Key points
- •
Blepharoplasty remains one of the most common aesthetic procedures, and knowledge of the potential complications and treatment based upon a post-operative timeframe is essential.
- •
Retrobulbar hemorrhage is rare, but can lead to blindness. It typically occurs in the first week post-operatively, but is most common within the first 24 hours after surgery.
- •
Corneal irritation is common and can occur throughout the post-operative period. Early on, this may signify an abrasion. Patients should be examined at a slit lamp and can be treated with artificial tears and/or antibiotic drops/ointment based upon the diagnosis.
- •
Eyelid malposition (ptosis, lagophthalmos, ectropion or entropion) may be noted early post-operatively, but is usually managed expectantly, unless it persists for months after surgery or threatens the health of the eyeball.
- •
Blepharoplasty is often performed concurrently with other periocular procedures in an attempt to achieve a more comprehensive aesthetic result. These procedures have their own set of complications.
Introduction
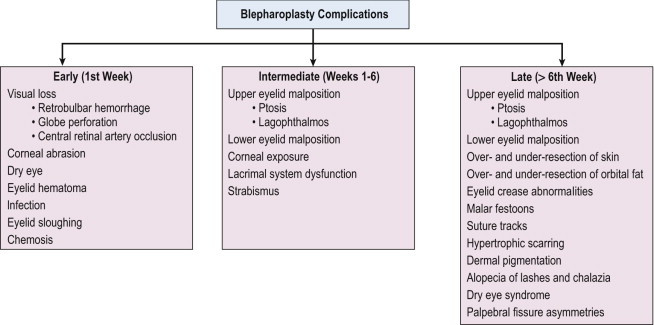
Blepharoplasty remains one of the most common aesthetic procedures performed. This chapter addresses the potential complications of blepharoplasty and offers a comprehensive approach to their recognition and treatment. The chapter is arranged based upon the typical post-operative timeframe when these are encountered. The following outline ( Figure 14.1 ) provides an overview of the most common and concerning complications.
Complications in the early post-operative period (week 1)
Visual loss
The most feared complication of blepharoplasty is permanent visual loss. The most common cause is retrobulbar hemorrhage, although other etiologies such as globe perforation, ischemic optic neuropathy and angle closure glaucoma can occur.
Retrobulbar hemorrhage
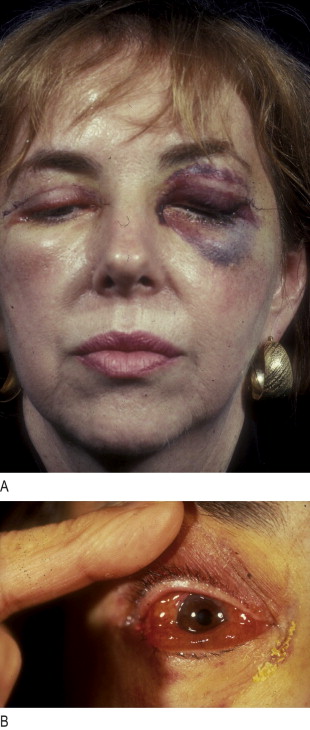
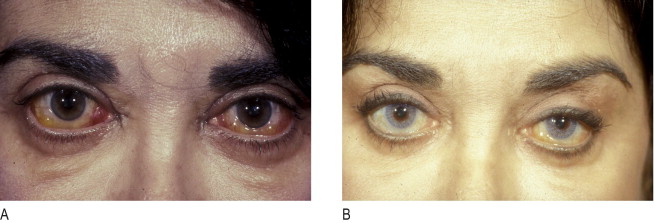
The incidence of post-blepharoplasty retrobulbar hemorrhage causing visual loss was reported in 1974 to be 0.04%. More recently, an epidemiologic study of more than 250,000 blepharoplasty cases found the incidence of retrobulbar hemorrhage to be 0.05%; associated permanent visual loss was diagnosed in 0.0045% ( ). This corresponds to a 1 : 2000 risk of significant hemorrhage and a 1 : 10 000 risk of permanent visual loss. Most hemorrhages occur within the first 24 h after surgery (96%), and of these, more than half occur intraoperatively or within the first six post-operative hours. The most common presenting symptoms are pain and pressure, although less than half of patients present with loss of vision, diplopia, nausea or vomiting. Examination typically shows decreased visual acuity, lid edema, proptosis, subconjunctival hemorrhage, extraocular motility disturbance, increased intraorbital and intraocular pressure and an afferent pupillary defect ( Figure 14.2 ).
