The glabellar angle (maximum prominence of the glabella in relation to the frontonasal suture) reduces during the aging process, in both sexes, and bone remodeling starts at this location.1Moreover, there is local fat loss, which is worsened by the thinning of the skin and repetitive muscular movements. Deep filler injections in this region are used to lift the eyebrow medially and the base of the nose, and can be combined with botulinum toxin and superficial filler injections to alleviate the horizontal and vertical lines caused by the contraction of the procerus and corrugator muscles, respectively.
Anatomy
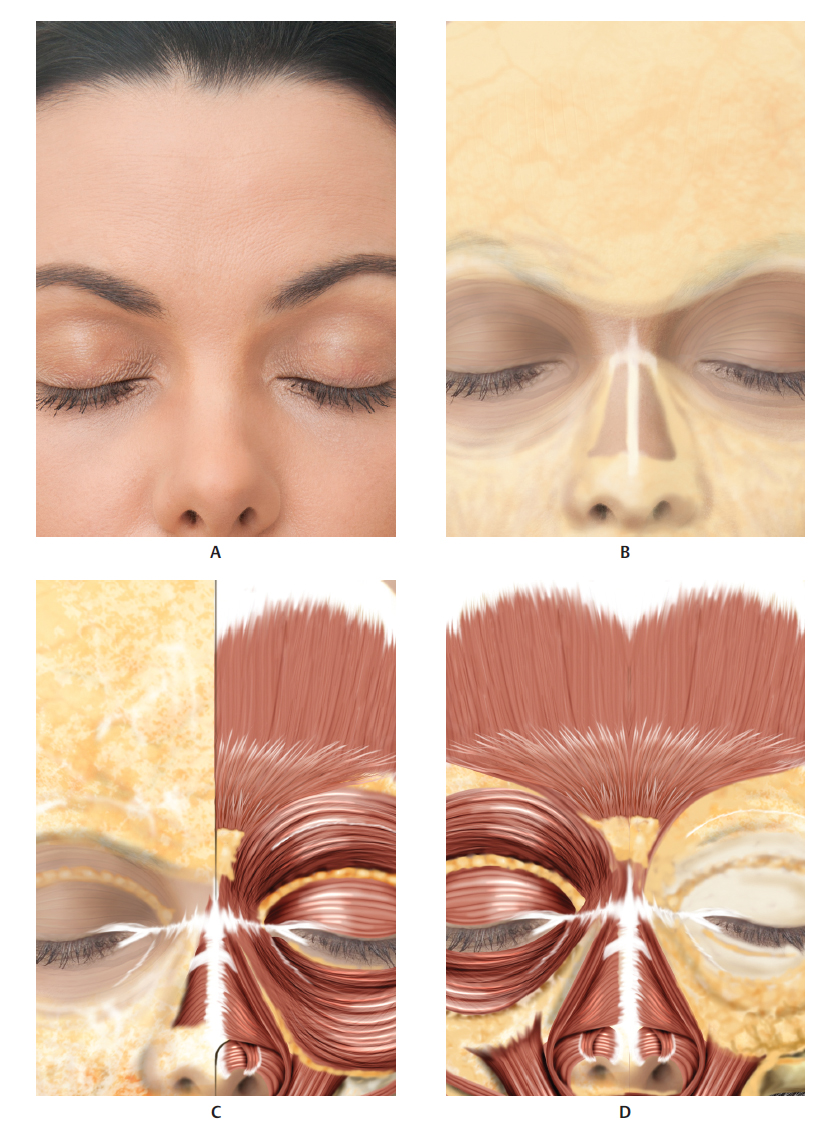
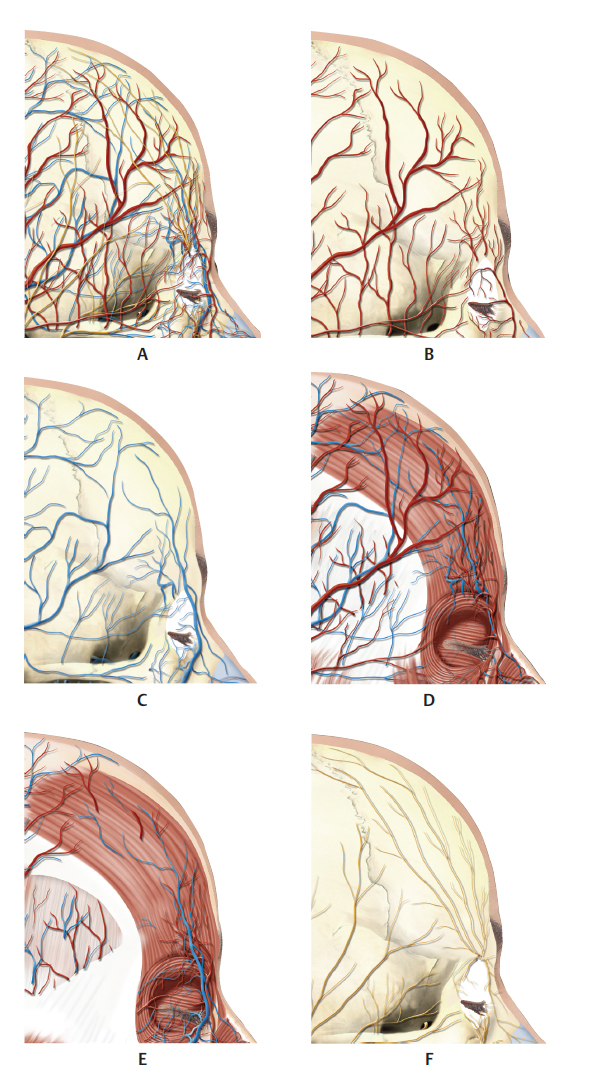
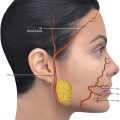
The central fat pad of the forehead lies below the skin and above the procerus muscle; it is delimited laterally by the middle fat pads and inferiorly by the nasal dorsum.2The supratrochlear nerve, vein, and artery leave the superomedial region of the orbit approximately 17 to 22 mm laterally to the midline, anastomosing with the supraorbital artery and the frontal branch of the superficial temporal artery (Fig. 9.1–9.7).
Intradermal Technique
An intradermal micro bolus is used for superficial wrinkles that persist after application of botulinum toxin in the corrugator muscle (Fig. 9.8,9.10, and9.11).
Supraperiosteal Technique
The following steps should be followed for this procedure (Fig. 9.9–9.16):
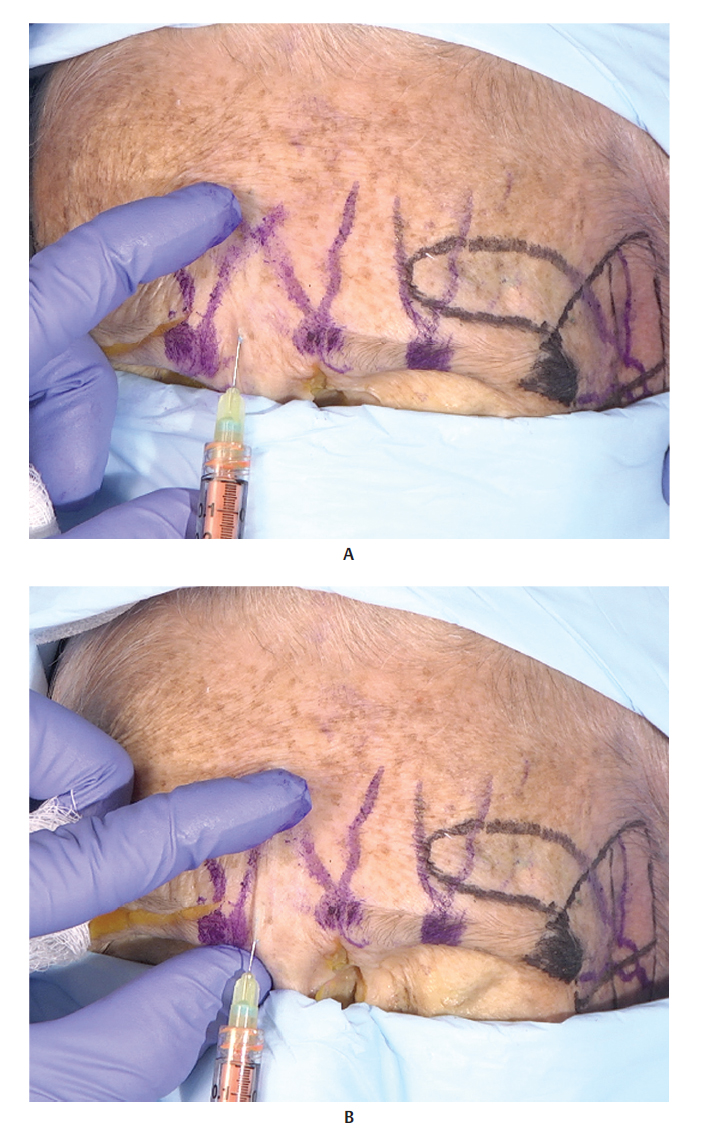
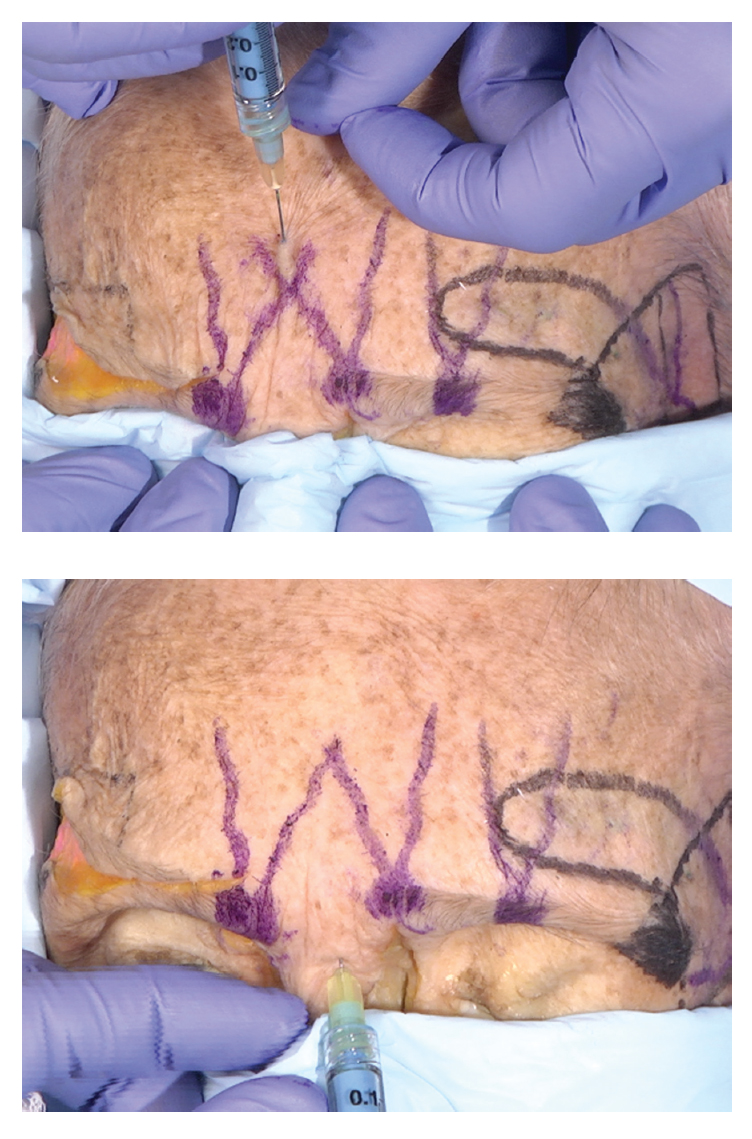
Mark the area to be filled.
Next, inject hyaluronic acid (HA) or volumizer through the entry point of the 25 Gx 50 mm microcannula in the supraperiosteal plane and massage the area. Carruthers and Carruthers3described the deep injection technique with a 27 G needle.
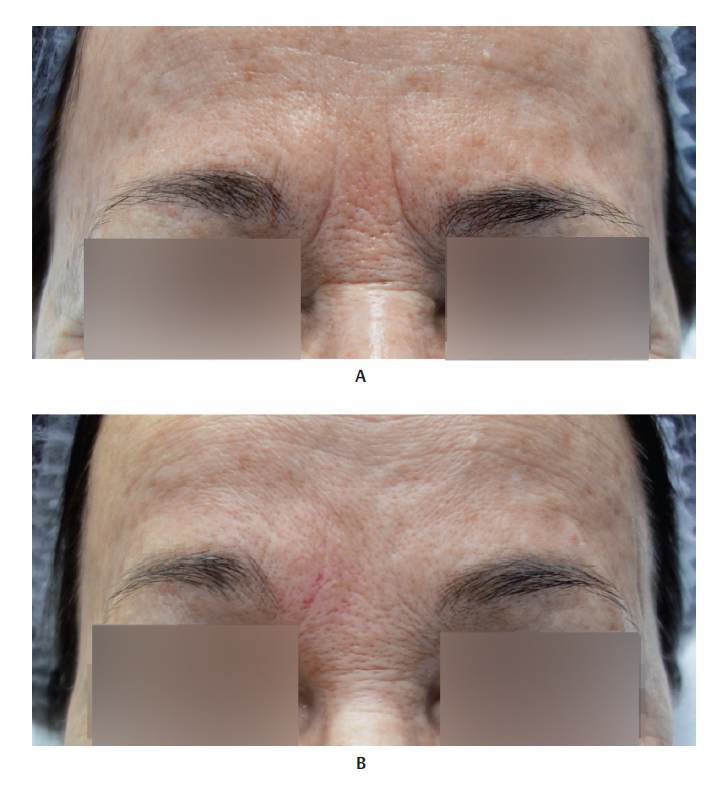
Fig. 9.17 shows a patient before and after the filler injection.
Complications
Sensitivity and slight local edema are to be expected. Asymmetries can be corrected by massaging the area, or by applying additional injections of HA or hyaluronidase. Onset of ischemia is possible due to external compression of the local vessels; therefore, large volumes of HA should be avoided. Accidental intravascular injection can cause embolism and obstruction of the central retinal artery.
References
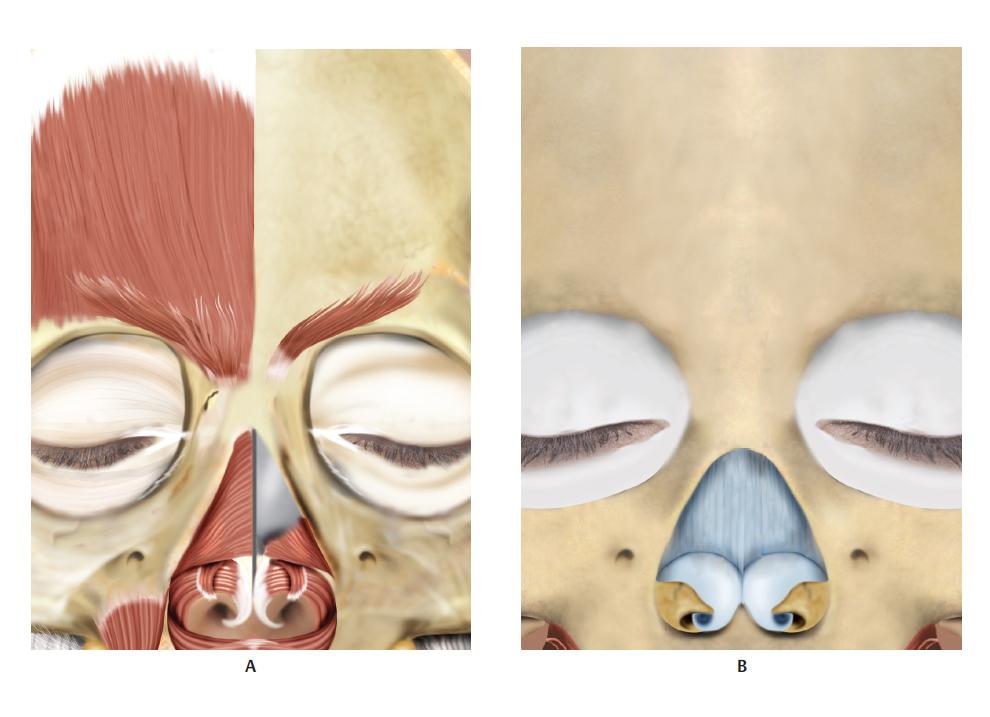
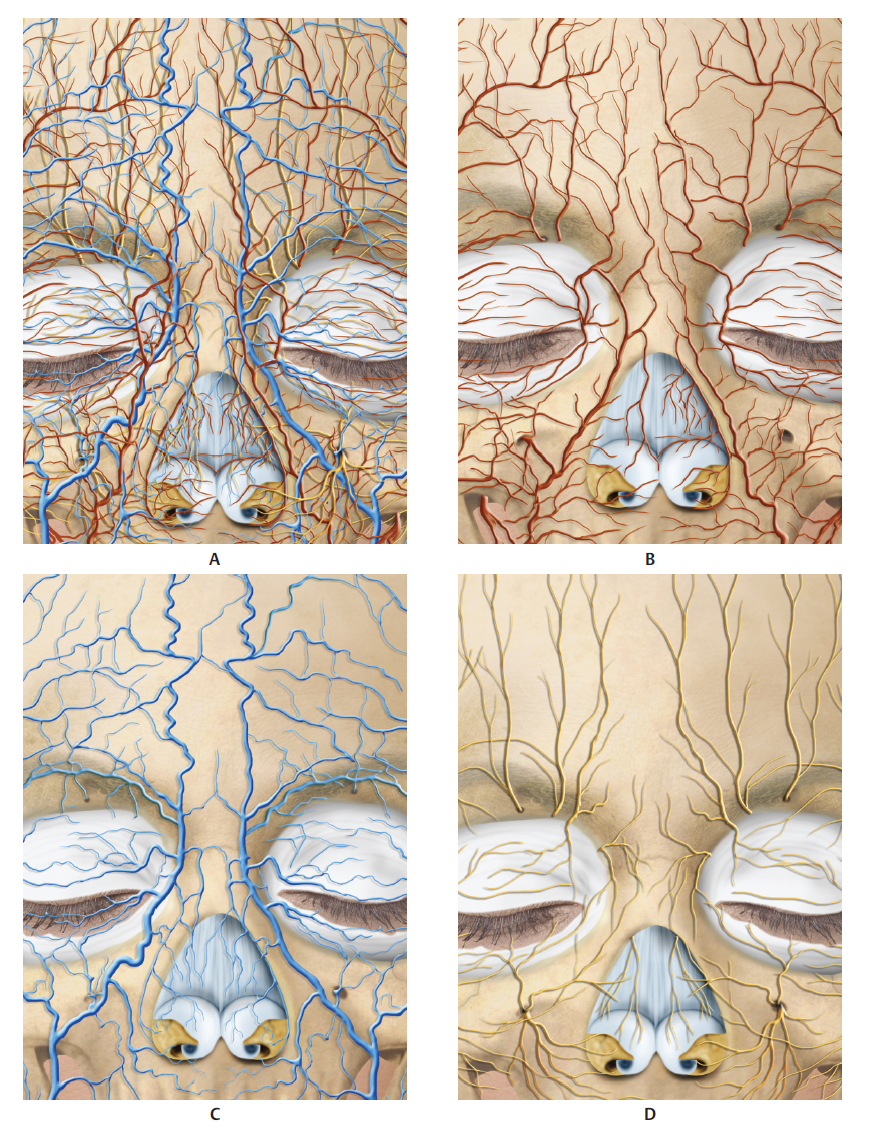
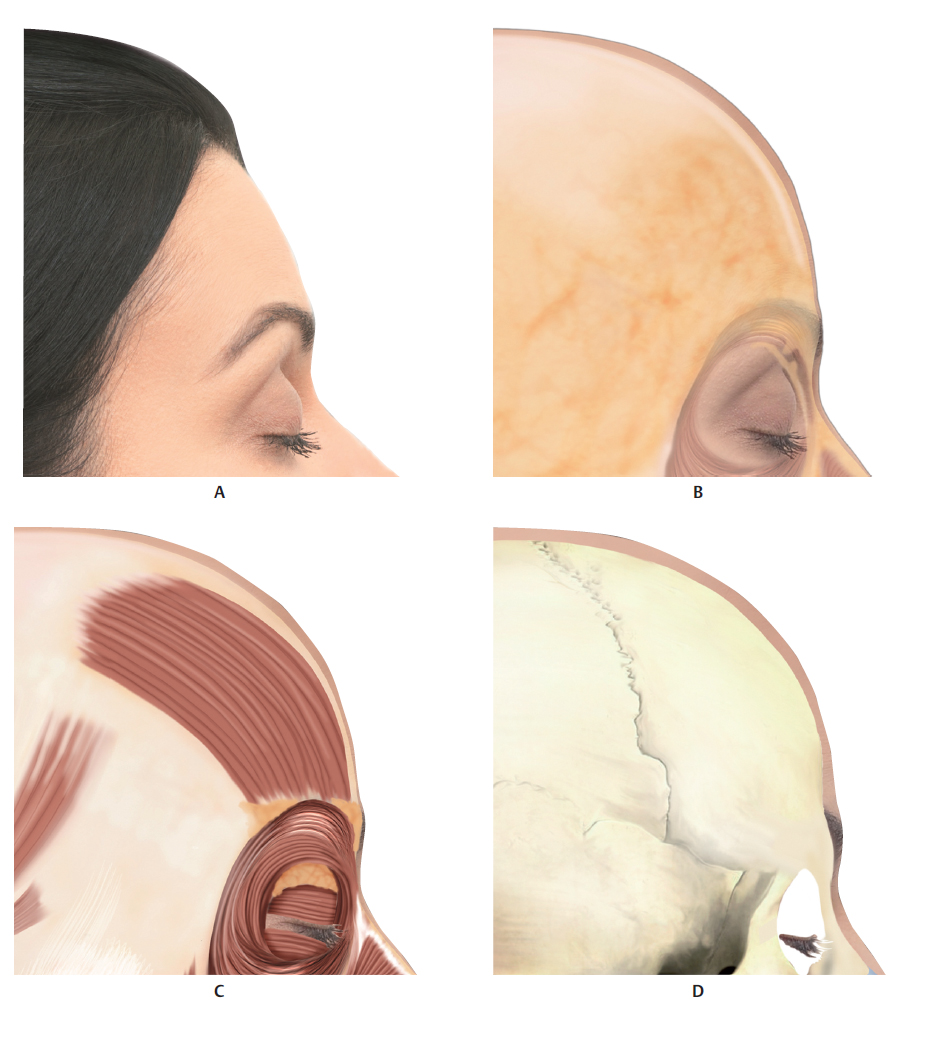
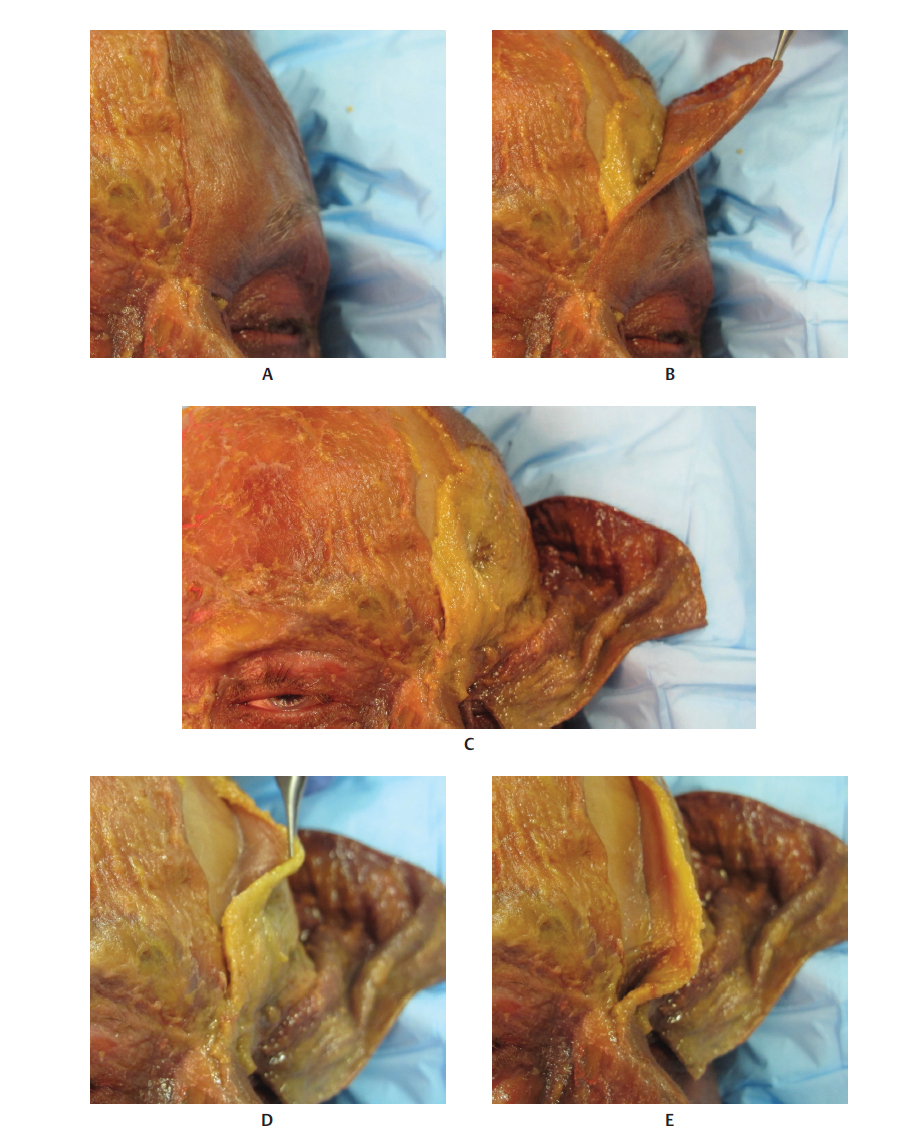
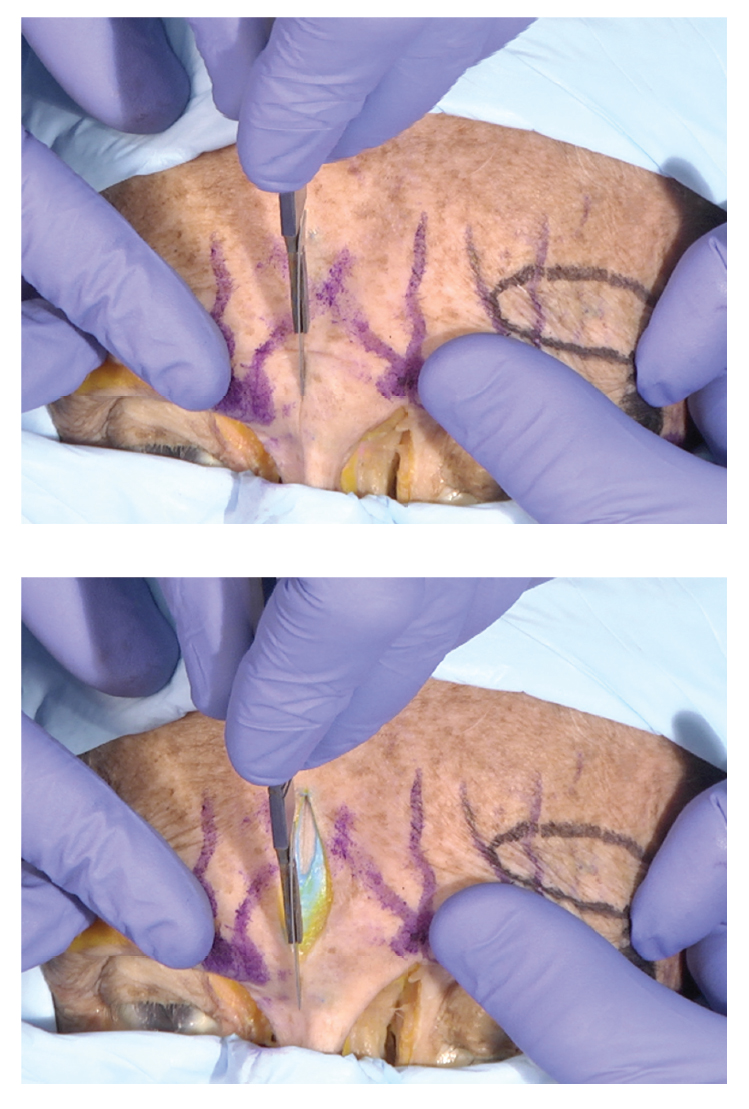
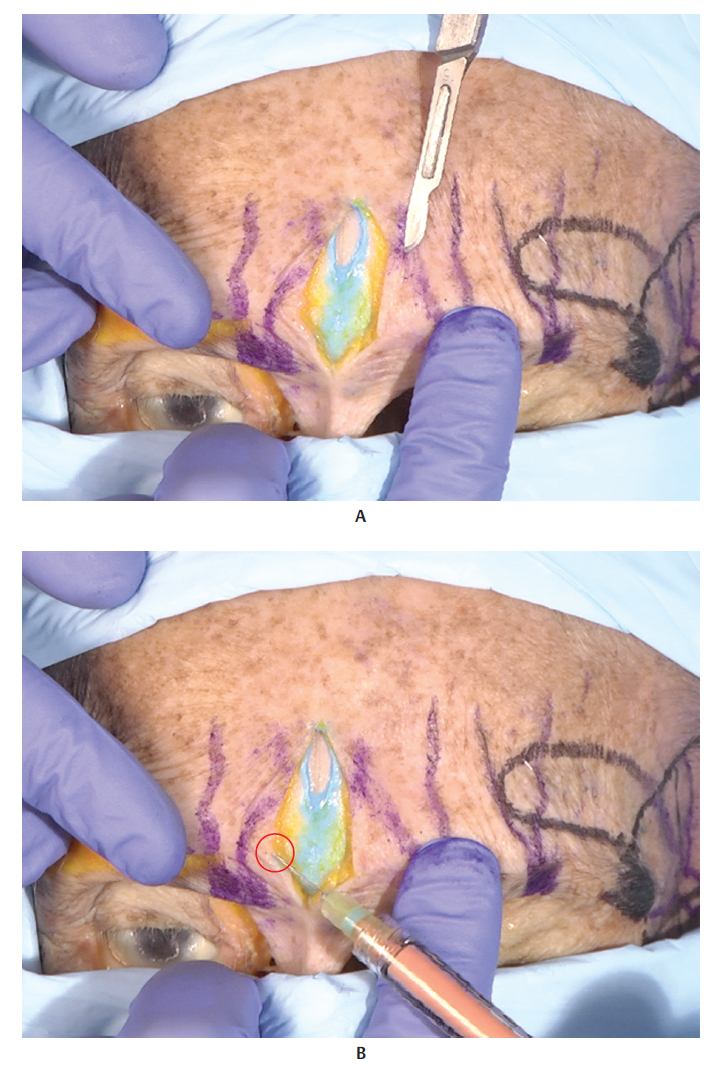
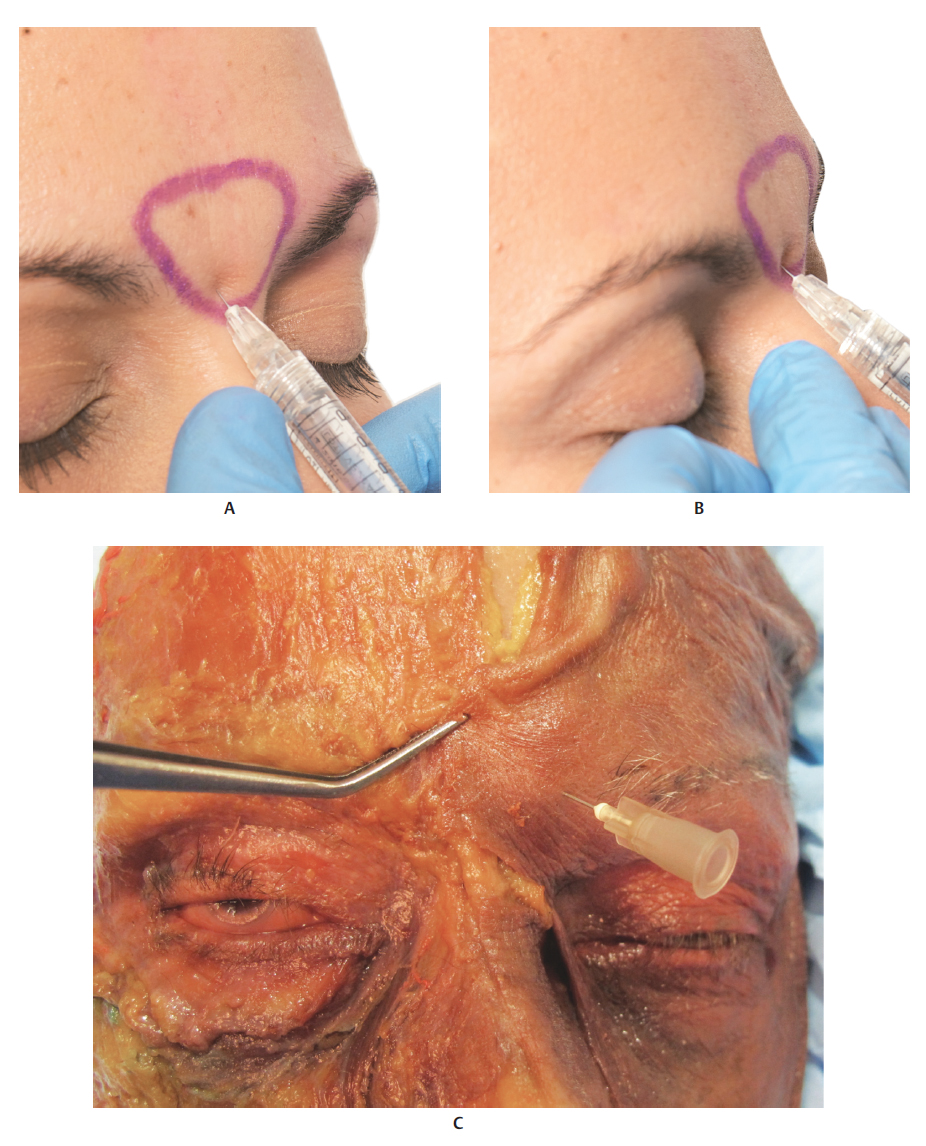
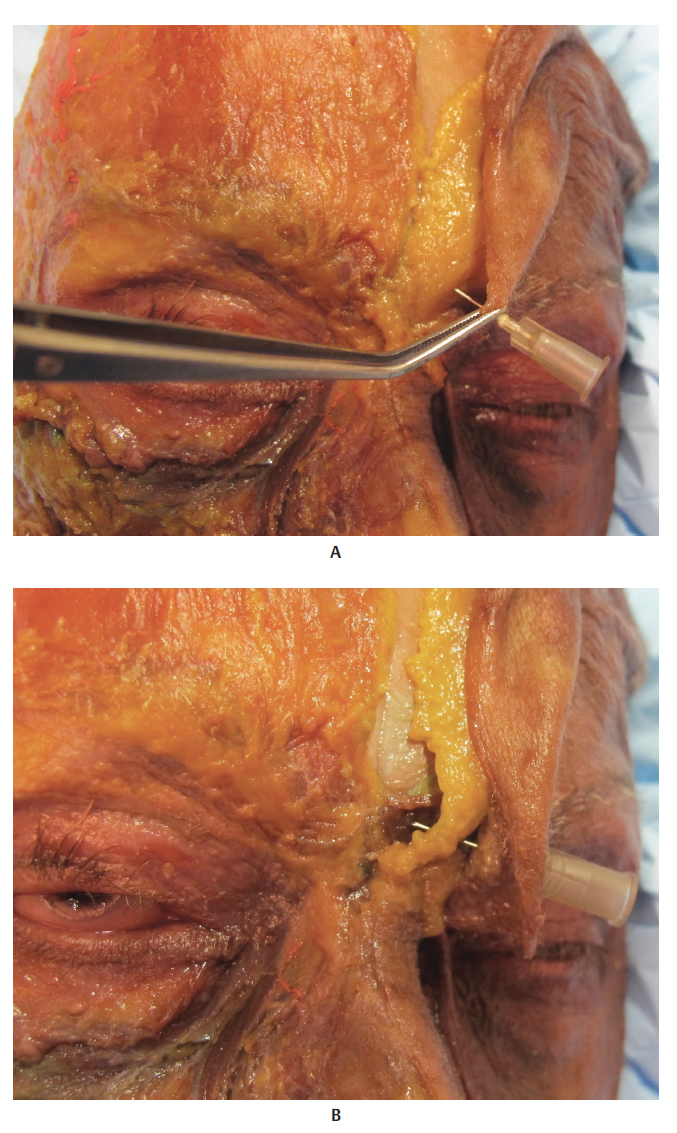
