Correction of Lateral Orbital Wall Fractures
Parit A. Patel
DEFINITION
Of the seven bones that make up the orbit, the lateral orbit is composed mainly of the zygomatic bone.
Fractures of the lateral orbit can result in expansion of the orbital volume with subsequent enophthalmos and orbital dystopia.
Open reduction and internal fixation of the orbit restore the anatomy of the orbit and orbital volume. To restore the orbital volume successfully, the surgeon must have comprehensive understanding of the intricate anatomy of the orbit and surgical approaches to the orbit.
ANATOMY
The orbit is a cone-shaped structure with a fixed volume.
The seven bones that compromise the orbit include the sphenoid, maxilla, zygoma, frontal, ethmoid, lacrimal, and palatine.
The contents of the orbit include the globe, extraocular muscles, cranial nerves II to VI, ophthalmic artery and other minor vessels, orbital fat, orbital septum, medial and lateral canthal tendons, check and suspensory ligaments, ciliary ganglion, lacrimal gland and sac, and nasolacrimal duct.
The optic canal contains the optic nerve and ophthalmic artery. The superior orbital fissure contains cranial nerves III, IV, and VI. The inferior orbital fissure contains the infraorbital artery and vein and branches of the maxillary nerve.
Orbital volume in the adult patient has been demonstrated to be 21.31 ± 2.50 cm3.1
Fractures of the lateral orbital wall can cause orbital volume expansion. Fractures greater than 2.0 cm2 can result in orbital expansion and clinically relevant enophthalmos.
Fractures of the lateral orbital wall occur at the zygomatic sphenoid (ZS) suture, the greater wing of the sphenoid or the zygoma. The zygomatic portion of the orbit is the thickest bone of the orbit.
Indications for treatment include clinically relevant expansion of the orbital volume with resulting enophthalmos and diplopia. Patients can also have blow-in fractures of the lateral orbit with associated proptosis.
The lacrimal apparatus is important for tear production and drainage.
The lacrimal apparatus consists of the lacrimal gland, which is located in the superolateral aspect of the orbit and produces tears.
The lacrimal canaliculi, lacrimal sac, and nasolacrimal duct are important structures for draining tears into the nose (FIG 1).
PATHOGENESIS
Lateral orbital fractures occur from significant force to the craniofacial skeleton due to trauma.
Impure fractures involve a fracture within both the orbit and the orbital rim.
Pure orbital fractures involve isolated fractures within the orbit.
The incidence of pure lateral orbital fractures is low, approximately 1% of all orbital fractures.2
Lateral orbital fractures most commonly occur at the ZS suture and can be associated with zygomatic maxillary complex (ZMC) fractures.
Fractures of the orbit can result in expansion of the orbital volume resulting in enophthalmos.
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient usually presents with a history of significant facial trauma.
Associated signs and symptoms include periorbital pain, swelling, ecchymosis, dysesthesia, diplopia, and/or enophthalmos.
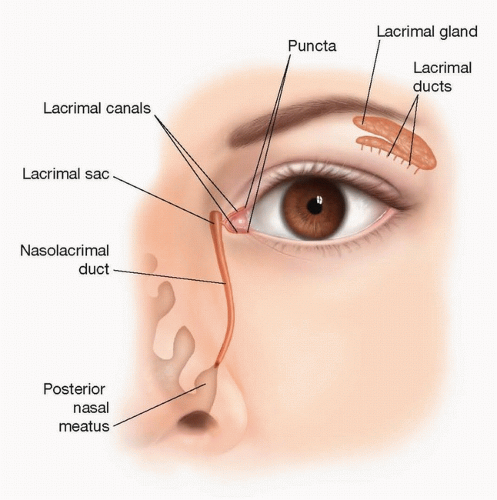
FIG 1 • Lacrimal apparatus.
The patient can also have associated facial fractures that can be identified on physical examination with bony stepoffs, gross facial asymmetries, and malocclusion.
