CHAPTER 8 Impact of Genetics on Lymphangiogenesis
KEY POINTS
Primary lymphedema is the presenting symptom of numerous distinct conditions; it is genetically heterogeneous.
Several abnormalities within the genes involved in lymphangiogenesis have been reported to cause primary lymphedema.
The identification of more pathogenic genes will advance our knowledge of the etiopathogenesis of lymphatic disease. In time, this may allow the development of therapeutic interventions.
Patients presenting with unexplained lymphedema, even in adulthood, are likely to have an underlying genetically determined primary lymphatic abnormality.
It has become clear that primary lymphedema is not one disease but a clinical sign of several distinct clinical entities. Most patients presenting with lymphedema in adulthood are diagnosed with secondary lymphedema, even without a clear underlying cause. It is likely that many of these patients will have an underlying genetically determined primary lymphatic abnormality that the clinician has not considered. The identification of the molecular abnormality for each subtype of primary lymphedema is crucial, because it advances the understanding of the underlying mechanism of the disease. This knowledge will assist with the identification of new therapeutic strategies in the future.
Lymphangiogenesis is the term used to describe the growth of new lymphatic vessels. Developmental lymphangiogenesis occurs in the fetus as the lymphatic system develops. However, lymphangiogenesis may also occur postnatally (for example, in association with inflammatory disease or cancer). This chapter discusses the development of the lymphatic system. (Chapter 7 provides additional detail about the clinical consequences of abnormalities in this process.)
Martinez-Corral and Makinen 1 have schematically summarized developmental lymphangiogenesis in Fig. 8-1.

Until recently, the lymphatic system has remained largely ignored by the scientific and medical communities. An overview of the current theories and factors reported to be involved in lymphatic development is presented in this chapter. The literature is continuously updated with newly identified molecules thought to play a role 1 (see Chapter 7).
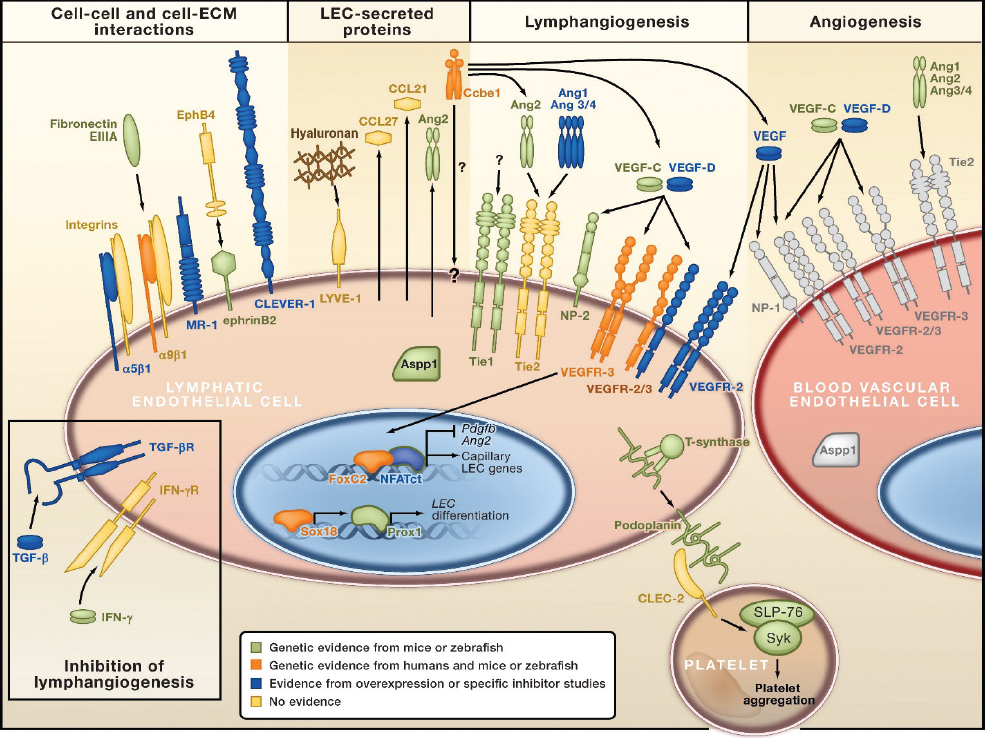
Research into lymphangiogenesis has recently identified several lymphatic endothelial cell–specific molecular markers and the genes involved in the process of lymphatic development (Fig. 8-2). Abnormalities within several of these genes are now known to cause different primary lymphedema phenotypes in both humans and animal models (see Chapter 46). However, these recent advances merely represent the “tip of the iceberg,” because there is much about lymphangiogenesis that must still be discovered.