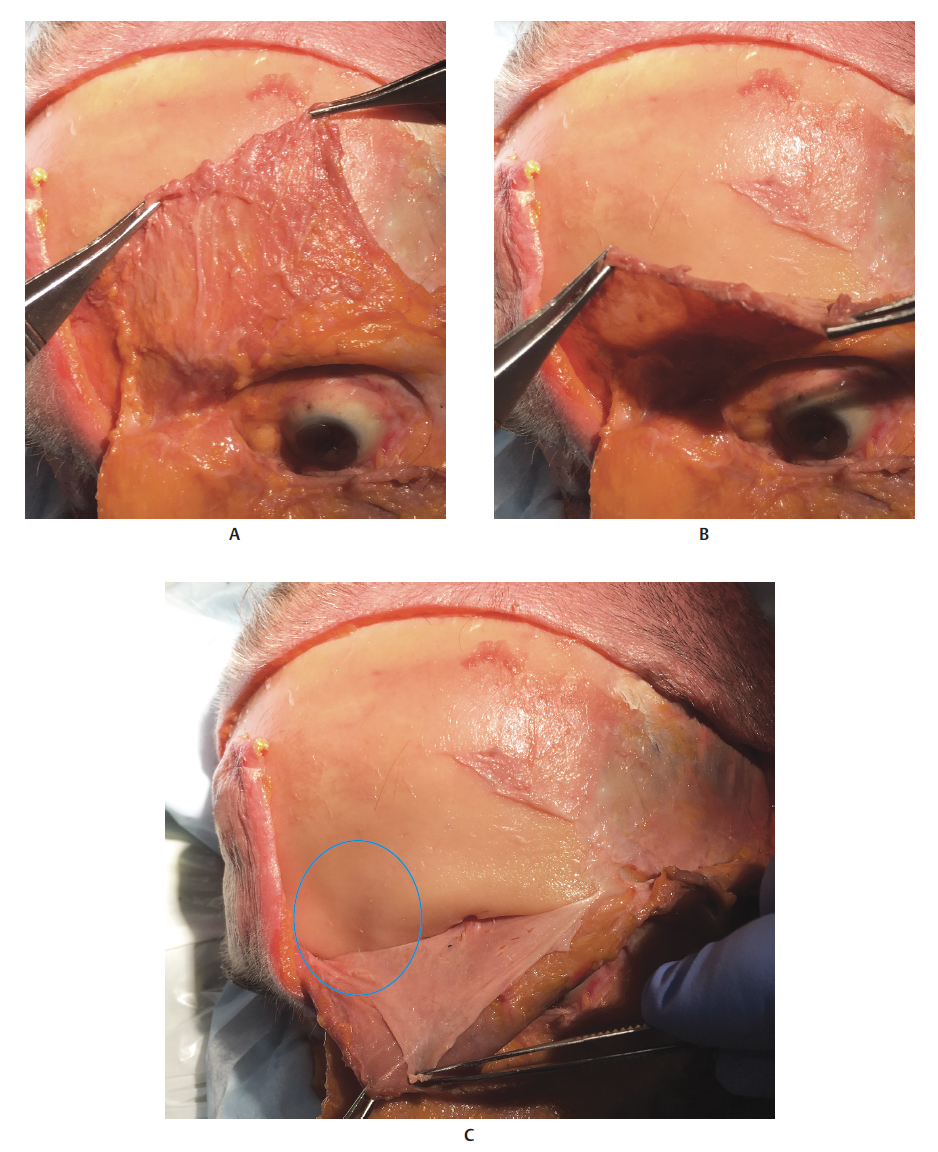
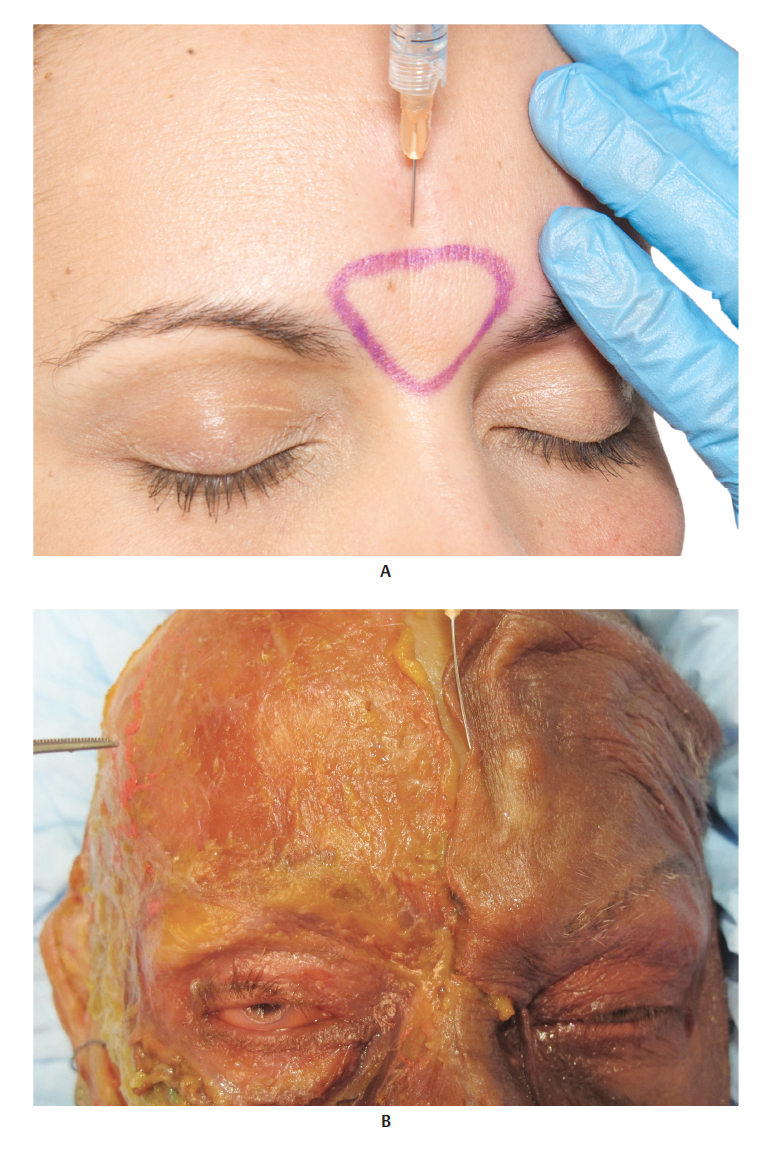
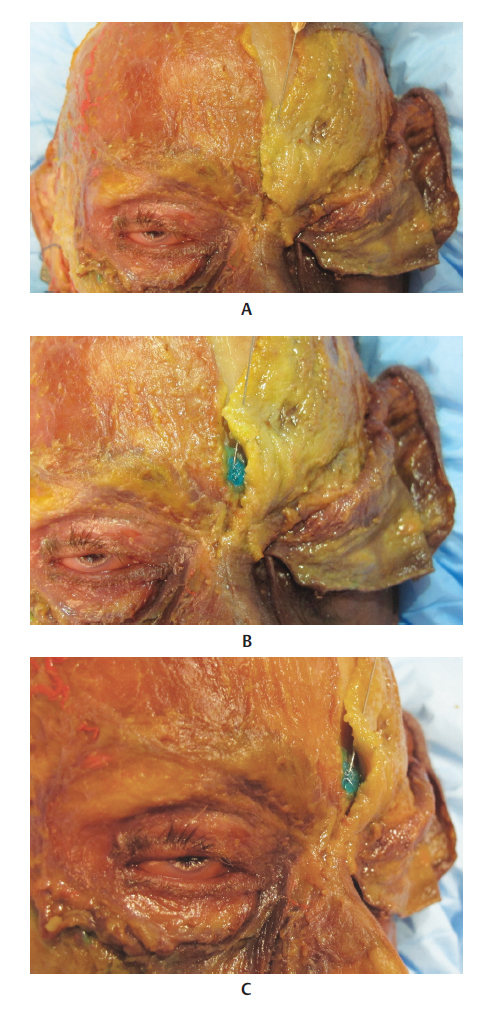
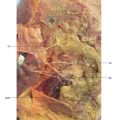
1 Shaw RB Jr, Katzel EB, Koltz PF, et al. Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg 2011;127(1):374–3832 Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg 2007;119(7):2219–2227, discussion 2228–22313 Carruthers J, Carruthers A. Volumizing the glabella and forehead. Dermatol Surg 2010; 36(3):1905–1909Fig. 9.1 A. Frontal view of the face focusing on the glabella.B. Frontal view of the face after removal of the skin, showing the superficial fat pad (SFP).C. Right side of the face showing the SFP and left side of the face showing the frontal muscle, orbicularis oculi muscle (OM), and corrugator muscle.D. Right side of the face showing the frontal muscle, OM, and