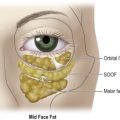
While many theories exist to explain the cause of retrobulbar hemorrhage, the final common pathway involves continued orbital bleeding leading to increased intraorbital and intraocular pressure with resultant ischemic damage to the retina and/or optic nerve. Prevention of this process begins pre-operatively. The history should focus on predisposing factors, such as hypertension, anticoagulant use and vascular disease. An ophthalmic examination is useful for detecting preexisting causes of visual dysfunction. Intraoperatively, control of hemostasis is critical. Koorneef’s description of the delicate connective tissue scaffold connecting the anterior orbital fat to deep orbital fat underscores the necessity to avoid excessive traction during fat excision. It is advantageous to delay wound closure by proceeding to another surgical site, returning later to re-assess hemostasis prior to suturing. Post-operative use of antiemetics and antitussives limits later valsalva maneuvers. Elevation of the head of the bed and use of ice compresses is generally performed. No correlation between retrobulbar hemorrhage and the use of occlusive patching has been found. We do not advocate occlusive dressing believing the downside outweighs any advantages in such a small percentage of patients who do experience a bleed.
Once the diagnosis of retrobulbar hemorrhage is made, the treatment requires immediate attention. The first step should be to identify those hemorrhages that require medical or surgical care, based upon the ophthalmic examination. If the intraocular pressure is elevated, topical and systemic glaucoma medications are utilized. Systemic corticosteroids are used for significant edema. When the bleeding threatens the visual system, or is worsening, surgical therapy is required. The incision is opened widely through the orbital septum and the surgical site and orbit are explored for signs of bleeding. Clots are evacuated and cautery is applied. If the condition remains unresponsive, a lateral canthotomy and cantholysis is performed. In severe cases, both the inferior and superior crus of the lateral canthal tendon can be released. When these measures fail, an emergency CT scan without contrast is warranted. If posteriorly organized hemorrhage is identified, bony decompression may be warranted to relieve orbital apex compression ( Figure 14.3 ). The treatment should be aggressive for the first 24–48 h post-operatively.

Globe perforation
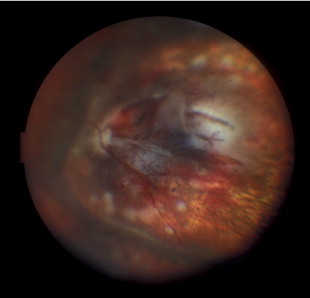
Inadvertent globe penetration can result from any periocular procedure. Caution is necessary during local anesthetic injection, particularly in the thin upper eyelid of older patients. Prevention of this complication begins with the use of protective corneal shields. The range of potential ocular damage from penetration includes an open globe, corneal perforation, traumatic cataract, intraocular hemorrhage, a hypertensive or hypotensive globe, retinal tears and detachment ( Figure 14.4 ). Perforation of the globe is an ophthalmic emergency and necessitates emergency consultation with an ophthalmologist. A Fox shield should be placed over the eye in the interim, broad-spectrum intravenous antibiotics given and the patient should be instructed not to touch the eye.
Central retinal artery occlusion
The potential for central retinal artery embolization following facial and periocular injection has been reported and is secondary to retrograde arterial displacement of the foreign substance from a peripheral arteriole into the ophthalmic arterial system. Prompt ophthalmic consultation is necessary, although the chance of visual recovery is slim; interim treatment involves decreasing the intraocular pressure topically and systemically.
Corneal abrasion
Corneal abrasion is generally a rapidly reversible cause of decreased vision post-operatively. The diagnosis is made by patient symptoms (pain, foreign body sensation, light sensitivity) and is usually apparent immediately after surgery. Diagnostic confirmation can be achieved by evaluating the cornea under a cobalt blue light after instillation of fluorescein ( Figure 14.5 ). Abrasions are often caused by drying of the corneal surface during surgery or inadvertent damage to the surface corneal epithelial layer. Abrasions are treated with ophthalmic antibiotic ointment four times daily, and should resolve within 24 hours. Persistent signs and symptoms should prompt ophthalmologic evaluation.

