CHAPTER 6 Applied Anatomy
KEY POINTS
The lymphatic system plays an important role in transporting tissue fluids and extravasated plasma proteins back to the bloodstream and absorbing lipids from the intestines.
The lymphatic system is composed of collecting vesels and lymph nodes and comprises five distributions: superficial, deep, communicating, perforating, and visceral.
The superficial lymphatic system includes two subsystems: epifascial and interfascial.
Research into the anatomy of the lymphatic system and its links to functional status has been and continues to be a controversial subject, in part because of the great complexity of the methods for its visualization and the complexity and variability of the lymphatics between individuals.
More than 30 years ago, Caplan and Ciucci of Buenos Aires University began working in the area of vascular anatomy, with a focus on the lymphatic anatomy, developing and adapting a range of techniques for visualization.
Our research, the results of which are indicated in this chapter, is a continuation of their work and was carried out by our group in the Third Normal Anatomy Department of Buenos Aires University. In this chapter we will summarize our findings on the anatomy of the lymphatic system, focusing on the lymphatic drainage of the breasts and limbs, to increase understanding of the anatomic basis of lymphedema.
Research Methods
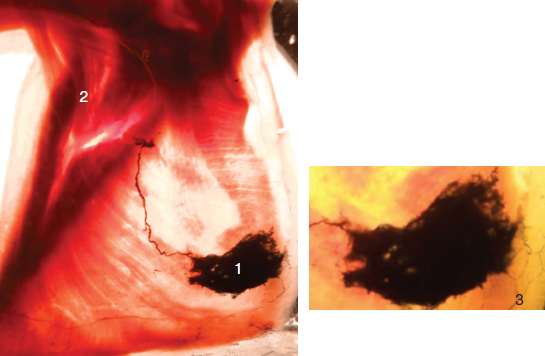
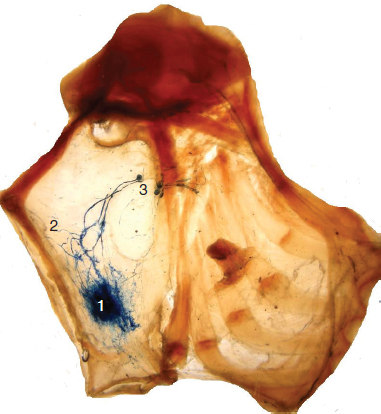
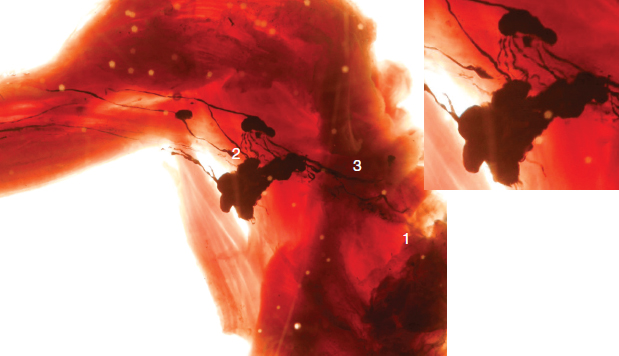
We began our anatomic study of the lymphatic system using a range of staining techniques (such as China ink, latex, Berlin blue, and others) that progressively improved over the years. We primarily used the Gerota method, which employs a mixture of turpentine essence, Prussian blue, and sulfur ether, as described by Dimitrie Gerota in 1896. We modified his method by replacing the sulfur ether with heat to dilate the lymph capillaries.
To visualize the lymphatic vessels and the lymph nodes without risk of injuring them during dissection, and to enable our research into the morphology of the lymphatic system, its variant drainage, and the relationship with subfascial lymphatics, we added diaphonization by the Spalteholz technique. This technique is employed after fixation and clearing of the cadaveric material. First the specimen is dehydrated using alcohol, then it is immersed in xylol, thus changing the refractive index and making it possible to generate a three-dimensional image. 1 , 2
General Considerations
The lymphatic system plays an important role in transporting tissue fluids and extravasated plasma proteins back to the bloodstream as well as absorbing lipids from the intestinal tract. It is also important for the immune response and is one of the main routes for the metastatic spread of tumor cells.
