Introduction
Breast augmentation with fat has evolved over the past 12 years. According to the American Society of Aesthetic Plastic Surgery, fat transfer to the breast dramatically increased 41% over 2016, and this trend does not appear to be diminishing. Core breast volume augmentation with fat alone, despite its potential, has experienced poor adoption because of patient and physician opposition to BRAVA pre-expansion and the graft to capacity limitations of enlarging breasts with fat in one session.
With prosthetic implants alone, the revision rate remains high and a majority can be attributed to soft tissue failure, which is not necessarily failure of the prosthesis but lack of sufficient breast tissue leading to unappealing visibility. With a sudden spike in the interest of fat grafting, many sought to rely on fat for core volume augmentation; however, its limitations for this application are analogous to the “mountains of sand” theory, in which core volume is lost at the expense of a wide breast base. This drawback paved the way for a new concept in which the combination of core volume projection of an implant and the soft, natural appearance and impression of fat provided an ideal solution to the world of primary breast augmentation.
As an offshoot of this experience, some, including the senior author, sought to obtain the core projection using an implant and surround this with fat to obtain the best of both worlds—the so-called composite breast augmentation. , ,
Since that time, composite breast augmentation has gained popularity to manage a variety of cosmetic and reconstructive problems. This chapter will focus on composite breast augmentation’s evolution into a spectrum of fat-to-implant ratios and clinical cases in which these ratios make surgical sense.
Indications and Contraindications for Composite Breast Augmentation