corrugator muscle, and left side of the face with the aforementioned muscles removed, revealing the retroorbicularis oculi fat (ROOF) and suborbicularis oculi fat (SOOF).Fig. 9.2 A. Right side of the face after removal of the skin, superficial fat pad (SFP), and orbicularis oculi muscle (OM). The frontal, corrugator, and nasal muscles are visible. Left side of the face after removal of the skin, SFP, OM, and frontal muscle. The corrugator muscle and the bone structure of the aforementioned region are visible.B. Bone structure of the glabella.Fig. 9.3 Frontal view of the face.A. Close-up of the glabella, showing its corresponding vascularization and innervation.B. Corresponding arterial vascularization.C. Corresponding venous vascularization.D. Corresponding innervation.Fig. 9.4 Right profile view.A. Focus on the glabella.B. Region after removal of the skin, showing the superficial fat pad (SFP).C. Region after removal of the skin and SFP, exposing the frontal muscle, and orbicularis oculi muscle (OM). Retroorbicularis oculi fat (ROOF) is visible behind this.D. Bone structure of the region.Fig. 9.5 Right profile view of the glabellar region.A. Corresponding vascularization and innervation.B. Corresponding arterial vascularization.C. Corresponding venous vascularization.D. Arterial and venous vascularization above the frontal muscle and orbicularis oculi muscle (OM).E. Same illustration asD after removal of the superficial temporal fascia and the frontal superficial temporal artery. The corresponding arterial and venous vascularization is visible above the deep temporal fascia.F. Corresponding innervation.Fig. 9.6 A andB. Frontal view of a 3D digital model.C andD. Glabellar