Choledochoduodenostomy
Michael A. Zimmerman
Igal Kam
DEFINITION
Biliary reconstruction during cadaveric or living donor liver transplantation (LDLT) is predominantly performed in duct-to-duct fashion using the Roux-en-Y choledocho- or hepaticojejunostomy as an alternative. However, direct anastomosis of the bile duct to the duodenum is a viable and safe alternative: choledochoduodenostomy (CDD) or hepaticoduodenostomy (HD). This reconstructive technique has been historically used sparingly in the treatment of benign biliary obstruction and repair of major bile duct injuries.
PATIENT HISTORY AND PHYSICAL FINDINGS
In the setting of transplantation, several elements of the patients’ history may raise the surgeon’s awareness that bile duct viability during liver transplantation may be in question.
Although the final decision is made following careful intraoperative assessment of the patient/recipient’s bile duct, direct duodenal anastomosis may prove most useful in the setting of autoimmune disease, retransplant, cholangiocarcinoma +/− radiation, or in a patient with an extensive history of abdominal surgery with dense adhesions.
IMAGING AND OTHER DIAGNOSTIC STUDIES
In addition to ABO compatibility, the potential recipient should undergo standard pretransplant laboratory evaluation required for listing.
Anatomic assessment of the bile ducts in patients with suspected biliary stricture or cancer is generally assessed with endoscopic retrograde cholangiopancreatography (ERCP). This approach facilitates evaluation of the entire biliary tree including the relationship of a dominant stricture or mass to the distal common bile duct.
Computed tomography (CT) may further characterize this relationship and identify concomitant liver pathology including additional lesions, arterial variation, and portal vein thrombosis.
In the event that ERCP is not possible, magnetic resonance imaging (MRI) may provide adequate biliary characterization.
SURGICAL MANAGEMENT
Preoperative Planning
The final decision to perform a CDD or HD is made intraoperatively at the time of the biliary anastomosis.
Positioning
Liver transplant is always performed in the supine position. Placement of nasogastric tube is necessary to reduce gastric and duodenal distension.
TECHNIQUES
ASSESSMENT OF RECIPIENT BILE DUCT
The recipient bile duct is carefully assessed following reperfusion of the transplanted liver. The entire abdomen must be inspected carefully, especially in the setting of previous surgery and severe abdominal adhesions.
If the bile duct is determined to be not viable, the remainder of the extraduodenal duct may be completely resected if necessary and sent to pathology for a frozen section examination in the setting of cancer. The remainder of the bile duct stump is then oversewn with a 5-0 Maxon suture.
POSITIONING OF THE BILE DUCT AND DUODENUM
Assessment of the bile duct length and position relative to the duodenum can be easily performed at this point. Placing several lap pads behind the right lobe of the liver may provide easier alignment with the retractor in place and simulate liver positioning when the incision is closed.
If the bile duct appears to be too short to reach a viable portion of the duodenum, perform a Kocher maneuver to allow for optimal positioning of the duodenum relative to the distal bile duct of the allograft.
In the setting of previous radiation, the duodenum should be carefully inspected for radiation injury.
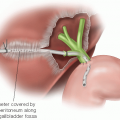
In LDLT, multiple ducts are not uncommon. If the ducts are close in proximity, a single 5-0 Maxon suture can be used to run the back wall and create a common cuff (ductoplasty) and thus a single anastomosis is performed. If this is not feasible, each duct can be anastomosed to the duodenum individually over a stent (FIG 1A,B).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree