Upper eyelid ptosis and crease abnormalities can lead to significant cosmetic deformity. An intimate knowledge of the anatomic structures responsible for eyelid height, contour, and pretarsal show will allow precise surgical correction.
Key points
- •
Involutional changes with levator aponeurotic dehiscence is the most common cause of blepharoptosis, which presents with low margin-to-reflex distance, elevated eyelid crease, and normal levator function.
- •
Pretarsal platform is a complex anatomic structure defined by the anatomic eyelid crease and preseptal skin, fat, and brow positions.
- •
Precise surgical levator advancement can lead to appropriate marginal contour, symmetric height and allows exact eyelid crease management.
- •
Muller muscle conjunctiva resection is an effective, precise surgical procedure that requires no intraoperative patient interaction for improvement of ptosis and eyelid crease asymmetry.
- •
Eyelid crease creation and symmetry improvement can be achieved with or without ptosis repair and involves deep fixation of pretarsal anterior lamellae to the levator aponeurosis.
Introduction
The complex anatomy of the upper eyelid is not only responsible for the upper eyelid position superior to the visual axis, but also contributes to the aesthetically pleasing lines of the eyelid margin and eyelid crease, and their relationship to the brow. The function of the upper eyelid is ocular protection and tear dispersion over the eye. Upper eyelid retractors, which are responsible for upper eyelid height and excursion, include the levator muscle and its aponeurosis, Muller muscle, and limited functions from the frontalis muscle ( Fig. 1 ). The levator muscle, which is primarily responsible for upper eyelid height and excursion, is innervated by the oculomotor nerve after its origination on the sphenoid bone in the posterior orbit. The skeletal muscle of the levator palpebrae superioris transitions into an aponeurosis after passing through the Whitnall check ligament in the superior orbit. Traditionally, the upper eyelid crease is thought to derive from the insertion of the levator aponeurosis fibers into the anterior lamellae of the eyelid. Muller muscle is an involuntary, sympathetically innervated, smooth muscle, which originates on the undersurface of the levator muscle and inserts at the superior edge of tarsus. The peripheral arcade of eyelid is an excellent landmark as it sits just above the tarsus, sandwiched between the levator aponeurosis and Muller muscle. The orbicularis muscle is a sphincter within the anterior lamellae and is responsible for eyelid protraction.
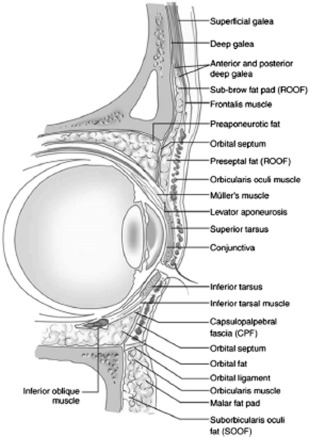
The ideal upper eyelid exhibits a gentle curve with acute medial angle, peaks as it extends laterally beyond the pupil, and gently tapers as it extends temporally. Centrally, the upper eyelid margin commonly falls just below the superior limbus but still well above the central visual axis. The healthy upper eyelid is full without significant fat protrusion. The complex relationship of the upper eyelid not only involves the height of the margin in relation to the visual axis, but also the stature of the pretarsal platform. Classically in most anatomic textbooks, the insertion of fibers from the levator aponeurosis into the orbicularis muscle and skin are responsible for the formation and maintenance of the eyelid crease. Functionally, the upper eyelid crease is formed at the “buckle point” of the upper eyelid skin where the nonfixated preseptal and orbital skin meets the well-fixated pretarsal anterior lamellae. Because of differences in the amount of excess eyelid skin and fat, in addition to brow architecture, the anatomic upper eyelid crease does not always correspond with the height of the pretarsal platform. Eyelid creases and secondarily the pretarsal platform can take on multiple shapes, including tapered, semilunar, and parallel. Compensatory brow elevation is commonly noted in patients with acquired blepharoptosis and can be noted not only as brow asymmetry but also frontalis muscle stimulation on the elevated side. Frequently, the brow will achieve normal height following repair of blepharoptosis. Symmetry is the key to the cosmetically appealing upper eyelid. Not only is the upper eyelid height evenness crucial, but the shape, pretarsal platform height, eyelid crease curvature, and brow position are all equally important in aesthetic eyelid evaluation.
Blepharoptosis of the upper eyelid is diagnosed when the upper eyelid margin to corneal light reflex distance (MRD) is abnormally low and can occur in one eye or both eyes. Ptosis is commonly secondary to senile involution, but in some cases can have secondary myogenic, neurogenic, or mechanical causes. Dehiscence of the levator aponeurosis causing ptosis can occur as an age-related involutional change, but is more prevalent in contact lens wearers and patients who have undergone ocular surgery. Measurement of eyelid elevator function remains one of the best differentiating factors for ptosis etiologies. Unlike other etiologies, levator function is normal in patients with involutional ptosis despite levator aponeurotic disinsertion.
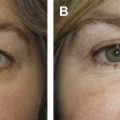
Eyelid crease asymmetry is commonly associated with blepharoptosis but can have other congenital, anatomic, or ethnic etiologies. Commonly with levator dehiscence, the pretarsal platform will expand secondary to elevation of the eyelid crease ( Fig. 2 ). Despite normal MRD, congenital and anatomic eyelid crease asymmetries are common and may require surgical correction. Aesthetically, symmetry of eyelid MRD and contour are important; however, height of pretarsal platform may be more important for some patients.

Introduction
The complex anatomy of the upper eyelid is not only responsible for the upper eyelid position superior to the visual axis, but also contributes to the aesthetically pleasing lines of the eyelid margin and eyelid crease, and their relationship to the brow. The function of the upper eyelid is ocular protection and tear dispersion over the eye. Upper eyelid retractors, which are responsible for upper eyelid height and excursion, include the levator muscle and its aponeurosis, Muller muscle, and limited functions from the frontalis muscle ( Fig. 1 ). The levator muscle, which is primarily responsible for upper eyelid height and excursion, is innervated by the oculomotor nerve after its origination on the sphenoid bone in the posterior orbit. The skeletal muscle of the levator palpebrae superioris transitions into an aponeurosis after passing through the Whitnall check ligament in the superior orbit. Traditionally, the upper eyelid crease is thought to derive from the insertion of the levator aponeurosis fibers into the anterior lamellae of the eyelid. Muller muscle is an involuntary, sympathetically innervated, smooth muscle, which originates on the undersurface of the levator muscle and inserts at the superior edge of tarsus. The peripheral arcade of eyelid is an excellent landmark as it sits just above the tarsus, sandwiched between the levator aponeurosis and Muller muscle. The orbicularis muscle is a sphincter within the anterior lamellae and is responsible for eyelid protraction.
The ideal upper eyelid exhibits a gentle curve with acute medial angle, peaks as it extends laterally beyond the pupil, and gently tapers as it extends temporally. Centrally, the upper eyelid margin commonly falls just below the superior limbus but still well above the central visual axis. The healthy upper eyelid is full without significant fat protrusion. The complex relationship of the upper eyelid not only involves the height of the margin in relation to the visual axis, but also the stature of the pretarsal platform. Classically in most anatomic textbooks, the insertion of fibers from the levator aponeurosis into the orbicularis muscle and skin are responsible for the formation and maintenance of the eyelid crease. Functionally, the upper eyelid crease is formed at the “buckle point” of the upper eyelid skin where the nonfixated preseptal and orbital skin meets the well-fixated pretarsal anterior lamellae. Because of differences in the amount of excess eyelid skin and fat, in addition to brow architecture, the anatomic upper eyelid crease does not always correspond with the height of the pretarsal platform. Eyelid creases and secondarily the pretarsal platform can take on multiple shapes, including tapered, semilunar, and parallel. Compensatory brow elevation is commonly noted in patients with acquired blepharoptosis and can be noted not only as brow asymmetry but also frontalis muscle stimulation on the elevated side. Frequently, the brow will achieve normal height following repair of blepharoptosis. Symmetry is the key to the cosmetically appealing upper eyelid. Not only is the upper eyelid height evenness crucial, but the shape, pretarsal platform height, eyelid crease curvature, and brow position are all equally important in aesthetic eyelid evaluation.
Blepharoptosis of the upper eyelid is diagnosed when the upper eyelid margin to corneal light reflex distance (MRD) is abnormally low and can occur in one eye or both eyes. Ptosis is commonly secondary to senile involution, but in some cases can have secondary myogenic, neurogenic, or mechanical causes. Dehiscence of the levator aponeurosis causing ptosis can occur as an age-related involutional change, but is more prevalent in contact lens wearers and patients who have undergone ocular surgery. Measurement of eyelid elevator function remains one of the best differentiating factors for ptosis etiologies. Unlike other etiologies, levator function is normal in patients with involutional ptosis despite levator aponeurotic disinsertion.
Eyelid crease asymmetry is commonly associated with blepharoptosis but can have other congenital, anatomic, or ethnic etiologies. Commonly with levator dehiscence, the pretarsal platform will expand secondary to elevation of the eyelid crease ( Fig. 2 ). Despite normal MRD, congenital and anatomic eyelid crease asymmetries are common and may require surgical correction. Aesthetically, symmetry of eyelid MRD and contour are important; however, height of pretarsal platform may be more important for some patients.
Preoperative planning and preparation
Ptosis repair can be desired for several different reasons, including visual obstruction, heavy sensation, contact lens fitting, and cosmetic improvement. Ideal results of surgery depend on appropriate surgical candidate selection, preoperative planning, and surgical technique. Consideration of patient concerns, etiology of complaints, anatomic findings, systemic or ocular comorbidities, and goals of surgery should be intertwined to develop a surgical plan. A clear understanding of patients’ concerns will allow the surgeon to evaluate the likelihood of achieving the desired goals. Patients may complain of visual obstruction, eyelid heaviness, or even droopy eyelid, which may relate to a low MRD, excessive eyelid skin, or even pretarsal platform asymmetry. A mutual understanding should be achieved between the patient and surgeon with a clear expectation of anticipated surgical outcomes. If possible, poor surgical candidates, those with unrealistic expectations, and patients with worrisome secondary diagnoses inducing ptosis should be avoided.
One goal of evaluating patients with upper eyelid ptosis is to exclude secondary worrisome causes that may affect patient health or surgical candidacy. Besides an in-depth evaluation of the patient’s complaints and systemic assessment, several ophthalmic findings should be appraised, including MRD, levator excursion, skin crease, eyelid height variability, orbicularis strength, and Bell phenomenon. The MRD is best measured in primary gaze with a millimeter ruler and a dim flashlight. Fixation of the patient’s gaze onto the light allows the most accurate assessment. Levator excursion is the most clinically useful assessment as to the health of the levator, and the measurement is taken for the amount of movement of the eyelid margin from extreme downgaze to extreme upgaze. Isolation of the eyelid with brow immobilization and avoiding head movement will provide the best assessment. Normal excursion ranges from 12 to 18 mm. Suspicion of a secondary cause for ptosis should be considered if levator movement is less than 12 mm or significantly different between eyes ( Fig. 3 ).