The Origin of Lymphatic Endothelial Cells
The first lymph sacs develop in human embryos at the age of 6 to 7 weeks’ gestation, almost 1 month after the blood vasculature system begins to develop. 2 Animal model research (see Chapter 46) has demonstrated that a subpopulation of blood endothelial cells, which sprout from cardinal and peripheral veins, will differentiate into lymphatic endothelial cells (LECs). 3 Lymphatic vessel endothelial hyaluronan receptor 1 (LYVE1) is the earliest known cell marker indicating that LEC competence has been acquired. 4 The LECs will then bud off to form primitive lymphatic structures called lymph sacs. 5
The differentiation of LECs from blood vascular endothelial cells is controlled by transcription factors, such as prospero homeobox 1 (Prox1), Sox18, and COUP transcription factor 2 (COUP-TFII). Prox1 is required for the differentiation of LECs during embryogenesis and for LEC maintenance during adult life. 6 LECs that express Prox1 are then able to upregulate other lymphatic endothelial-specific molecules, such as vascular endothelial growth factor receptor 3 (VEGFR-3) and LYVE1. 7 Sox18 is expressed in the cardinal vein and regulates Prox1 expression. 8 However, the signal that induces Sox18-mediated Prox1 production has not yet been identified. COUP-TFII interacts with Prox1 and induces expression of LEC-specific genes, including Vegfr-3 and neuropilin 2 (Nrp2). 9 It also establishes LEC specification by suppressing Notch signaling. 10
Venous Sprouting of Lymphatic Endothelial Cells
In embryogenesis, individual LECs connect to each other by adherens junctions and will “sprout” into the primitive lymphatic structures, the lymph sacs. 11 Animal studies have identified that the vascular endothelial growth factor C (VEGF-C)/VEGFR-3 and collagen and calcium-binding EGF domain 1 (CCBE1) signaling pathways regulate sprouting. 12
The ligands vascular endothelial growth factor D (VEGF-C and VEGF-D) bind to and activate the tyrosine kinase receptors VEGFR-2 and VEGFR-3 and their coreceptor Nrp2 on LECs. VEGFR-3 is considered the main VEGF-C receptor for lymphangiogenesis. 1 Both VEGF-C and VEGF-D promote migration and proliferation of LECs in vitro and lymphatic vessel hyperplasia in vivo. However, only VEGF-C is needed for embryonic lymphatic development. 13 , 14 The other VEGF-C receptor, VEGFR-2, is thought to be involved in lymphangiogenesis, but this has not yet been proved. CCBE1 is expressed in tissues that are in close proximity to the budding venous-derived LECs. CCBE1 does not appear to have direct lymphangiogenic activity on its own but can enhance the lymphangiogenic effects of VEGF-C by upregulating the levels of it. 15 It was recently discovered that CCBE1 promotes proteolytic cleavage of the poorly active 29/31-kDa form of VEGF-C by the ADAMTS3 protease, resulting in the mature 21/23-kDa form of VEGF-C, which subsequently induces increased VEGF-C receptor signaling. 16
Lymphatic Sprouting
Further development of the lymphatic system occurs by lymphatic vessel sprouting from the primitive lymph sacs mentioned previously. This process is controlled by the VEGF-C ligand and its receptor VEGFR-3. NRP2, Ephrin-B2, and Notch are also required for the regulation of late embryonic and postnatal lymphatic sprouting and remodeling. 17 Notch will induce VEGFR-3 expression and thereby increase endothelial cell responsiveness to VEGF-C in early mouse embryos. 18
Remodeling of a Lymphatic Vascular System
The primitive lymphatic vessels are now required to mature into a functional vascular network with vessel-type features to serve their critical functions. Remodeling processes occur late in embryonic development and the early postnatal period. They lead to the formation of flap valves in lymphatic capillaries, the establishment of precollecting and collecting vessels by way of smooth muscle cell (SMC) recruitment, and the development of luminal valves.
Flaplike openings (called primary valves) form between the LECs of lymphatic capillaries to create button-like intercellular junctions that facilitate the entry of interstitial fluid into initial lymphatic vessels. 19 Molecular mechanisms controlling this process remain poorly understood, but vascular endothelial (VE)–cadherin is thought to promote junction stability. 19
Intraluminal valves within developing collector vessels are formed by the expression of Prox1 and forkhead box (FoxC2) transcription factors by clusters of LECs. It has been proposed that mechanical forces resulting from the flow of lymph may play a role in establishing the locations of these valves. 20 Valve-forming endothelial cells arrange themselves on the vessel wall to form a transverse ridge, which subsequently develops into mature valve leaflets. 21 FOXC2 is a significant regulator of lymphatic valve formation. FOXC2 deficiency in humans and animal models results in lymphatic vessel valve dysplasia. 22 However, it is apparent that other regulators are involved in lymphatic valve development, such as NFATC1, calcineurin, Ephrin-B2, Ang2, connexin, and integrin alpha9/fibronectin-EIIIA signaling pathways. 21
The lymphatic precollectors and collecting lymphatic vessels are covered by SMCs except in the luminal valve areas to assist with the proximal propulsion of lymph. 23 The number of perivascular SMCs increases progressively along the lymphatic vascular trunk. Several markers are involved in SMC recruitment, including plateletderived growth factor B (PDGF-B). 22
CLINICAL CONSEQUENCES OF ABNORMALITIES WITHIN THE LYMPHANGIOGENESIS PATHWAY
Until recently primary lymphedema received limited interest from both the clinical and academic communities. Until Connell et al 24 published their 2010 paper on classification, phenotyping of patients was considered of little benefit. Their paper highlighted the importance of accurate in-depth phenotyping and how it can lead to the identification of new causal genes. A revision of the classification pathway was published in 2013 25 (Fig. 8-3). It highlighted the spectrum of disorders that may present with primary lymphedema and suggested the underlying causal gene. The classification pathway was presented in the form of a color-coded algorithm to illustrate the five main categories of primary lymphedema and the individual subtypes within these categories. The main categories are as follows:
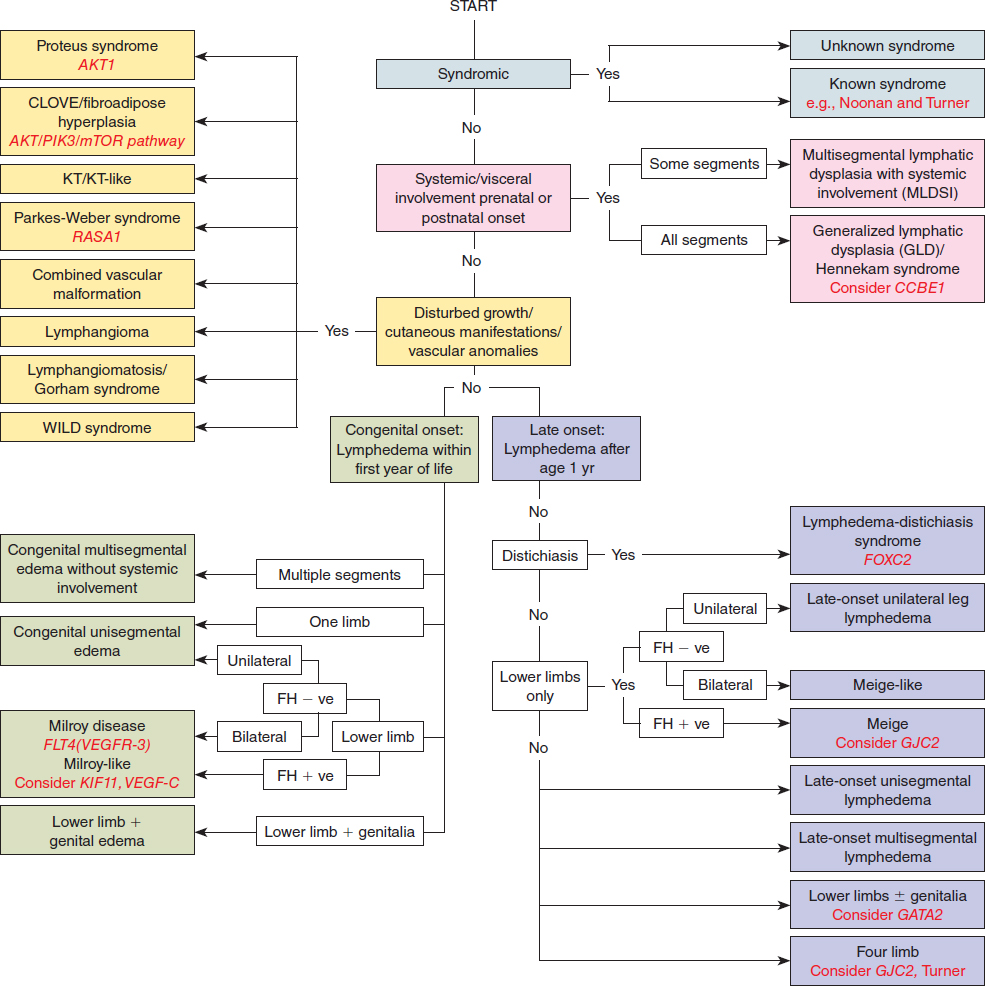
Syndromic disorders associated with lymphedema (but where lymphedema is not the predominant feature) (blue)
