Introduction
Venous insufficiency is an extremely common problem. According to the Framingham study, there are more persons in the US with venous insufficiency than with coronary and peripheral artery disease. Many patients with venous insufficiency do not seek medical attention until late in the course of the disease, and in many of those who do seek medical help, venous insufficiency is not adequately diagnosed or treated. Most patients with venous problems have leg heaviness, edema, pruritus, or other symptoms for years (or even decades) before they get medical advice. Some seek medical help for the first time after they have had bleeding from a varicose vein or after they have developed a venous stasis ulcer which indicates the final stage of venous insufficiency.
Although most physicians know that compression is the treatment of choice for venous insufficiency, there is a lack of proper understanding on when and how to prescribe compression garments. For example, practitioners frequently prescribe stockings to patients with untreated leg swelling with the hope that the garments will reduce the edema. However, stockings are designed to keep edema from forming and only minimally reduce existing leg edema.
The varicose veins and venous insufficiency should be treated by correcting the underlying problem, managing symptoms, and managing and preventing complications. As discussed elsewhere in this book, venous hypertension due to reflux or obstruction is common in patients with varicose veins. The pathophysiology of venous hypertension is complex, and a full review goes beyond the scope of this chapter. However, it is important to keep in mind the mechanisms that lead to edema formation and the damage to the veins and skin that result from sustained venous insufficiency and are responsible for the signs and symptoms of this disorder.
In this chapter, I will discuss the use of different compression devices to manage venous insufficiency and its complications, such as edema, pain, and ulceration. I will describe the initial management of edema with compression bandages, such as Unna boots, short-stretch bandages, and multilayer bandages. This information will help the reader to manage efficiently edemas of etiologies other than to venous insufficiency. These bandaging techniques are invaluable for managing venous stasis ulcers.
Although my focus will be on the use of compression stockings, I will also discuss alternatives for patients who are unable or unwilling to use compression stockings. These devices have allowed us to treat edema in patients with abnormally shaped limbs, peripheral neuropathy, or concomitant peripheral vascular disease, in whom standard compression may be associated with complications such as skin breakdown, inadequate distribution of compression forces, or limb ischemia. The goals of compression therapy in the patient with venous insufficiency are to reduce the amount of blood in the lower extremities, promote venous flow from the superficial venous system to the deep venous system, prevent edema fluid from accumulating, and improve associated symptoms such as pain, heaviness, and overall discomfort. The use of compression stockings is of great value in the prevention or amelioration of the post-thrombotic syndrome and is an important tool after endovenous ablation, microphlebectomy, or sclerotherapy of incompetent veins ( Table 12.1 ). Although we live in an era of evidence-based medicine and I have presented the most up-to-date information, there have been no rigorous studies on the effectiveness of compression therapy. Therefore, many of the recommendations come from experience and individual observations. As always in medicine, common sense combined with continuous learning should guide practitioners in the art of prescribing. I also offer cost-effective alternatives, because compliance is often jeopardized by the cost of compression garments, which are not always covered by insurance companies.
| Condition | Compression bandages | Compression garments |
|---|---|---|
| Unresolved edema | X | |
| Lymphedema | X | X |
| Severe stasis dermatitis (acute deep or superficial) | X | |
| Venous thrombosis | X | |
| Venous stasis ulcer | X | X |
| Varicose veins | X | |
| Prophylaxis and treatment of post-thrombotic syndrome | X | X |
| Maintenance of limb volume after edema reduction | X | X |
| Prevention of venous stasis ulcer recurrence | X | |
| Deep vein thrombosis prophylaxis | X | |
| Venous insufficiency | X | X |
Physiology and Anatomy
As described earlier in this book, the venous system is a network of deep and superficial veins interconnected by perforating veins that bring blood from the low-pressure superficial system into the deep veins. Venous return from the periphery to the heart relies mainly on the negative pressure created during inspiration and by the contractile activity of the calf muscles. Valves promote unidirectional blood flow, and their ability to work effectively is critical for fighting gravity between breaths and muscle relaxations.
