| Paralytic lagophthalmos |
| Exposure keratopathy |
| CN VII palsy |
| Failing/exposed corneal transplant |
| Neurotrophic cornea |
| Recalcitrant corneal infections |
| Debilitating corneal pain |
| Presence of Bell’s phenomenon |
| Degree of lagophthalmos |
| Corneal epithelial staining |
| Orbicularis strength |
| Anterior or posterior lamellar shortage |
| Prior eyelid, facial surgery or trauma |
| History of head and neck cancer treatment, especially involving facial nerve |
| Corneal sensation |
| History of thyroid eye disease/proptosis |
Introduction
A conjunctival pillar tarsorrhaphy is suitable for treating corneal exposure that is refractory to medical management. The size and location of the conjunctival pillar can be customized for the degree of corneal exposure. Exposure of the medial cornea, in particular, is difficult to treat with permanent tarsorrhaphy ( Chapter 46 ) without significantly constricting the horizontal palpebral aperture. A conjunctival pillar tarsorrhaphy can be rapidly reversed in the clinical setting and is cosmetically superior to permanent lateral tarsorrhaphy.
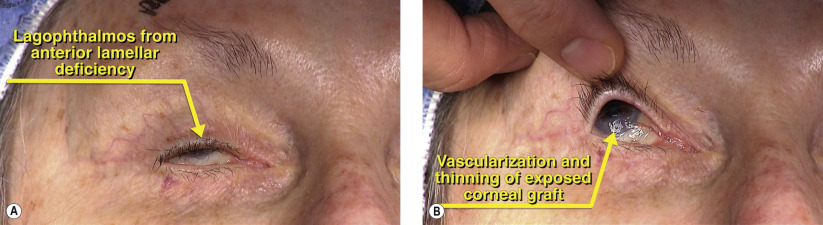
Patients with a history of impending failure or recurrent penetrating keratoplasty with corneal exposure are particularly suited for conjunctival pillar tarsorrhaphy. The conjunctival pillar continually lubricates the corneal graft with blinking and routine eye movements while maintaining a normal vertical aperture to allow for instillation of topical medications and slit lamp examination. Recurrent corneal infections, viral, bacterial or protozoal, may be considered after failed medical management. Acquired or heritable causes of neurotrophic corneas are other indications for treatment.
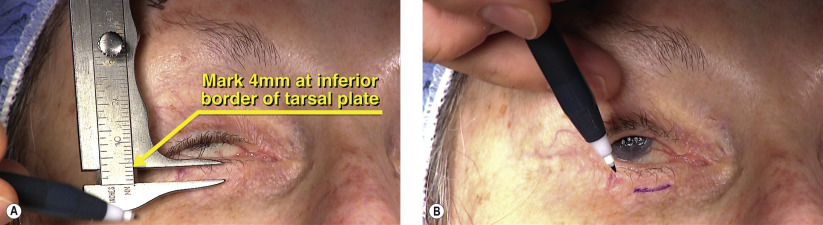
The surgery involves raising a tarsoconjunctival flap from the upper eyelid and fusing this to the lower eyelid. The pillar can easily be severed in the clinical setting with topical anesthesia and no disfiguring sequela.
Surgical Technique