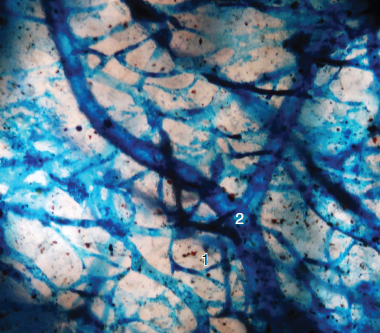
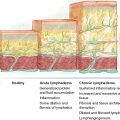
The system starts in the interstitial space with the initial lymphatic capillaries (Fig. 6-1). It drains the lymph through the collecting vessels, which is then filtered in the lymph nodes and finally cleared into the venous system. It is distributed throughout the body, except for the central nervous system, where the perivascular spaces have a prelymphatic or paralymphatic function.
Lymphatic System Distribution
Topographically, the lymphatic system can be separated as follows:
Superficial system: Drains the cutis and subcutis. In terms of the lower-limb lymphatic drainage, in the superficial system there are two subsystems:
The epifascial system, between the skin and the saphenous fascia
The interfascial system, between the saphenous fascia and the muscle fascia
Deep system: Subaponeurotic/subfascial; drains the lymph from the muscles, joints, synovial sheaths, and nerves. It runs alongside the deep blood vessels.
Communicating system: Consists of a group of lymphatic vessels that interconnect a system (deep or superficial) on the same aponeurotic stratum.
Perforating system: Interconnects the two systems (superficial and deep).
Visceral system: Drains the lymph from different organs.
Lymph Trunks
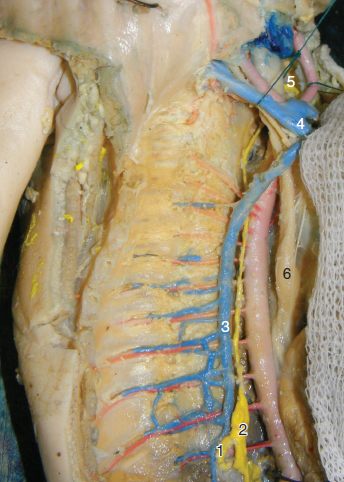
Classically and schematically, the thoracic duct is considered the main prevertebral collector that drains lymph from three body quadrants and discharges it into the left venous angle. It is formed by the union of the two lumbar trunks and the intestinal trunk, at the height of lumbar vertebrae L1 and L2 (abdominal origin) or behind the crus of the diaphragm and in front of thoracic vertebrae T11 and T12 (thoracic origin) (Fig. 6-2).
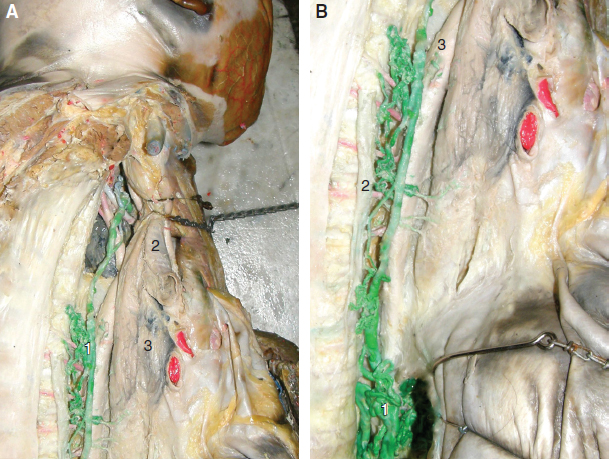
Occasionally a dilation of the origin can be observed, called the cisterna chyli. Anatomic variations are also frequently seen, such as the plexus shape in the origin and trunk (Fig. 6-3).