The classic patient who benefits from composite breast augmentation has small breasts and inadequate breast tissue to cover her desired implants. In an implant-only world, if one follows the classic Tebbetts/Adams “high five” principles, the surgeon is faced with either placing an inadequately small implant in a patient or violating her soft tissue footprint to maintain a narrow cleavage gap. In the composite scenario, the surgeon does not violate the native soft tissue footprint and instead it helps maintain the high five principles. Composite breast augmentation liberates us from this predicament by placing small implants with a narrow diameter and is allowing the fat to do the transitional filling of the cleavage gap instead of the implant.
Contraindications for a composite procedure are similar to those for liposuction, including patients with a significant family history of breast cancer, unreasonable expectations with regard to size and shape, or unwillingness to undergo touch-up procedures for further volume and filling of the cleavage gap. In addition, as noted earlier, patients desiring implant removal after capsular contracture or other device-related issues are likely better candidates for simultaneous implant exchange with fat (SIEF) rather than a composite breast augmentation.
Preoperative Evaluation and Special Considerations
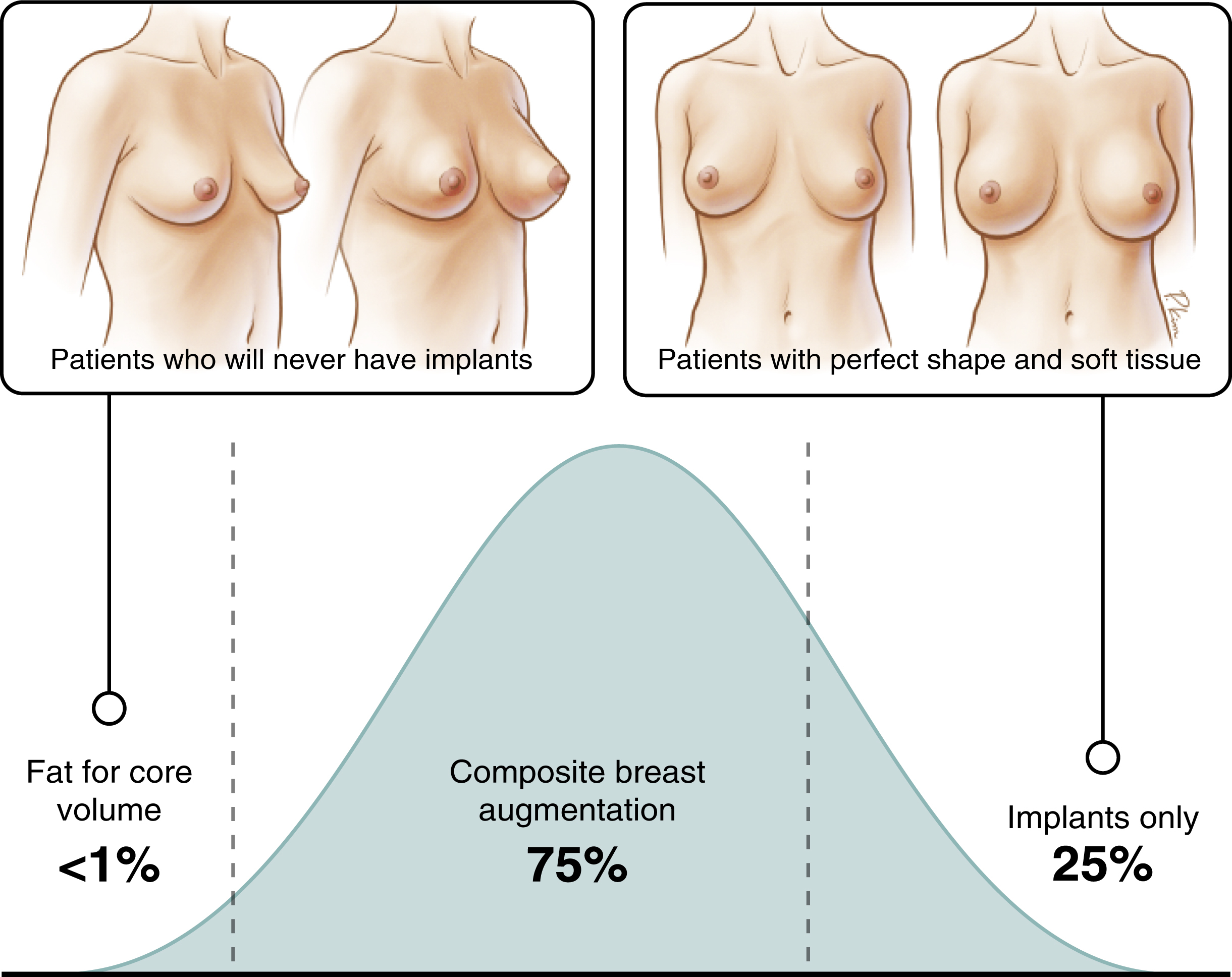
The majority of patients presenting for primary breast augmentation are candidates for a composite procedure ( Fig. 7.1 ). The implant provides the core volume projection, and the fat delivers width and transition and addresses asymmetries. Unlike other composite approaches, the implants and fat are co-dependent. The ideal patient would be one with inadequate soft tissue and a thin body frame. The sharp transitions can be addressed with fat and the optimal 45/55 rule achieved without an anatomic implant. Patients with adequate soft tissue and ideal breast aesthetics are candidates for implants alone; however, this group tends to vary among practices and does not embody all patients. A third group of patients who desire larger breasts but do not favor prosthetic devices make up the “padded bra” cohort. These women desire larger breasts but do not want breast augmentation. Some of these women may seek out core volume fat augmentation.