Enophthalmos can be identified using a Hertel exophthalmometer.
For every 1-cm3 volumetric increase in the orbital volume, enophthalmos increases by an increment of 0.89 mm.3
It can be difficult to assess enophthalmos in the acute setting because of periorbital swelling.
The treating surgeon should be aware of surgical emergencies related to trauma to the orbit such as globe rupture, hyphema, entrapment, or a retrobulbar hematoma. In the setting of entrapment, there is restriction of movement of the globe.
The clinical findings of a retrobulbar hematoma include severe ocular pain, visual acuity disturbance, and proptosis.
There should be a low threshold for involving ophthalmology in situations of significant trauma to the periorbital region.
Traumatic superior orbital fissure syndrome, although rare, can occur with lateral orbital wall fractures and is associated with ophthalmoplegia, proptosis, eyelid ptosis, a fixed and dilated pupil, and anesthesia in the ipsilateral ophthalmic branch of the trigeminal nerve. Orbital apex syndrome has a similar presentation; however, the patient additionally has visual loss from optic nerve injury.
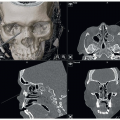
IMAGING
A CT scan of the face confirms clinical findings associated with facial fractures.
The axial images will demonstrate the fracture of the lateral orbital wall and other related fractures, such as a ZMC fracture.
The coronal images will demonstrate the size of the defect, which can be measured to assist in determining the indications for surgery.
Sagittal images can help determine the posterior extent of the fracture and assist in sizing the implant or graft.
NONOPERATIVE MANAGEMENT
If the fracture is less than 2.0 cm2 and there are no signs of acute enophthalmos, the patient can be managed nonoperatively and monitored closely for development of enophthalmos and/or diplopia. There is approximately a 4- to 6-week window to treat the patient before the diplopia may require surgical correction.
If the orbital fracture defect is marginal, the patient can be monitored until the swelling subsides to evaluate for enophthalmos.
After resolution of swelling, if the patient has no signs or symptoms of enophthalmos or diplopia, surgery is not required.
If there is a nondisplaced fracture of the zygomatic portion of the lateral orbital wall or at the ZS suture, the patient can be managed nonoperatively.
Isolated fractures of the greater wing of the sphenoid, even with mild displacement, can be managed nonoperatively.
SURGICAL MANAGEMENT
If the patient is stable, it is ideal to repair the orbital fracture in the first 24 to 48 hours.
Beyond that time, there is maximal swelling that makes the operation and surgical approach more difficult.
If the fracture is of marginal size and the patient does not have evidence of clinically relevant enophthalmos, the surgeon can wait 2 weeks to monitor and determine if surgery is indicated.
The objective of surgical intervention is to restore the anatomy of the orbit and the premorbid orbital volume. This prevents development of facial asymmetries related to enophthalmos or orbital dystopia. Furthermore, operative repair reduces the risk of developing strabismus and diplopia in the subacute phase or long term.
Operative repair involves a surgical approach to the orbit through either a transconjunctival approach or a transcutaneous approach (ie, subciliary or midlid incision). Once in a subperiosteal plane, the periorbita is dissected free from the underlying bony orbit.
Fractures of the lateral orbital wall occur most commonly at the ZS suture. The fracture can be comminuted and have an associated defect or be a linear fracture at the ZS suture or through the zygomatic bone.
Depending on the extent of the fracture, the fracture can be repaired without bony fixation or with a titanium plate. If a sizeable defect is present, the lateral orbit can be reconstructed with an alloplastic orbital implant, mesh plate, or bone graft. If the fracture of the lateral orbit is associated with a ZMC fracture, the fracture at the ZS suture can be used to verify the reduction of the ZMC segment, with or without plate fixation.
After open reduction and internal fixation, the lower lid is reconstructed appropriately to minimize the risk of ectropion, entropion, or lower lid malposition.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree