CHAPTER 5 Changing Concepts in Lymphatic Pathways
KEY POINTS
A rich avalvular lymph capillary network exists in the skin and galea of the scalp, which connects adjacent lymph territories in layers.
The number and diameter of the lymph collectors differ from person to person.
Some lymph collectors drain upward toward the mandible in the anterior neck above the platysma.
The lymphatic drainage patterns of the head and neck are diverse among individuals, and even within each side of the same individual.
Knowledge of the anatomy of the human lymphatic system and advances in imaging will help clinically when surgery of any type is anticipated as well as in follow-up scenarios for patients with lymphedema.
The lymphatic system is a vast network of tiny, colorless vessels that facilitate the removal of intracellular metabolic products from the body, provide protection from disease, and are the main route of cancer metastasis, yet remains the least described in the medical literature. Our current knowledge of the lymphatic system is mostly based on investigations that were done in the nineteenth century. However, this knowledge is often discordant with clinical experience. Further, it does not explain clinical anomalies seen with melanoma and breast cancer patients using technologic developments such as lymphoscintigraphy and sentinel node biopsy for early stage cancer treatment. Importantly, it is also well known that cancers can recur at distant sites in the absence of lymph node involvement, suggesting that disseminating cancer cells can access the circulation without traversing lymph nodes.
Lymphatic malformations, such as those that occur in primary lymphedemas, and damage or destruction of them cause many pathologic states, including lymphedema. However, with the application of improved knowledge and awareness, as described in this chapter, we may be able to anticipate improved outcomes for our patients. The main leverage point is that of imaging the lymphatic system, perhaps only at first in anticipated high-risk patients, preoperatively and perioperatively, and using that knowledge to vary the process or procedure to minimize lymphatic damage but at the same time not increasing the risk of cancer recurrence. Once this becomes an established procedure, this imaging could be employed for all patients whose lymphatics are about to be damaged (such as individuals who are about to undergo a surgical or radiologic intervention) or for those who already have a lymphatic malformation or defect.
History of Lymphatic Discovery
The accumulation of our knowledge of the lymphatic system was a gradual one, relating mainly to improvements in techniques to help visualize the delicate and mostly transparent lymphatic vessels. Originally, cadaveric dissection and observation were the major techniques. These were used for studies of the parietal and visceral tissues of the body after Aselli identified the lymphatics in a postprandial canine in 1622. 1 – 3 In the following years, the discovery of mercury as an imaging aid, by Nuck in 1692, 4 made it possible to map the lymphatics of the body. 5 – 7 However, it was Sappey 8 who published the definitive work using mercury injection to identify the fine lymphatic networks, long before the discovery of x-rays. His artistic drawings were based on studies of many subjects and resulted in the production of an overall map of the lymphatic network of the human body. Thereafter different types of injection materials, including dyes, iodine, milk, and radioactive isotopes were substituted for the toxic mercury, and it is these which formed the basic knowledge of the lymphatic system of the body. 3 , 9 – 11 However, in many ways this was still inadequate; our knowledge of the lymphatic system needed to be updated to explain some of the unexpected findings frequently seen clinically. 12 – 14
In the past decade a series of lymphatic studies in human cadavers have been published by using a new technique with radiopaque materials as the injection medium. 15 – 28 These results might help to clarify some unexpected findings in the clinic. Recent clinical experience in melanoma and breast cancer and the most recent cadaveric results have led to a fundamental reevaluation of the “classic” theory, since the drainage varies from the traditional predictions of Sappey and others in many cases. 12 , 13
Therefore a more precise and eventually an individualized map of the anatomic details of the lymphatic pathways of the human body, especially in the head and neck, can form an important basis for improved clinical management of trauma, infection, lymphedema, and cancer.