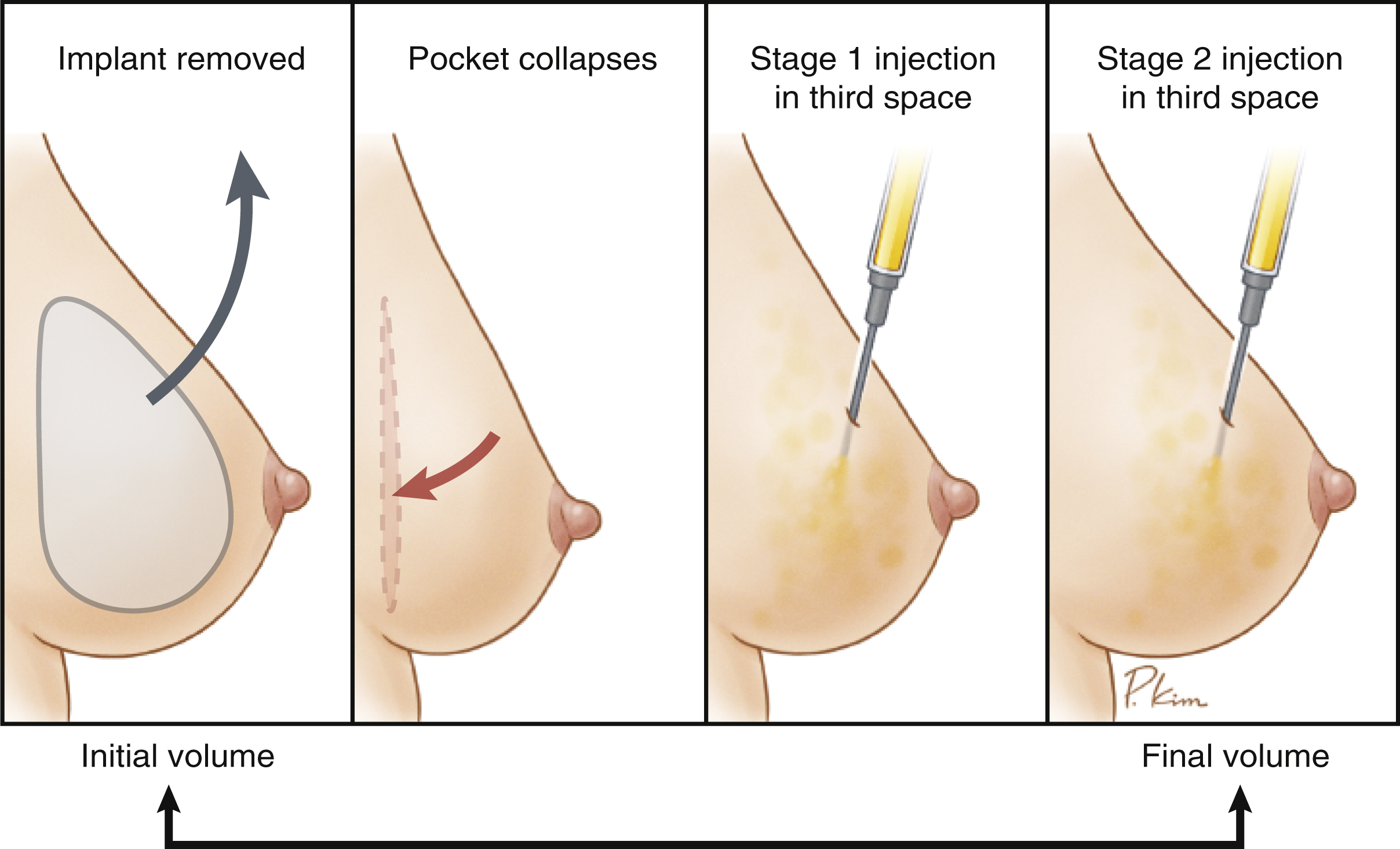
Within the composite spectrum, three different scenarios were created. These include type 1: subglandular or subfascial primary breast augmentation and fat overlay, type 2: submuscular primary breast augmentation with implants and fat, and type 3: revision breast augmentation using implants and fat ( Table 7.1 ). The senior author prefers a subfascial approach with fat overlay because this prevents animation deformities and lateral malposition of the implant. In type 3 patients, pre-expansion with BRAVA is usually required to significantly increase the third space recipient site, usually two to three times the volume of the subcutaneous tissue.
| Implant Plane | Anatomic Boundaries | Capacity of Third Space | Volume Possible to Graft | Location on AP Footprint |
|---|---|---|---|---|
| Subglandular | Superficial subcutaneous fat | Low | 50–100 | Periphery, mainly upper border |
| Subfascial | Subcutaneous fat to fascia | Medium | 50–200 | Periphery |
| Submuscular | Subcutaneous fat, fascia, muscle | High | 50–500 | Complete implant overlay |
a The versatility of implant position and fat offers three primary composite breast augmentation approaches. Each approach differs by the capacity of the recipient site. In general, the deeper the implant plane, the larger is the capacity of the space of the breast.
Fat transplantation to the breast can be divided into three major categories: core volume fat transplantation to the breast with BRAVA pre-expansion, SIEF, and composite breast augmentation, each with its own applications. , , Of the three categories, composite breast augmentation is positioned to be the most common technique for all patients requiring some form of fat transfer to the breast (see Fig. 7.1 ).
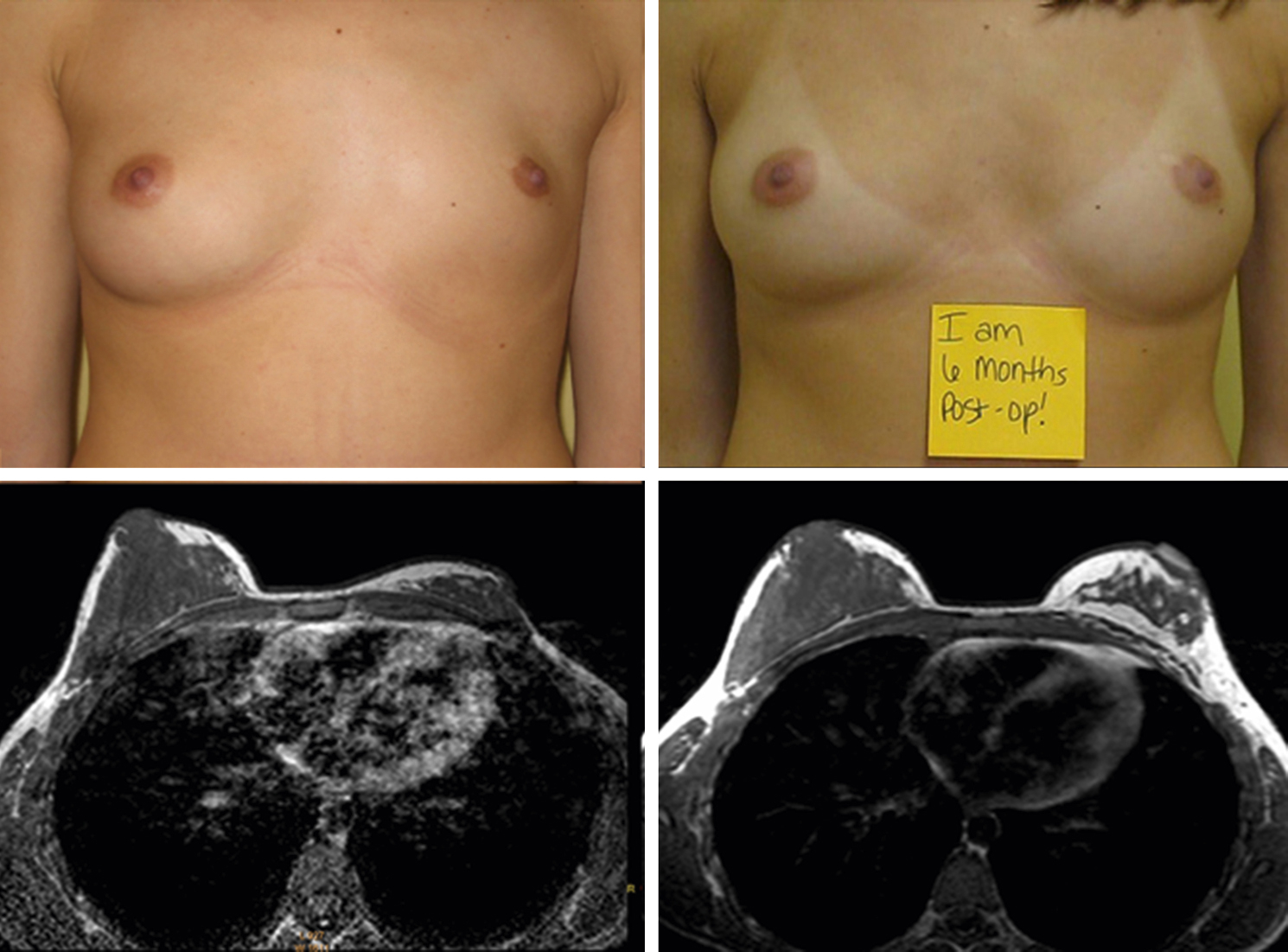
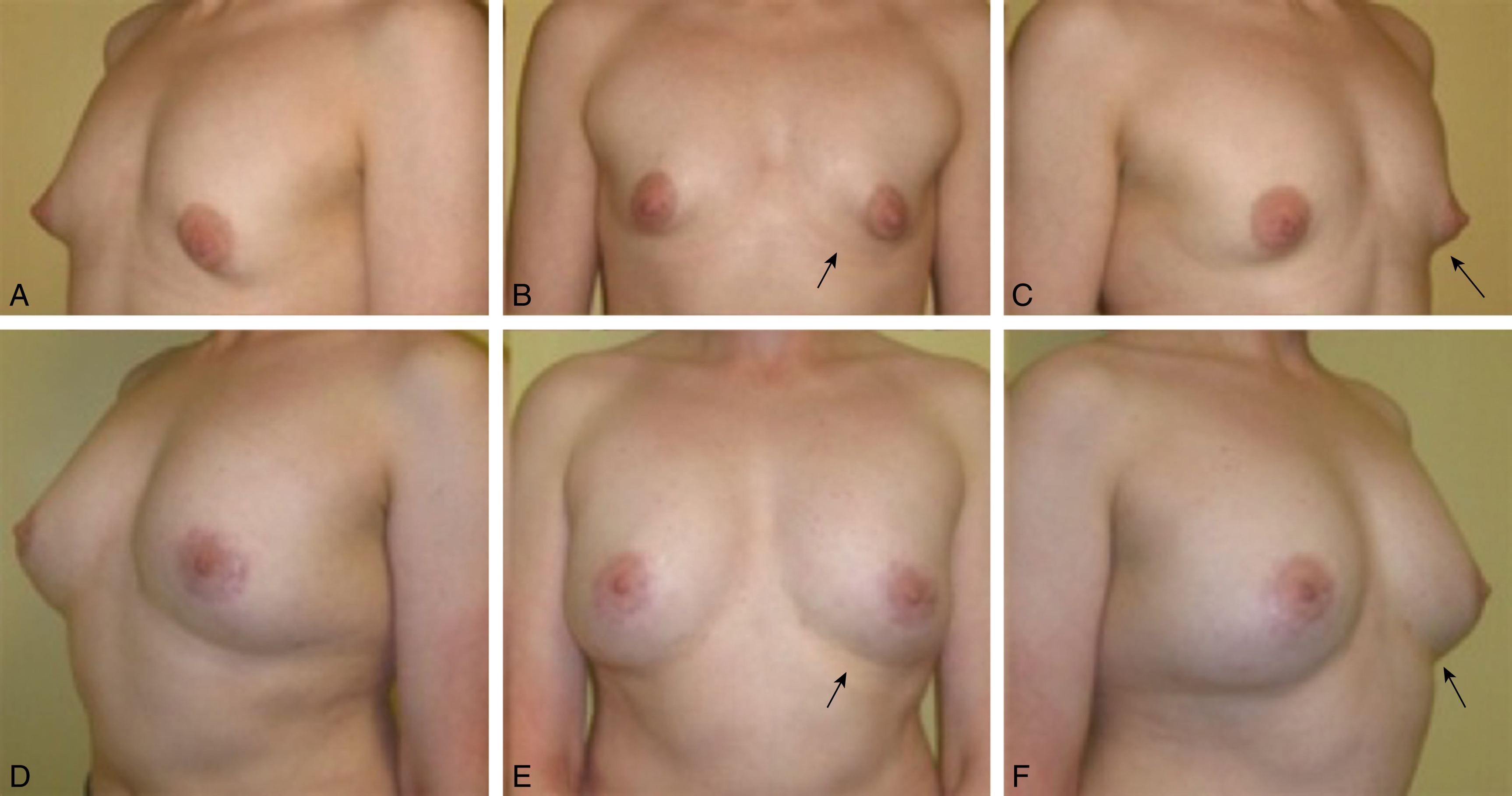
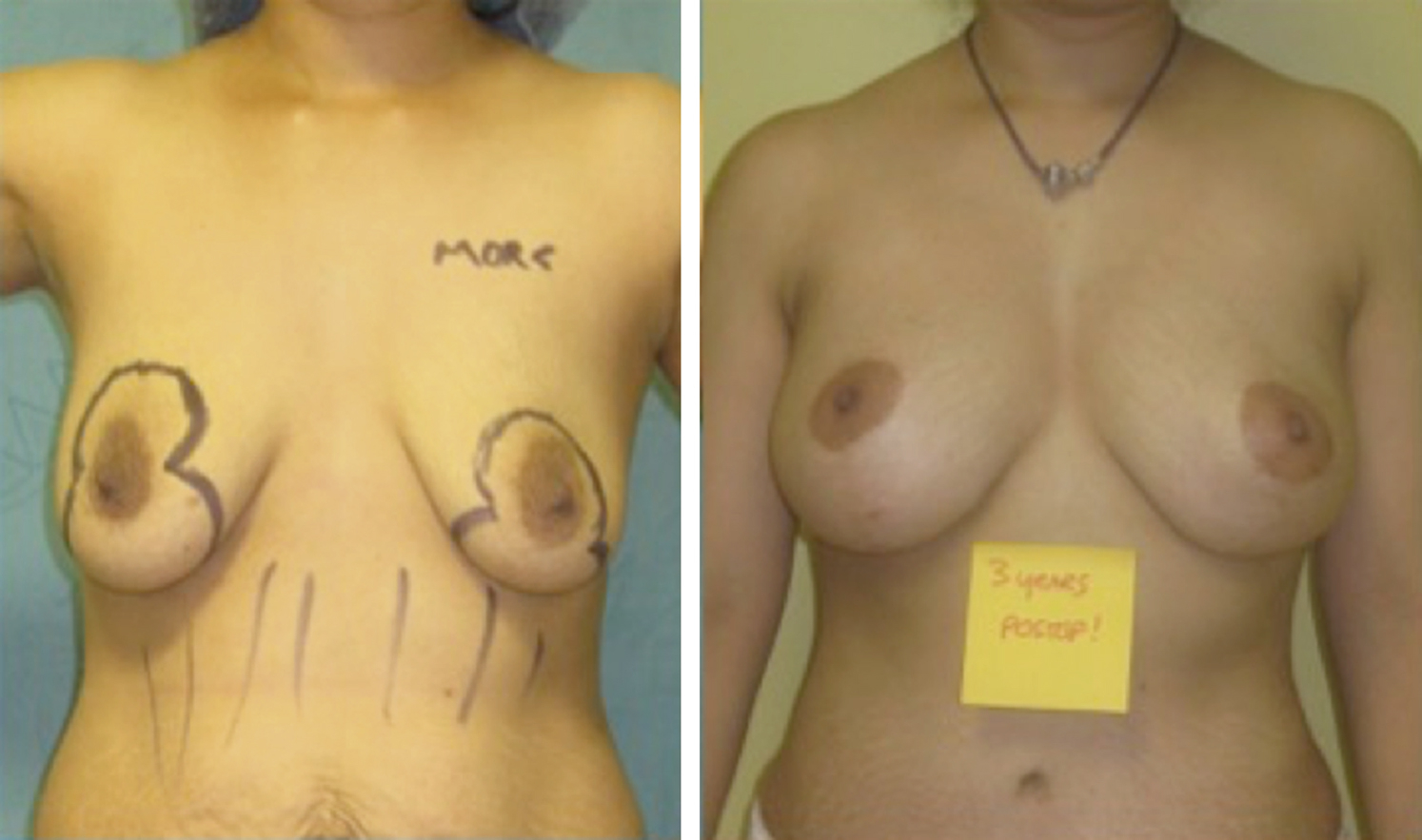
Fat for core volume transplantation for primary breast augmentation is a reliable solution for less than 1% of patients (see Fig. 7.1 ). However, comparable to the mountains of sand analogy, fat is a poor material to provide projection, and as more fat is transplanted, even with BRAVA pre-expansion, this leads to an undesirable wide breast base without a robust centrally projected mound ( Fig. 7.2 ). Nevertheless, core volume fat transplantation remains useful in severe congenital asymmetries, constricted breasts, or use with a mastopexy only to obtain volume restoration ( Figs. 7.3–7.7 ). Targeted fat transplantation affords preferential fill of the breast in the lower pole, obviating the need for anatomic textured implants to achieve the Mallucci 45:55 ideal beautiful breast ratio ( Fig. 7.8 ).




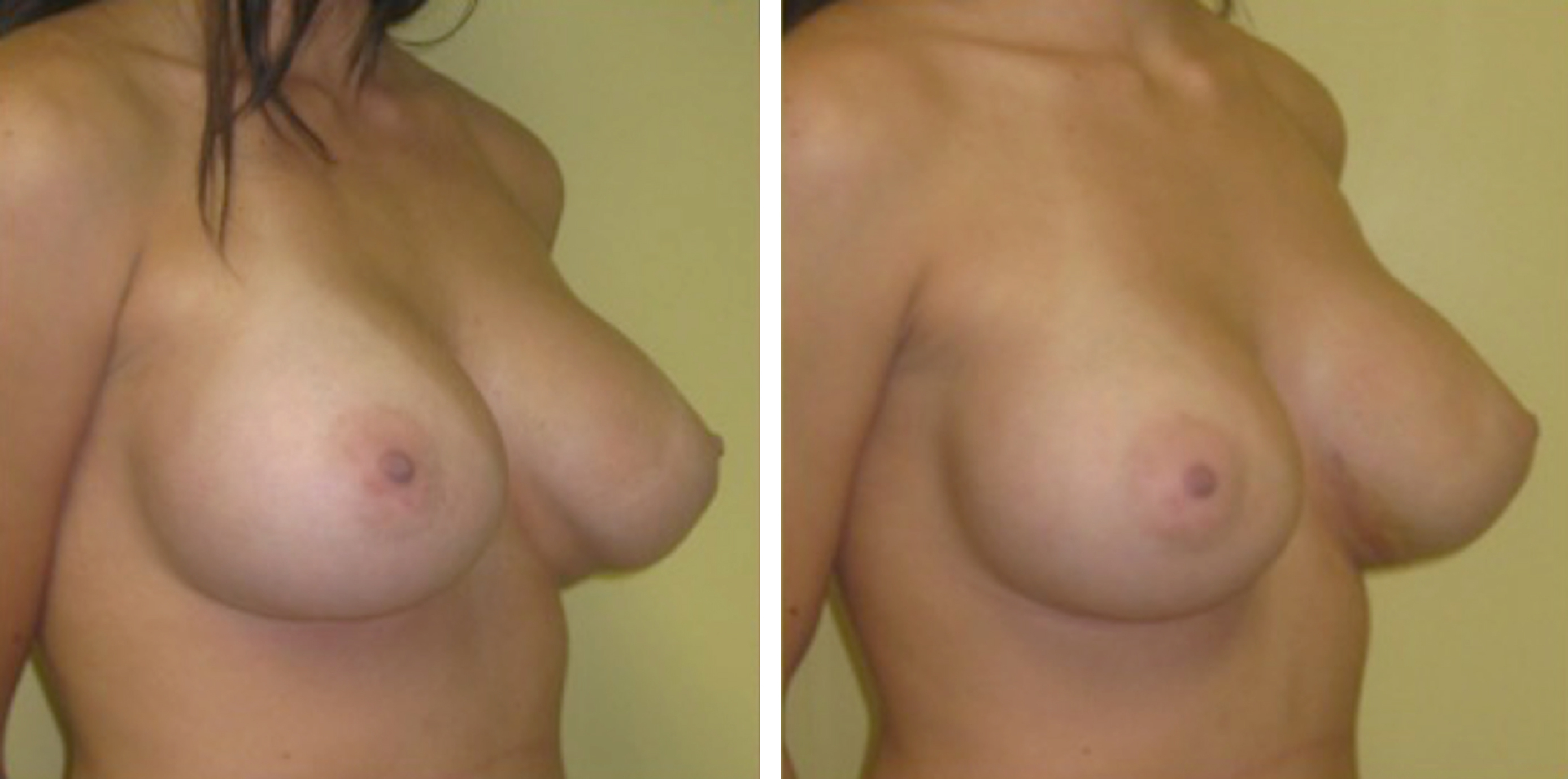
At times, breast deformities after implant placement may be due to soft tissue failure rather than implant malposition. In these cases, one may modify the soft tissue over the device and not replace the implant for a notable improvement ( Fig. 7.9 ). However, when all else fails, one must remove the implant. In these cases, SIEF, initially described in 2012 by the senior author, affords a viable option for patients needing prosthetic device removal. Here, pre-expansion of the breast before removal of the implant and subsequent placement of fat in the third space of the breast mound, provides an independent plane for fat placement to help alleviate breast deformities and asymmetries secondary to capsular contracture or implant drift ( Fig. 7.10 ). , , ,