Chin Augmentation With Implant
Daniel A. Cuzzone
Barry M. Zide
DEFINITION
Chin augmentation encompasses genioplasty with the use of mandibular osteotomies as well as placement of implants in the form of grafts or alloplastic materials. Herein we do not discuss osteotomies.
The chin is a defining feature of the lower one-third of the face that connotes a sense of strength to the face.
Correction of microgenia is desired in about 20% to 25% of patients undergoing rhinoplasty, with the goal of balanced facial symmetry.
Implant-based augmentation of the chin may be performed with a variety of implant-based materials, each with its own set of benefits and perceived deficiencies (TABLE 1).
Osteotomies to advance the lower border of the symphysis may accomplish the same thing, but the risks and benefits of each are not described herein.
ANATOMY
The chin, as an anatomical subunit, is composed of the sublabial area and the pad.
The mental nerve is the terminal branch of the inferior alveolar nerve. It is a branch of the third division of the trigeminal nerve and is responsible for sensation of the lower lip, portions of the chin pad, and menton (FIG 1A, blue area) except for a small area that is supplied by a sensory branch off the nerve to the mylohyoid (see FIG 1A, pink area; FIG 1B).
The location of the mental foramen can be variable (FIG 2).
Anatomical studies have demonstrated that the mental foramen is located inferior to the second mandibular premolar in about 50% of adults, between the first and second premolar in 25%, and posterior to the second premolar in 25% of the remaining population.
It is located about halfway between the alveolar ridge and the inferior border of the mandible (8 to 10 mm from the inferior border) and is between 2 and 3 cm lateral to the midline.
Table 1 Implant Subtypes and Characteristics
Material
Trade Name
Tissue Interface
Pros
Cons
Complications
Polydimethylsiloxane
Silastic (silicone rubber)
Fibrous capsule
Easily carved, easily placed and removed
Bone resorption (if too high), seroma, exposure
Malposition, extrusion, infection (may be salvaged)
High-density porous polyethylene
MEDPOR
Su-Por
Limited tissue ingrowth
Versatile
Difficult to remove; requires hardware
Malposition, extrusion, infection (not salvageable)
It may be lower in vertically short height mandibles.
The mentalis muscles are paired mimetic muscles that elevate and compress the chin against the anterior mandible and indirectly raise the lower lip (FIG 3).
PATHOGENESIS
Congenital and acquired factors may contribute the most to a hypoplastic mentum.
Aging
Dentures that cause trauma to the mentalis origin may lead to soft tissue ptosis and poor projection.
PATIENT HISTORY AND PHYSICAL FINDINGS
A pertinent history and physical exam are instrumental in optimal operative outcomes and should include an appreciation for the patient’s aesthetic goals, history of prior facial surgery, or orthodontic/orthognathic treatment, and a comprehensive facial examination.
Lip eversion and position
Occlusion
Static chin pad thickness (normal 9 to 14 mm)
Labiomental fold depth and height
Dynamic chin pad motion while smiling (the pad may be effaced and in some cases may descend)
Symphyseal narrowness
Assessment of lip position should be noted.
Normal interlabial gap is up to 3.5 mm.
Normal lower incisal show at rest is 2 to 3 mm.
Normal upper incisor show is up to 3.5 mm in males and up to 5.5 in females.
Lower facial height should be noted. Sagittal implant projection will give the face a longer appearance; conversely, if the chin is deficient sagittally but long, an implant will not work well.
Symmetry of the chin should be noted as well as skin irregularities.4
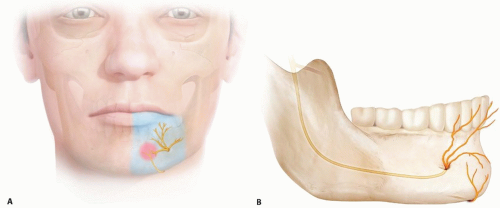
FIG 1 • A. Sensory distribution of the mental nerve seen in blue and the contribution of the sensory branch of the never to the mylohyoid in pink. B. Course of the sensory branch off the nerve to the mylohyoid (denoted by the dotted white circle).
Dimpling may be seen after previous surgery, injury, or facial lesion such as Bell palsy.
Assess in repose and during animation both from the frontal and profile view.
When the chin symphysis is narrow, bony advancement may be inadvisable vs prosthetic augmentation.
Dental occlusion
Prominent teeth may evert the lower lip, producing a more acute labiomental fold. A vertically high implant may worsen this. Also, a skeletally deep bite may seem to shorten the face with the occlusion, allowing the upper teeth to push the lower lip forward.
IMAGING
High-definition preoperative photography is important for photo documentation and for perioperative planning.
Views that should be obtained include frontal and lateral, with and without smile. The smile view shows how the chin pad moves dynamically.
Radiographic evaluation is often reserved for secondary surgical procedures, with short mandibles where the mental foramina may be low, or to evaluate prior hardware.
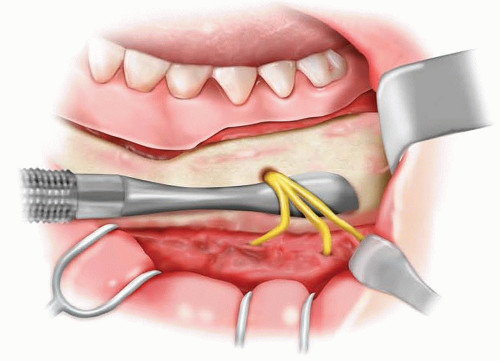 FIG 2 • Mental nerve as it exits from the mental foramen in the body of the mandible at about the level of the second premolar. |
IMPLANT SELECTION
Ideally, only small and medium silicone implants should be utilized because the larger ones tend to result in more erosion.
SURGICAL MANAGEMENT
Preoperative Planning
Single oral or intravenous dose of antibiotic is provided as per the surgeon’s preference.
Implant-based chin augmentation can be performed under local anesthesia with oral sedation or with intravenous sedation with proper supervision.Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