Localized or generalized lymphedema associated with systemic/visceral lymphatic abnormalities (pink)
Lymphedema in association with disturbed growth and/or cutaneous/vascular anomalies (yellow)
Congenital lymphedema (green)
Late-onset primary lymphedema (purple)
There will be exceptions and outliers to this classification system, but it has proved a useful clinical and research tool that is still evolving. Rigorous phenotyping in combination with recent advances in genetic analysis, such as next-generation sequencing, will enhance the identification rate of new genes that cause primary lymphedema.
Several abnormalities within genes involved in lymphangiogenesis have already been reported to cause primary lymphedema, and they will be discussed. Although we do not yet fully understand all mechanisms involved in lymphangiogenesis, the identification of mutations in VEGFR-3, VEGF-C, CCBE1, SOX18, and FOXC2 in humans with lymphatic insufficiency supports the critical role these genes play.
Mendola et al 26 recently screened 78 patients for mutations in known primary lymphedema genes and detected mutations in 36% of cases. This supports the hypothesis that other causal genes for primary lymphedema have yet to be identified. Certainly not all cases of primary lymphedema will have a monogenic cause.
Cutaneous manifestations | Nevi/pigmentation variations (for example, epidermal nevi/vascular malformations) |
Distichiasis | Presence of aberrant eyelashes arising from the meibomian glands |
Disturbed growth | Hypertrophy (overgrowth) and hypotrophy of bone or soft tissue resulting in altered length of a limb or body part |
KT/KT-like | Klippel-Trenaunay/Klippel-Trenaunay-like syndrome |
Prenatal onset | Detection of lymphatic abnormality in the prenatal period; isolated pedal edema excluded from this definition, because this may be a presentation of Milroy disease |
Segment | A region of the body affected by lymphedema (for example, the face, conjunctiva, genitalia, upper limbs, lower limbs—each constitutes one body part); multisegmental refers to more than one segment affected by lymphedema (bilateral lower limb swelling not considered multisegmental lymphedema) |
Syndromic | A constellation of abnormalities, one of which is lymphedema |
Systemic involvement | Systemic lymphatic problems persisting beyond the newborn period or manifesting at any age thereafter, including hydrops fetalis, chylous ascites, intestinal lymphangiectasia, pleural and pericardial effusions, and pulmonary lymphangiectasia |
Vascular anomalies | Includes congenital vascular abnormalities |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


