital, involutional, neurogenic, myogenic and mechanical. The vast majority of cases are either congenital or involutional. In the aesthetic setting, even more are involutional and are seen in conjunction with dermatochalasis and/or brow ptosis. For this reason, appropriate diagnosis of upper eyelid ptosis is critical to achieving a successful result.
Patients may complain of eyelid height or crease asymmetry, and/or a gradual decrease in the size of the palpebral aperture. Visual symptoms include superior visual field loss and central loss of vision in severe cases. Patients should be questioned about the onset of the ptosis, a history of trauma, prior surgery or botulinum toxin injection, fluctuation in the eyelid height, diplopia and any associated systemic manifestations. Old photographs are useful in determining the onset and degree of prior ptosis. When surgical repair is considered, patients should be questioned about other ocular diseases, and in particular dry eyes.
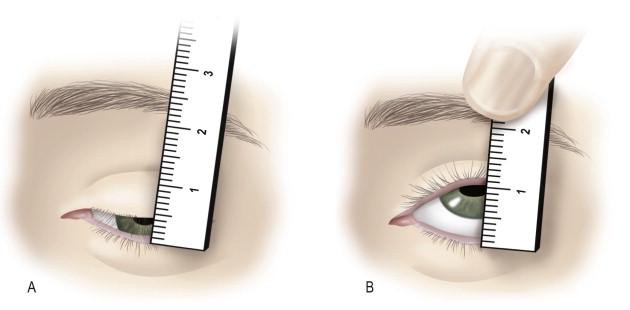
The physical examination can usually determine the etiology and guides surgical planning. The most useful clinical measurements are margin reflex distance (MRD), palpebral fissure width (PF), levator function (LF), and lid crease height (LC). Measurements are made in primary gaze with the brow relaxed or negated with the examiner’s hand. The MRD is measured from the central corneal light reflex (usually the center of the pupil) to the upper eyelid margin and is normally 3–4 mm. The PF is measured from the lower to upper eyelid margin in the mid-pupillary axis and is usually 8–10 mm. The LF is assessed by measuring the upper eyelid excursion from extreme downgaze to extreme upgaze while the brow is neutralized ( Figure 3.1 ). This measurement is critical to determining if an eyelid procedure can be utilized to correct ptosis. A normal measurement is 14–16 mm and values less than 5 mm generally require frontalis fixation for ptosis correction. The shape and height of the upper eyelid crease is noted. In aponeurotic or involutional types of ptosis, the eyelid crease is elevated and a deep superior sulcus may be seen. Pupillary examination focuses on asymmetry and reactivity in light and dark to rule out Horner syndrome, which may be associated with mild upper eyelid ptosis. Humphrey visual field testing can be performed to demonstrate a superior visual field defect that improves with taping of the upper eyelid.
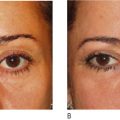
The vast majority of patients, particularly aesthetic consultations, will present with involutional ptosis. In this case, patients will notice a gradual decrease in the upper eyelid height. Aponeurotic ptosis may be associated with contact lens use, prior eye or periocular surgery, eye rubbing and chronic ocular allergy. The examination will show a decreased MRD, elevated eyelid crease and/or a deep superior sulcus with normal levator function. Often, patients will demonstrate chronic frontalis use to compensate for upper eyelid ptosis. This may present as an elevated brow on the side with eyelid ptosis. It is important to identify this, as masking of aponeurotic ptosis can result in suboptimal post-operative results in cosmetic eyelid surgery ( Figure 3.2 ). In asymmetric cases, Hering’s law of central and equal innervation to the levator muscles may cause the less ptotic or normal eyelid to appear retracted ( Figure 3.3 ).


Indications
Patients with classic aponeurotic ptosis are candidates for surgical correction if they are bothered by the change in eyelid aesthetics or if there is functional visual loss associated with the ptosis. Those patients with a history of dry eye disease, prior laser in-situ keratomileusis (LASIK) or a poor Bell’s phenomenon should consider the increased risk of post-operative ocular sicca symptoms and keratopathy. If proceeding with surgery, the surgeon should err on the side of undercorrection in these individuals.
Operative technique
Many operative techniques have been described for the correction of involutional ptosis associated with moderate or good levator function. These include levator reinsertion, muellerectomy and the Fasanella–Servat procedure. Herein we describe our experience with a modified Fasanella–Servat procedure for the correction of mild–moderate ptosis in a predominantly aesthetic patient population. We prefer this method since it does not require intraoperative patient participation, allowing for general anesthesia in cases that are combined with additional plastic surgical procedures. Additionally, as described later, the procedure offers the opportunity to post-operatively adjust the eyelid contour and height in the office without the need for anesthesia.
Pre-operative preparation
The incision site is marked in the holding area with the patient in the seated or semi-reclined position. The upper eyelid crease is marked, as is any proposed skin resection, similar to a standard upper eyelid blepharoplasty. Of note, even in cases where there seems to be little dermatochalasis, one can expect a small amount of additional skin presenting itself once the eyelid is elevated and the chronic brow use is diminished by ptosis correction. We almost always remove some skin with this technique.
The patient is placed in the supine position and either monitored sedation or general anesthesia is used. If the procedure is confined to the eyelids, typically sedation is chosen. Tetracaine ophthalmic drops are given to each eye. Lacri-Lube® ointment is placed within protective corneal shields and these are placed over both eyes. Local infiltration of the upper eyelid is achieved with 2% lidocaine with 1 : 100 000 epinephrine.
Technique
A #15 blade is used to incise the skin in the previously made blepharoplasty mark. Skin and orbicularis oculi muscle are removed with curved Steven scissors. Hemostasis is obtained with unipolar cautery and pledgets soaked in epinephrine. The orbital septum is incised along the extent of the incision. Any excess central or medial fat is judiciously resected with the Colorado needle tip. The orbicularis muscle is contoured with the same device.
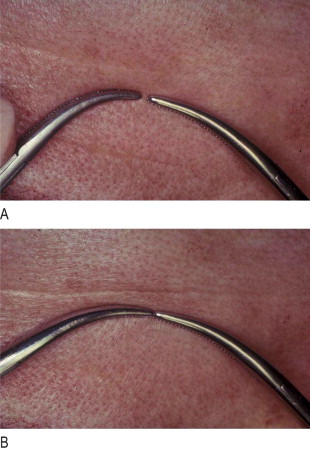
Two symmetrically sized and shaped curved hemostat clamps are chosen for the tarsoconjunctival resection ( Figure 3.4 ). These will ultimately create the eyelid contour and should be selected carefully. The upper eyelid is everted ( Figure 3.5 ) and a small (2 mm), medium (4 mm) or large (6 mm) tarsoconjunctival resection is delineated with the clamps. We anticipate achieving 1 mm of lift for a small resection, 2 mm for a medium and 3 mm for a large ( Box 3.2 ). It is imperative to leave at least 4 mm of residual tarsus and conjunctiva on the upper eyelid to avoid lid destabilization and potential entropion. The clamps are placed such that the largest resection occurs over the medial aspect of the pupil in primary gaze ( Figure 3.6 ). In older patients, a lateral shift of the tarsus occurs with aging, but the clamps should be placed such that the peak of the upper eyelid will be in the mid-pupillary axis, not at the region of greatest tarsal vertical length. A 5-0 nylon suture on a P-3 needle is loaded backhand and passed from inside the upper eyelid wound centrally and directed to exit at the posterior aspect of the clamps medially ( Figure 3.7 ). The suture is passed in a running, buried fashion, just posterior to the clamps, from medial to lateral ( Figure 3.8 ). It is important that each suture pass begins in the previous suture hole, thereby burying the suture. If exposure of the suture occurs, the patient will experience foreign body sensation and may develop a corneal abrasion or ulcer.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