In the past decade we studied a total of 62 specimens harvested from 27 unembalmed cadavers (12 male and 15 female cadavers), aged between 69 and 98 years (average 86 years). 16 – 28 The investigation commenced at the distal end of each specimen; 0.5 ml of 6% hydrogen peroxide mixed with blue drawing ink (ratio 20:1), or 6% hydrogen peroxide only, was injected into the dermis. The epidermis and dermis were incised carefully and gently under a surgical microscope. The distended lymphatic vessel was identified in the subcutaneous tissue. A 30-gauge needle was then inserted into the vessel, and a radiopaque mixture (lead oxide or barium sulphate, milk powder, and water) was injected into the vessel. If the caliber of the vessel was smaller than 0.2 mm, a glass needle (premade using thinwalled G-100 glass tubes and the Puller PP-830) was used for injection. The specimen was radiographed using a Fuji FCR IP Cassette and a Fuji Computed Radiography Processor to locate the proximal extent of the injection for further cannulation and injection. All vessels were traced, photographed, and radiographed to demonstrate the lymphatic routes from the distal side to the proximal lymph nodes. 16 – 28
Head and Neck
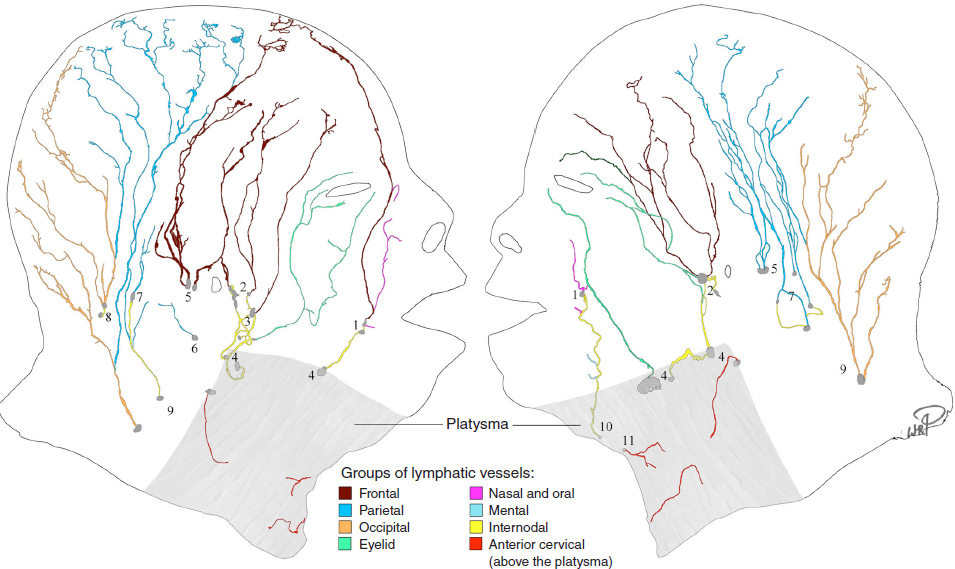
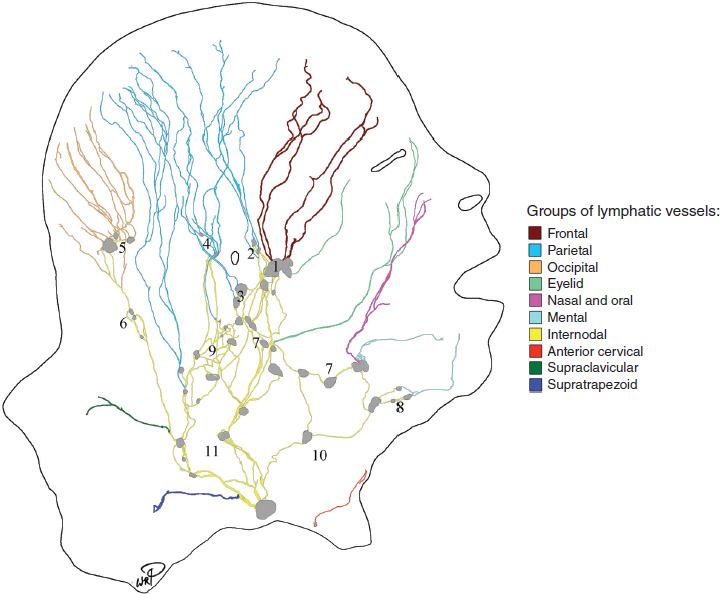
The drainage patterns of the head and neck were found to be different in individual specimens and even asymmetrical between the sides of the same body. The lymph-collecting vessels are dense in the scalp and lateral neck but sparse in the face and anterior and posterior neck areas. Imaging revealed a complete lymphatic map of the integument of the head and neck.
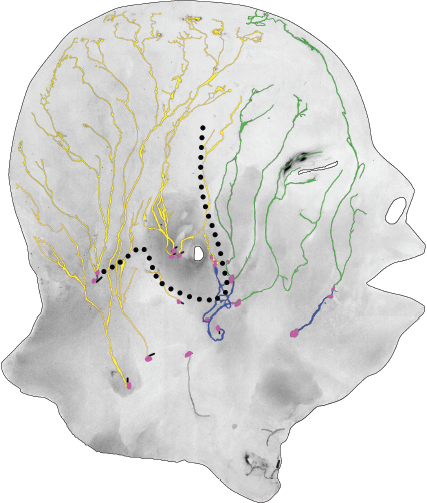
The key outcome of these new observations is that the major lymphatic vessels may drain to different lymph nodes, even if they come from the same group. For example, the lymphatics of the parietal region may drain into preauricular, retroauricular, infraauricular, or even internal jugular lymph nodes. Therefore some lymph nodes could be firsttier nodes for one group of vessels but second-, third-, or even fourth-tier nodes for the other vessels. Furthermore, two layers of lymphatic vessels were found in the anterior superficial neck. Importantly, vessels in the head and neck did not always enter the closest lymph nodes but sometimes bypassed them (Figs. 5-1 and 5-2).
Lymphatic vessels in the superficial tissue of the head and neck are distributed through the scalp (between the anterior hairline and occipital hairline), the face (between the anterior hairline and the inferior board of the mandible), and the neck (below the inferior board of the mandible and occipital hairline) regions.
SCALP REGION
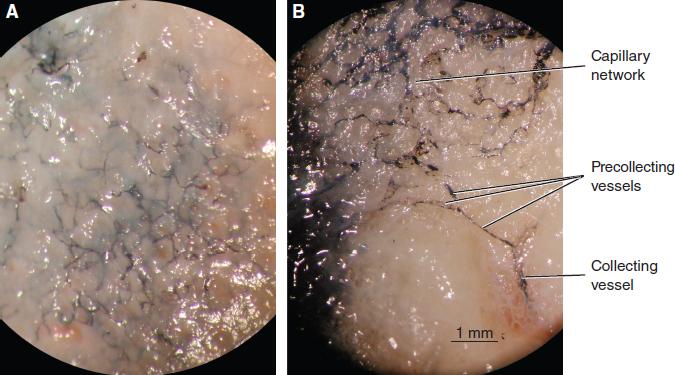
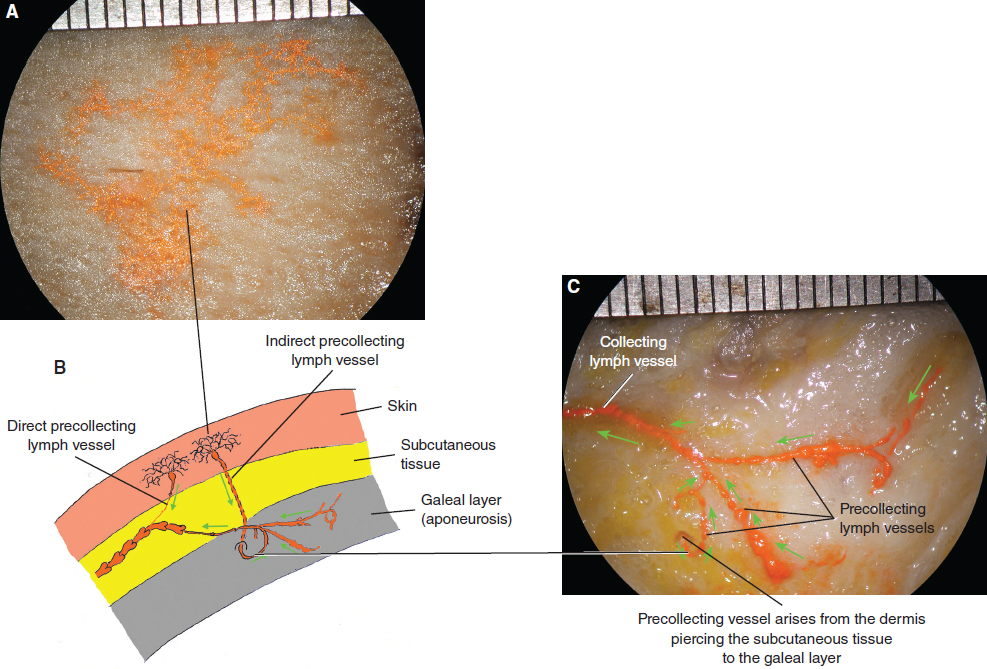
Our findings in the scalp showed rich avalvular lymph capillaries originating from both the dermis and the galeal layers (Fig. 5-3), where they converged to precollectors and directly drained to the collector. An alternative presentation occurred in which precollectors arose from the lymph capillaries of the dermis, crossed the subcutaneous tissue, and passed other collectors to join a precollector network in the galeal layer. Thus these were named indirect precollectors or bridge precollectors (Figs. 5-4 and 5-5).
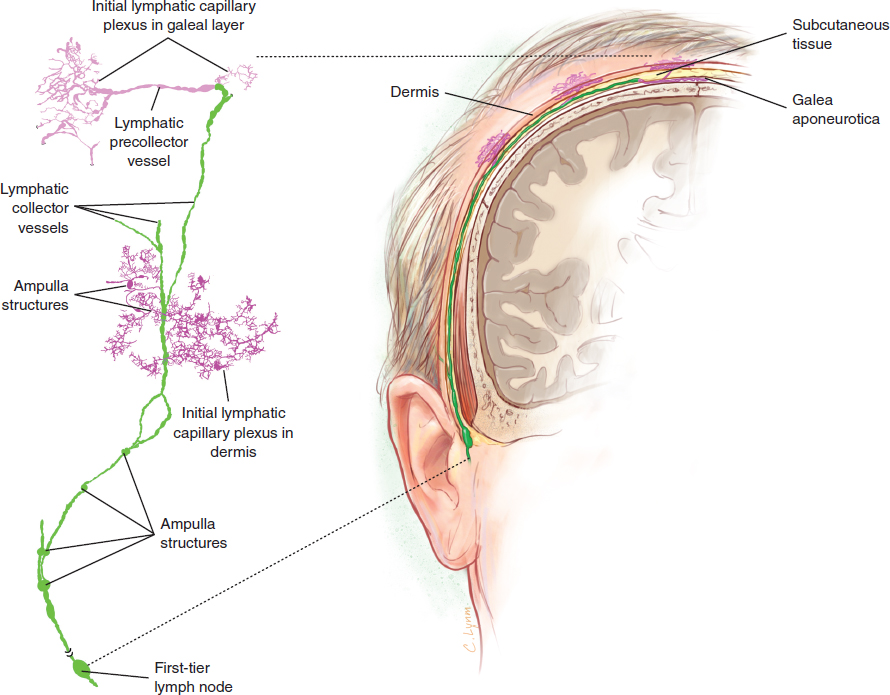
Measuring an average of 0.25 mm, the collecting lymphatic vessels are dense in the scalp region and run obliquely down to reach their firsttier lymph nodes (Figs. 5-4 and 5-6). Vessels diverged and converged along their course, like the branches of a river. Sometimes they crossed over each other and/or anastomosed with neighboring vessels. During their course, lymph collectors ran caudally in the deep aspect of the subcutaneous tissue, receiving precollectors on the way, and then drained toward their firsttier lymph nodes. The scalp lymphatic vessels include the frontal, parietal, and occipital groups, which are described next.
