Chapter 5 Anesthetic Block
Introduction
An anesthetic block consists of injecting anesthetic solution into the main trunk of the nerve, or around it, in order to relieve pain in its area of sensory distribution. One of the advantages of these blocks is that a single, precisely positioned injection can relieve large areas of sensitivity without distorting the tissue at the site of injection. As many nerves are accompanied by their corresponding veins and arteries, prior aspiration is essential in order to reduce the risk of an intravascular injection. 1 ,. 2
Anatomical Structure of the Facial Foramens
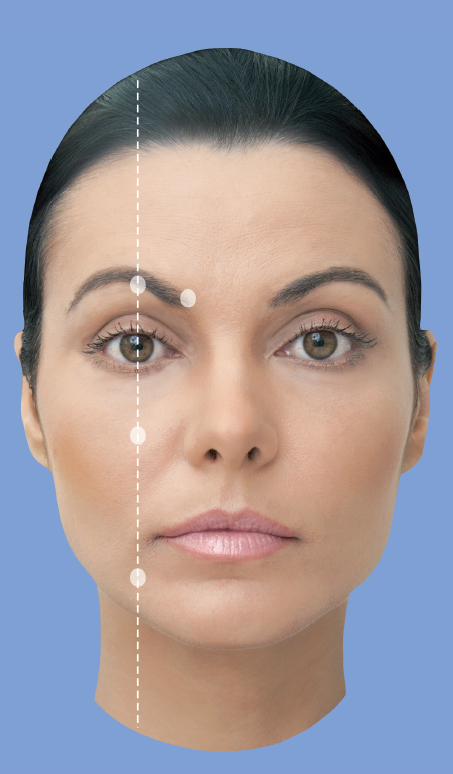
A successful anesthetic block depends largely on the injector’s knowledge of the position of the nerve foramens. The injector takes advantage of the alignment of the main facial foramens, which are distributed along the pupillary midline, when the eye is in a normal position and looking forward naturally (Fig. 5.1 and5.2).
Supraorbital Nerve
The supraorbital nerve exits the foramen in the upper ridge of the orbit, approximately 27 mm laterally from the midline of the glabella. This foramen can be easily palpated in the majority of patients. After exiting the foramen, the nerve crosses the corrugator muscles and divides into the medial and lateral portions (Fig. 5.3–5.6). 1 ,. 3
Supratrochlear Nerve
The supratrochlear nerve exits from a notch or foramen, approximately 17 mm from the midline of the glabella, and innervates the medial portion of the forehead. The infratrochlear nerve exits from a foramen below the trochlea and supplies the medial upper eyelid, medial commissure, skin of the bridge of the nose, conjunctiva, and lacrimal sac. When injecting into this area, the injector should always use the noninjecting hand to palpate the orbital rim, ensuring that the needle tip is above the bone ridge of the orbit. The infratrochlear nerve is blocked by the injection of anesthetic into the junction between the orbit and the nasal bones (Fig. 5.7–5.9).
Infraorbital Nerve
The infraorbital nerve exits the infraorbital foramen (IOF) about 5 to 10 mm below the inferior orbital rim, in an imaginary line traced from the midpupil. Anesthetized areas include the side of the nose, lower eyelid, and upper margin of the injected lip. This nerve can be blocked intra- or extraorally. The intraoral approach involves applying anesthetic gel to the oral mucosa along the vestibular groove, then below the canine fossa (between the canine tooth and the first premolar) and waiting for a few minutes. Then the upper lip is lifted, and the needle is inserted into the groove, pointing up toward the IOF. The infraorbital nerve can also be easily blocked using the facial transcutaneous method, which can be the preferred route for patients with “dental phobia.” The needle is inserted into the skin in the direction of the foramen, but care must be taken to avoid the superficial vessels, which can cause ecchymosis (Fig. 5.10–5.14).
Mental Nerve
The mental nerve (MN) exits the mental foramen (MF) at the base of the root of the second premolar (many patients might not have premolar due to orthodontic extractions). The MF is located, on average, 11 mm from the gumline. Alternatively, the MN can be blocked through the skin of the face by aiming the needle at the same point. The anesthetized area will be the unilateral lower lip up to the midline and laterally up to the mentolabial sulcus (Fig. 5.15–5.19).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