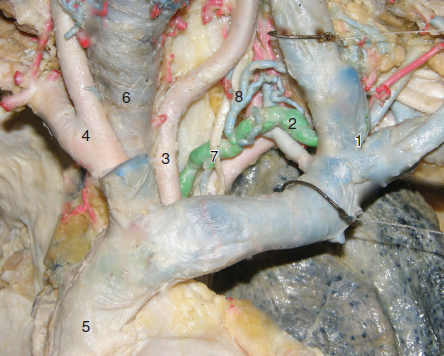
The thoracic duct ascends between the azygos vein and the aorta and is covered by the pleura and esophagus. At the level of thoracic vertebrae T4 and T5, the duct crosses under the esophagus and aortic arch and ascends toward the thoracic inlet on the left margin of the vertebral column, between the esophagus and the left subclavian artery, reaching the left jugular subclavian angle (Fig. 6-4). Our research has shown that in the left carotid region there is a lymph collector that receives the lymph from the left fascial, cervical, carotid, and temporal regions. The right duct is the one that drains the remaining upper right quadrant to the right venous angle. 3 , 4
Applied Anatomy of the Lymphatic System
LYMPHATIC DRAINAGE OF THE BREAST AREA
The predominant lymphatic drainage pathway from the breast flows toward the axilla (Fig. 6-5). Axillary node dissection is a standard surgical treatment in patients with involved axillary lymph nodes. Unfortunately, arm lymphedema develops in 7% to 77% of patients with axillary lymph node dissections. Sentinel lymph node biopsy has become a frequently used and widely accepted method for surgical staging of axillary lymph nodes in breast cancer, although the incidence of arm lymphedema after sentinel lymph node biopsy varies from 0% to 13%. 5 The reasons for this may be seen in the multiple interpretations of the term sentinel lymph node—variously identified as the first lymph node to which the tumor drains, the closest node to the tumor, or the node that is most seen with the probe (which answers only the first word of the term). Thus, under certain circumstances, when a biopsy of more than one node is performed, a minimally invasive surgery becomes a pseudoaxillary lymph node dissection procedure. 6
In our anatomic research, we divided the lymphatic drainage of the mammary gland from that of the mammary skin and found it difficult to extrapolate our research to the clinical and surgical practice (Fig. 6-6). The most representative instance was the injection method in the sentinel lymph node technique. The optimal sites of dye and/or colloid injection have not been defined: intradermic, subareolar, peritumoral, or intratumoral. There is no consensus on this topic. The problem is to consider the same lymphatic drainage of the mammary gland and the mammary skin as a unique functional unit based on the embryologic hypothesis. Under this concept, the subareolar plexus is considered the center of lymphatic drainage in the breast. This plexus was described by Sappey in 1874. Perhaps, as suggested by Turner Warwick, Sappey confused the milk ducts with lymph vessels. He emphasized the subareolar plexus considering that this technique is the mercury injection in cadaver and it dates from 1800. 7 , 8 According to this concept, the exact tumor site is not as relevant at the moment of injection, because the tumor could be located in any of the breast quadrants. However, some investigators advocate injection in the subareolar area.
The lymph produced in the mammary parenchyma goes through a perilobular lymphatic network and through the interlobular spaces that feed the lymph capillaries, which meet and lead to the secondary pedicles. These lymph vessels exit the mammary gland and make up the axillary, mediastinal, and retropectoral lymphatic pedicles. 9 – 11
Axillary Pedicle
The axillary pedicle is the largest of the three mammary lymphatic pedicles; it is formed by two to six lymphatic vessels. This pedicle may receive lymph vessels from any breast quadrant, either superficial or deep, from the nipple, areola, or the skin covering the breast. It emerges from the lateral region of the breast, following the border of the pectoralis major, passes to the base of the axilla, and then crosses the pectoroaxillary aponeurosis (Fig. 6-7).
Four pedicles secondary to the axillary pedicle can be identified:
Lateral mammary: The lateral mammary pedicle follows the path taken by the lateral mammary vessels. It is formed by two to five lymphatic vessels and joins the nodes in the lateral mammary chain. This is the first node level of the axilla.
Subscapular: The subscapular pedicle is little developed. It passes toward the posterior surface of the axilla, where the subscapular vessels lie. It consists of one or two lymphatic vessels and joins the nodes in the subscapular chain.
Superior thoracic: The superior thoracic pedicle is formed by a single lymphatic vessel that crosses the aponeurotic base of the axilla, passes toward the apex of the axilla, and then slips in front of the anterior serratus and behind the pectoral muscles, to end in the superior thoracic chain. It is the second node level of the axilla.
Axillary-vein: The axillary-vein pedicle occurs least frequently. It is so named because it passes directly into the highest part of the axillary space and lies in direct contact with the axillary vein.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