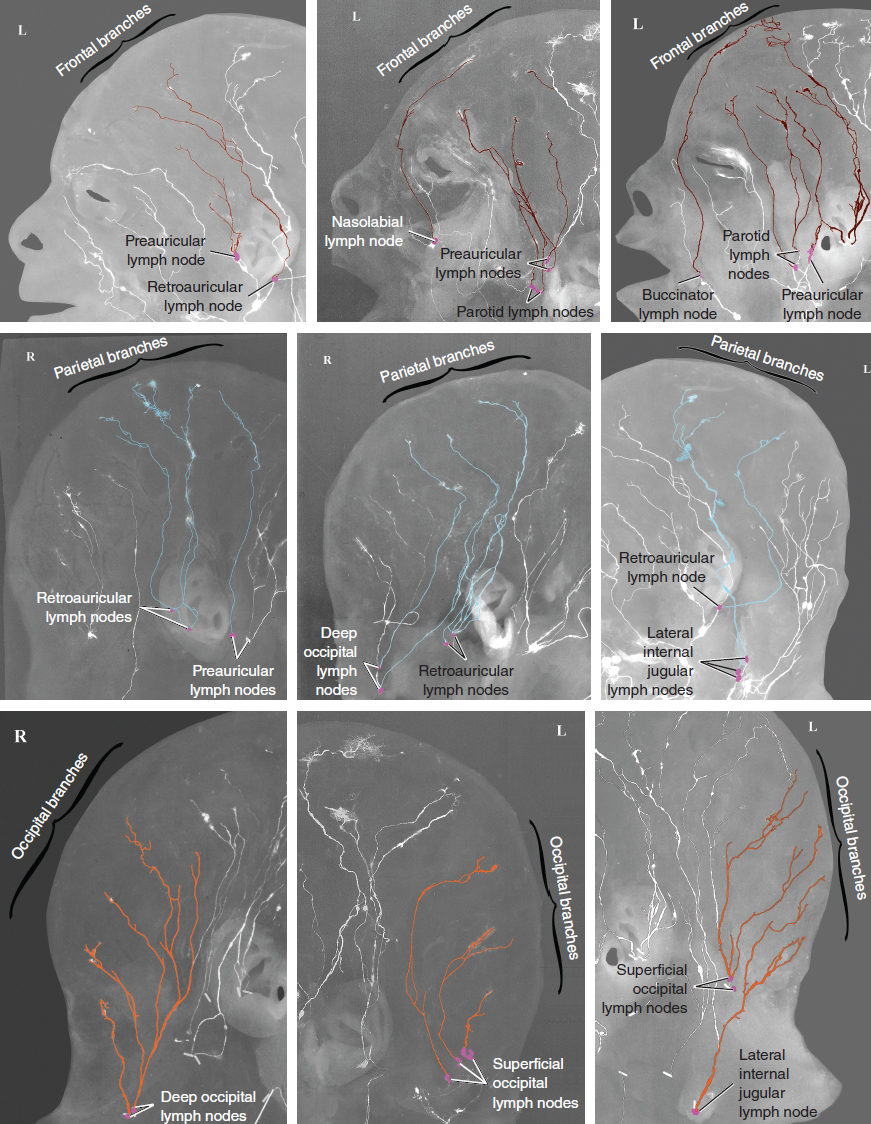
Frontal Group Here, an average of 4 branches (range 3 to 6) of frontal collecting lymph vessels were found. These vessels course radially toward their firsttier lymph nodes in the deep aspect of the subcutaneous tissue between the superior verge of the eyebrow and the coronal suture. They drained to one or multiple lymph nodes in the preauricular, retroauricular, and deep parotid groups. Occasionally one vessel, arising from the midfrontal region, traveled anteriorly and passed over the forehead, inner canthus, and root of the nose before draining to either the nasolabial or buccinator lymph nodes.
Parietal Group Here an average of 6 branches (but with a wide range of 4 to 12) of parietal collecting lymph vessels were found in each specimen. These vessels traveled radially in the deep aspect of the subcutaneous tissue between the coronal suture and the lambdoid suture. They did not only drain to the retroauricular but also the preauricular lymph nodes, sometimes even the occipital and jugular lymph nodes.
Occipital Group Here an average of 6 (range 4 to 9) occipital collecting lymphatic vessels were found. Vessels traveled radially in the subcutaneous tissue between the lambdoid suture and the posterior hairline. They drained into the superficial, deep occipital, or jugular lymph nodes.
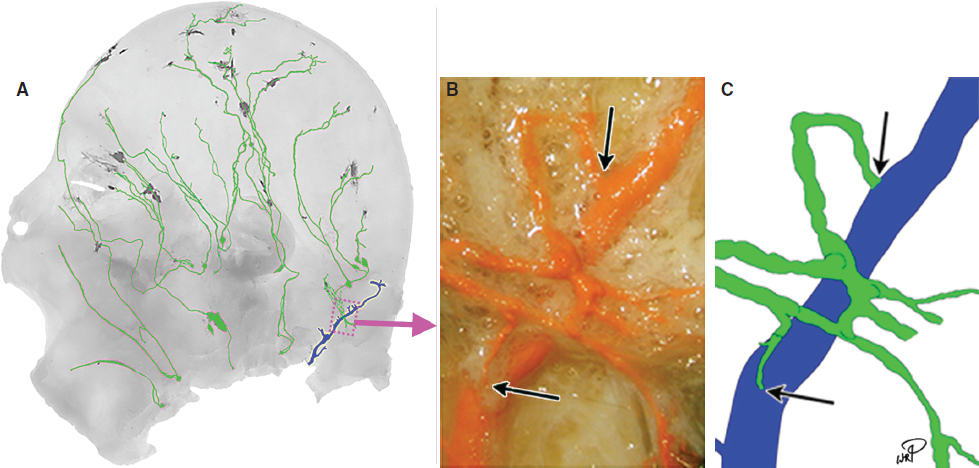
Lymphaticovenous Shunt One lymphaticovenous shunt was found in the occipital region. The efferent lymph vessels of the superficial occipital lymph nodes formed a lymphatic network. From the network two vessels emerged to communicate with a superficial occipital vein in the subcutaneous tissues (Fig. 5-7). This confirmed the clinical findings described by Wallace et al. 29
FACIAL REGION
Lymphatic vessels in the face were sparse. An average of 4 branches (range 3 to 5) was identified. The average diameter of vessels was 0.3 mm when distended with injectant, but this could be partly artifactual as a result of the vessels being abnormally stretched. Vessels traveled radially from medial to lateral in the deep aspect of the subcutaneous tissue between the eyebrow and the inferior border of the mandible toward their firsttier lymph nodes. Four groups of vessels are described according to their origin (Fig. 5-8): the eyelid group, nasal group, oral group, and mental group.
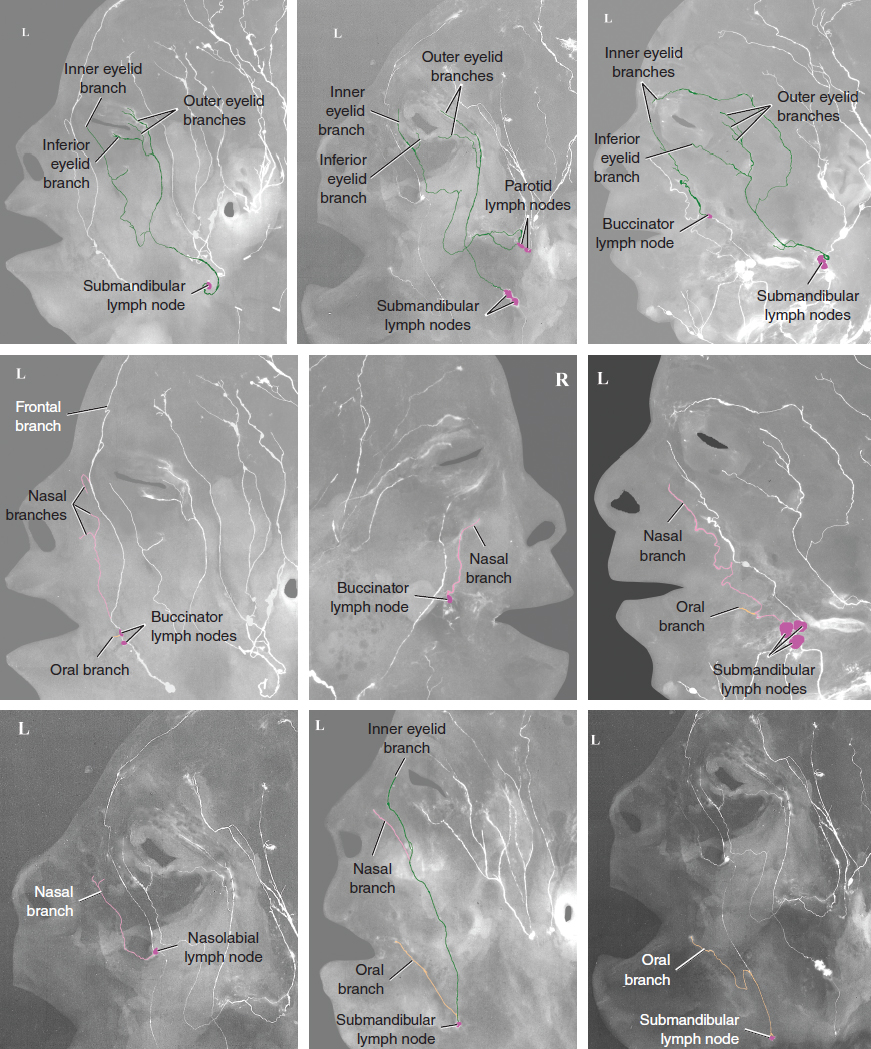
Eyelid Group The initial lymphatic capillaries arose in the upper and lower eyelids (Fig. 5-9).
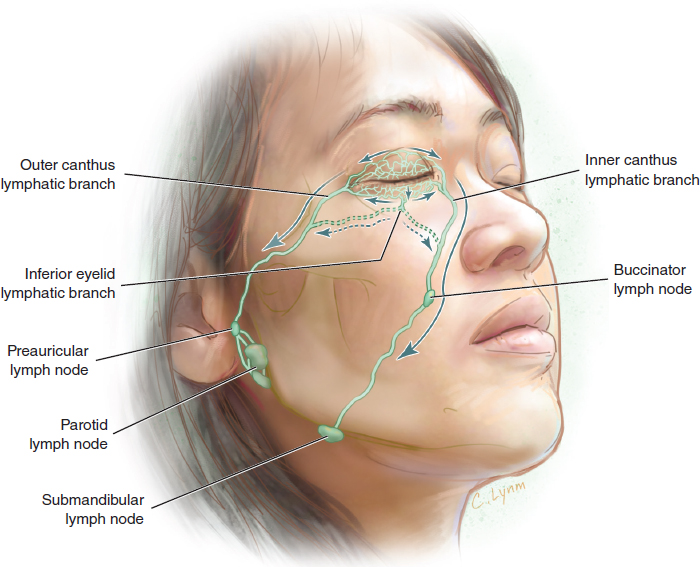
Outer Canthus Branch At the outer canthus of the eyelid, one to three lymph-collecting vessels were identified that then merged into a main collector that ran obliquely in the subcutaneous tissue and drained to the submandibular, or parotid lymph nodes.
Inner Canthus Branch At the inner canthus of the eyelid a collector, formed by the initial lymphatic capillaries arising in the upper and lower eyelids, ran obliquely in the subcutaneous tissue and drained to the submandibular, parotid, or buccinator lymph nodes.
Inferior Eyelid Branch One vessel, arising from the middle-inferior aspect of the lower eyelid, ran obliquely down in the subcutaneous tissue. It merged either with the outer or inner canthus branches and drained to the submandibular or deep parotid lymph nodes.
Occasionally an upper-inner canthus branch ran horizontally and laterally above the superior verge of the eyebrow and passed obliquely downward and posteriorly at the lateral edge of the eyebrow. Then it passed over the zygomatic process and descended anteriorly to converge with the main branch of the outer canthus draining to the submandibular lymph node.
Nasal Group The lymph vessel arising on the lateral side of the external nose traveled obliquely down from the median to the lateral side in the subcutaneous tissue of the cheek and drained into the nasolabial, buccinator, or submandibular lymph nodes.
Oral Group The initial lymphatic vessels arising in the perilabial tissue formed one or two collecting vessels near the corner of the mouth and drained to the buccinator, submandibular, or submental lymph nodes.
Mental Group The mental vessels ran in the deep aspect of the subcutaneous tissue and drained to the submental or submandibular lymph nodes (Fig. 5-10).
CERVICAL REGION
These vessels included the anterior, lateral, and posterior groups; these are discussed next.
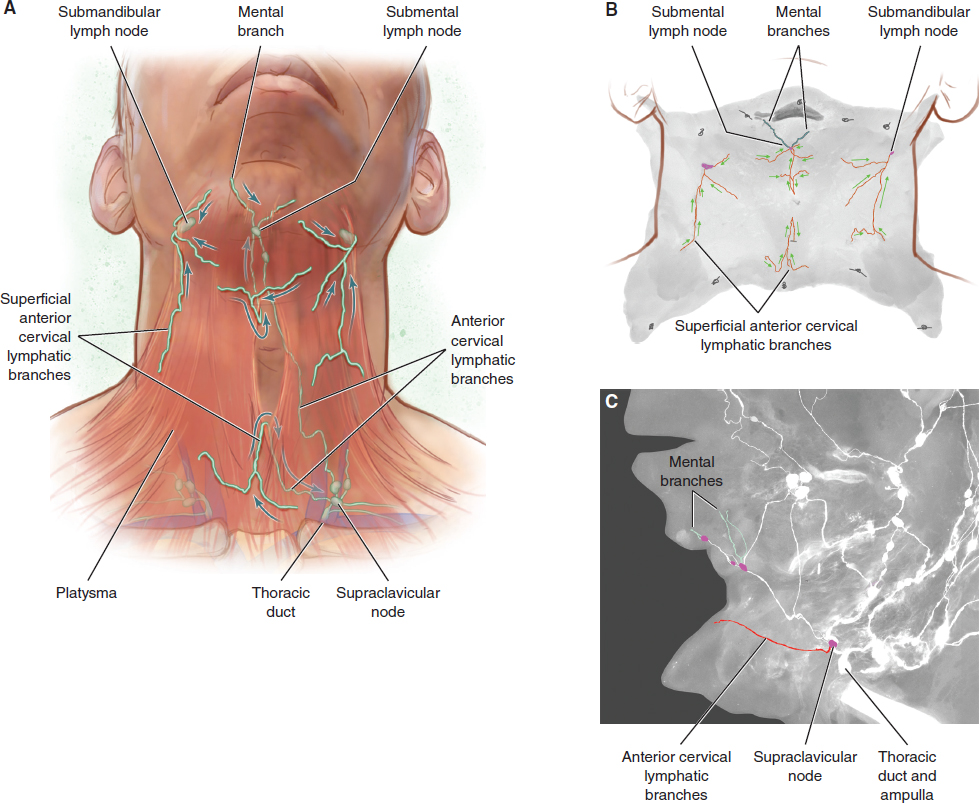
Anterior Cervical Group
Two layers of lymphatic vessels were found in the anterior superficial neck. Above the platysma vessels traveled upward, horizontally, or obliquely. The diameter of these vessels was small, 0.1 mm to 0.2 mm. Medially, they pierced the platysma near the midline, draining into the submental lymph node between the inferior border of the mandible and the laryngeal prominence and into the supraclavicular lymph nodes between the laryngeal prominence and jugular notch. Laterally, they turned over the lateral border of the platysma and drained to the submandibular lymph nodes. The vessels below the platysma were seen running above the deep fascia. They drained to the anterior jugular lymph node and/or supraclavicular lymph node.
Lateral Cervical Group
The vessels in the lateral cervical area were numerous and complex, located in the region between the inferior ear and root of the neck and running in different directions and in different layers: the subcutaneous (superficial), intermuscular (middle), and perivascular (deep) layers. Most of these vessels were situated between lymph nodes and are called the internodal lymph-collecting vessels (Fig. 5-11).
Posterior Group
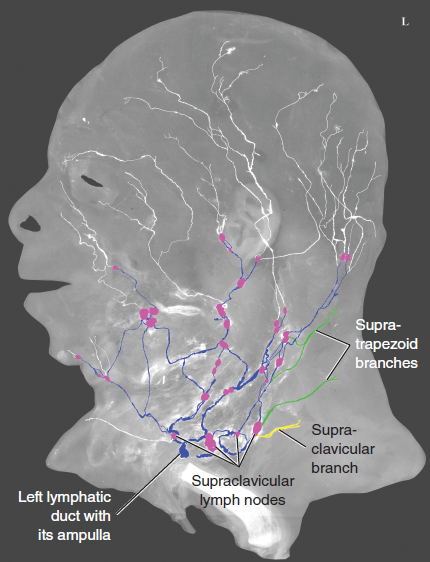
The vessels of the posterior group included the supraclavicular and supratrapezoid branches.
Supraclavicular Branch The diameter of these vessels was approximately 1 mm at least when distended with the injectant. The vessels ran anteromedially in the deep aspect of the subcutaneous tissue in the root of the neck, draining to the lateral internal jugular and/or supraclavicular lymph nodes.
Supratrapezoid Branch The diameter of these vessels also averaged 1 mm. They ran anteromedially in the deep aspect of the subcutaneous tissue in the root of the neck, draining to the supraclavicular lymph nodes.
EXTERNAL EAR
Four groups of lymph-collecting vessels were found in the external ear: the anterior, superior, middle, and inferior (lobule) branches (Figs. 5-12 and 5-13).