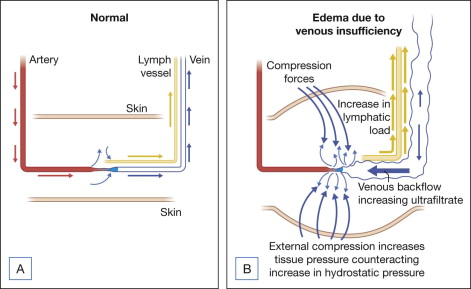
The main cause of venous insufficiency is malfunctioning valves due to post-thrombotic syndrome, obstruction, or primary degeneration of the venous wall. If the valves fail to close, the column of blood distal to the malfunctioning valve increases. This increases the hydrostatic pressure, which is transmitted all the way to the capillary level and increases blood ultrafiltrate. As a result, edema forms that initially is clinically not noticeable, because the lymphatic vessels compensate for the increase of interstitial fluid formation. When the lymphatic transport gets saturated, the patient develops phlebolymphedema that gets progressively worse if the venous hypertension is not resolved. In addition to edema formation, extravasation of white and red blood cells, plasma proteins, and alpha-2-microglobulin lead to chronic inflammation, dermatitis, hyperpigmentation, tissue damage, growth factor trapping, local hypoxia, and lipodermatosclerosis. The increase in ultrafiltration can only be alleviated by treating the underlying condition (e.g., thrombus) or by increasing the tissue pressure trough external limb compression ( Fig. 12.1 ).
Patient Selection
Patients need to have sensation in the affected limb and be able to communicate, because excessive pressure could cause pain from ischemia resulting in ulceration or tissue necrosis. Ideally, patients should be able to apply and remove the garments by themselves or they should have a provider who is able to assist with these tasks. Elderly and debilitated patients are less likely to tolerate higher levels of compression and associated conditions such as arthropathy, morbid obesity, and paresis need to be considered before prescribing a particular garment or bandage. Sometimes it is better to accept lower degrees of compression and have the patients comply with treatment than to insist in higher compression and have the patient reject treatment at all due to discomfort or incapacity of getting the garments on. Common factors affecting the prescription of compression therapy are discussed in Box 12.1 .
- •
Shape of leg
- •
Age of patient
- •
Skin characteristics
- •
Presence of arthritis or obesity
- •
Weakness
- •
Presence of peripheral vascular disease
- •
Extension of varicosities (knee versus thigh versus genital)
Types of Compression
Compression therapy has been used for centuries to manage venous insufficiency and varicose veins. The ancient Greeks applied tight leather boots to contain the swelling. Today, natural and synthetic materials are used to produce compression stockings and bandages. Bandages can be characterized as long or short stretch based on the degree of elasticity. Inelastic fabric can also be used to manage severe venous insufficiency.
The choice of the compression to be used on each patient should be individualized, and several factors should be considered to optimize outcome and assure patient compliance. Most patients with varicose veins do not need bandages, unless the swelling is not resolved by elevation of the affected limb. Practitioners should not use long-stretch bandages such as ACE ® wraps on these patients, because long-stretch bandages provide high resting pressures that could cause skin ischemia when the patient is supine ( Table 12.2 ). Patients with edema should be bandaged with short-stretch bandages such as Comprilan ® . This type of bandage provides low resting pressure and high active pressures when the patient walks.
| Compression type | Indication | ||||
|---|---|---|---|---|---|
| Edema reduction | Ulcer | Edema treatment | Post-phlebotic syndrome | Post-procedure after ablation, phlebectomy, sclerotherapy | |
| Short-stretch bandage | X | X | X | X | X |
| Medium-stretch bandage | X | X | X | X | |
| Long-stretch bandage | X | X | |||
| Multilayer compression system | X | X | |||
| Unna’s boot | X | X | |||
| Compression legging a | X | X | X | X | |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