Dry eye
Corneal irritation is common after blepharoplasty and symptoms are similar to, but less severe, than an abrasion. The diagnosis is made by the observation of punctate corneal staining during cobalt blue slit-lamp examination after the instillation of fluorescein. Treatment is with lubricating drops and ointment.
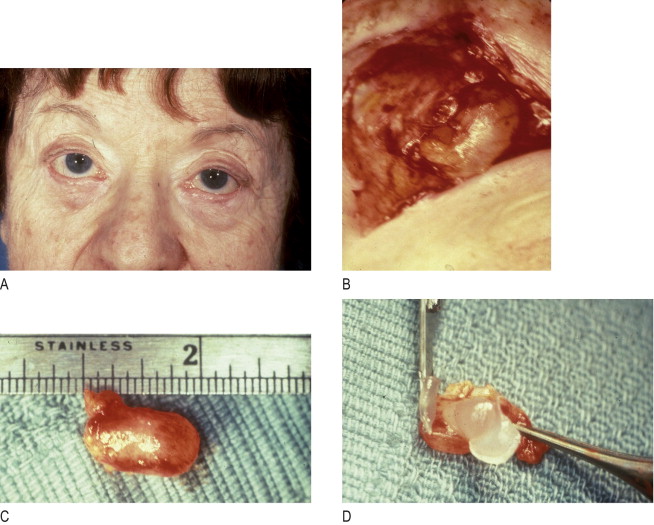
Very rarely, ophthalmic lubricant may be inadvertently introduced into deeper eyelid tissues from a transconjunctival surgical wound. This can result in encapsulation of the ointment within the wounds, and subsequent lipogranuloma formation that responds to excision ( Figure 14.6 ). Although this complication is extremely rare, physicians should keep in mind that excessive amounts of ointment are unnecessary and may result in inoculation of the wound.
Eyelid hematoma
Hematomas usually develop from bleeding of the orbicularis oculi muscle. Evaluation for symptoms consistent with retrobulbar hemorrhage should proceed first. Once ruled out, mild superficial hematomas are treated conservatively with ice compresses. Larger, stable hematomas should be followed for 7–10 days, until adequate liquefaction has occurred. Rarely do they need to be drained by needle aspiration or reopening of the wound. In severe cases, they may result in tissue fibrosis and lid scarring. Expanding hematomas require immediate surgical exploration, evacuation and hemostasis.
Infection
The development of cellulitis or abscess formation is extremely uncommon in the well-vascularized eyelid. Nonetheless, infections can occur, rarely leading to visual loss. Orbital cellulitis manifests by excessive pain, eyelid swelling, erythema, conjunctivitis, decreased visual acuity, diminished extraocular motility and pupillary abnormalities ( Figure 14.7 ). Contrast-enhanced computed tomography is effective in diagnosing an orbital abscess. Patients are managed by culturing purulent discharge and are treated with broad spectrum antibiotics for 7–10 days. Abscesses usually require surgical drainage.

Eyelid sloughing
Eyelid necrosis can follow inadvertent injection with formaldehyde or other substances. Complete eyelid sloughing can develop, necessitating multiple eyelid reconstructive procedures and setting the patient up for scarring, persistent lagophthalmos and chronic ocular irritation from dry eye ( Figure 14.8 ).

Chemosis
Conjunctival edema can develop in the early or intermediate post-operative period as the result of incomplete eyelid closure, ocular allergy, sinusitis or surgical edema with poor lymphatic drainage. Chemosis can be worsened by systemic conditions, such as renal failure ( Figure 14.9 ). Corneal drying may occur, as the edematous conjunctiva balloons around the cornea preventing adequate tear film dispersion. Additionally, the exposed conjunctival surface may keratinize, leading to ocular irritation. Treatment is with preservative-free artificial tears and ointment. A mild topical steroid eye drop can be prescribed, but the patient must be followed for potential elevation of the intraocular pressure and development of secondary infectious keratitis. Systemic steroids can be used in severe cases. Rarely, a temporary suture tarsorrhaphy may be needed.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