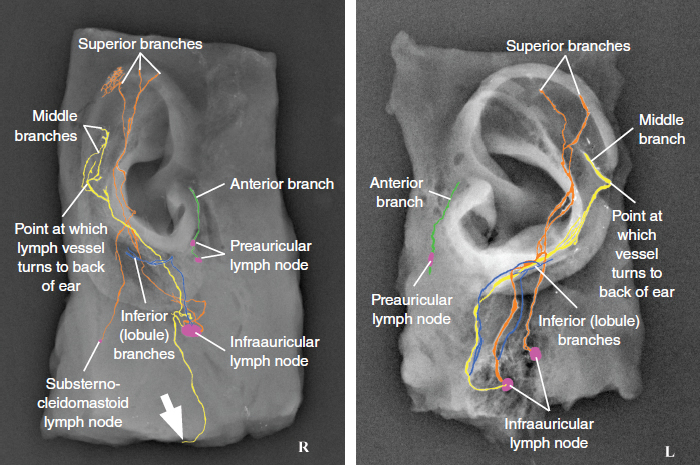
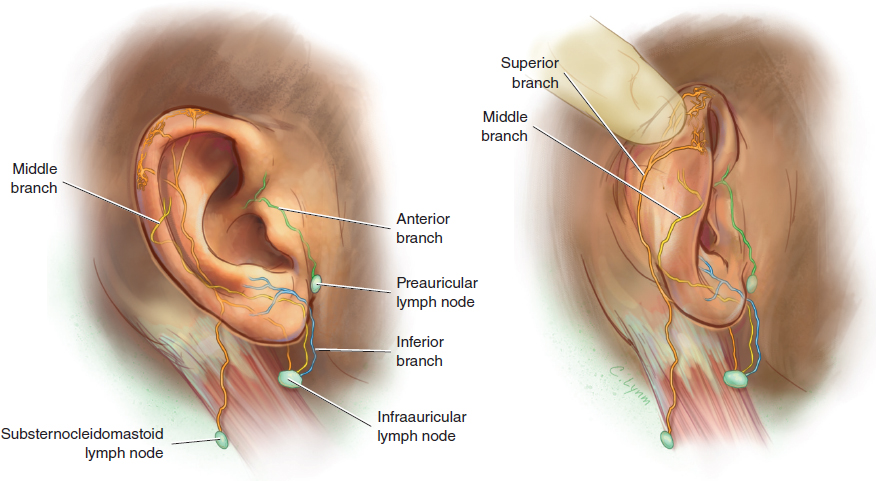
Anterior Group The initial lymphatic capillary network was distributed over most of the anterior aspect of the external ear. Medially, they converged to become one lymph-collecting vessel running under the skin of the crus of the helix and draining directly or indirectly (having merged with a vessel descending from the scalp) into the preauricular lymph node (see the green vessels in Figs. 5-12 and 5-13).
Superior Group Lymphatic vessels (here collectors are meant), arising in the superior part of the helix, traveled in the subcutaneous tissue of the back of the ear and merged together and then ran in the subcutaneous tissue of the upper lateral neck (sometimes they divided into branches) to reach the infraauricular and/or substernocleidomastoid lymph nodes (see the orange vessels in Figs. 5-12 and 5-13).
Middle Group These lymphatic vessels (here collectors are meant) arose from the scaphoid fossa near the auricular tubercle. They traveled down and passed over the cartilage at the middle of the rim and then ran obliquely in the subcutaneous tissue of the back of the ear. Continuing their course in the subcutaneous tissue of the upper lateral neck, they entered the infraauricular lymph node (see the yellow vessels in Figs. 5-12 and 5-13). Occasionally the vessel was divided before entering the infraauricular lymph node. One branch entered the node, and the other one bypassed the node and continued its course (see the large white arrow in Fig. 5-12).
Inferior (Lobule) Group Lymphatic vessels (here collectors are meant) arose in the lobule of the auricle, converged and ran obliquely down to reach the infraauricular lymph node (see the blue vessels in Figs. 5-12 and 5-13). Occasionally the vessel divided into two branches before entering the infraauricular lymph node. One entered the node while the other bypassed the node, continuing its course.
CLINICAL APPLICATIONS OF THE ANATOMY OF THE HEAD AND NECK
Rhytidectomy
The postoperative incidence of prolonged edema following rhytidectomy procedures is very low but remains a frustrating complication for the surgeon and patient alike. Baker et al, 30 after reviewing 1500 cases, reported that five patients had prolonged edema following rhytidectomy but did not mention any possible links between the lymphatic drainage and prolonged edema. 31 Guy et al 32 stated that postoperative persistent edema associated with rhytidectomy was unusual and presumably was related to lymphatic stasis, but they did not provide further discussion, and details of the lymphatic anatomy in this region were inadequate. Because the lymphatic drainage patterns of the superficial tissue in the head, face, and neck are different in each individual, the incision of the rhytidectomy might cross lymph-collecting vessels that gather in the preauricular area in some cases (Fig. 5-14) and cross those located in the subcutaneous tissue of the dissection area. Overdissection in this region might disrupt the major lymphatic vessels and result in the frustrating complication of edema.
Lymphedema of the eyelid is an uncommon condition that presents in many cases as a chronic form related to acne, rosacea, irradiation, and ocular surgery. 33 It has been mentioned that the degree of swelling is usually related to surgical factors such as excessive cauterization, extensive tissue manipulation or excision, and dissection in the lateral canthal area resulting in lymphatic interruption. 34 Fig. 5-9 demonstrates that the avalvular initial lymphatic capillaries arose in the upper and lower eyelids where the lymph could flow to the outer-inner canthus or inferior branches. If one of those branches was damaged or blocked, the others could still perform the function. It is likely that severe edema would occur if all branches were damaged by a severe injury of the periocular soft tissue or by multiple surgical incisions on the eyelid. 35
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