region in detail, withblue marking indicating the region.Fig. 9.7 A. Fresh cadaver with right side of the face showing the frontal muscle and left side of the face covered in skin.B. Right side of the face showing the frontal muscle and the skin of the left side of the face being folded back, exposing the superficial fat pad (SFP) of the forehead.C. Skin of the left side of the face has already been folded back completely, showing the SFP of the forehead.D. SFP of the forehead and frontal muscle being pinched and folded back.E. SFP of the forehead and frontal muscle folded back, exposing the frontal bone. The supraperiosteal plane is the safest site for glabellar filler injections, but this is nonetheless a high-risk area.Fig. 9.8 A. Glabella of a fresh cadaver with a 30 GX13 mm needle being inserted into the superficial intradermal plane for a hyaluronic acid (HA) injection, using the microdroplets technique.B. Glabella of a fresh cadaver with a 30 GX 13 mm needle being inserted into the superficial intradermal plane for an HA injection, using the retrograde injection technique. The raised outline caused by the needle shows that the injection has to be superficial in order to minimize the risk of complications.Fig. 9.9 Glabella of a fresh cadaver with a 27 GX 13 mm needle being inserted into the supraperiosteal plane for a hyaluronic acid (HA) injection, using the bolus technique. The supraperiosteal plane is the safest site for glabellar filler injections, but this is nonetheless a high-risk area.Fig. 9.10 Glabella of a fresh cadaver being dissected with a scalpel.Fig. 9.11 A. Dissected glabella of a fresh cadaver. Superficial fat pad (SFP) of the glabella and supraperiosteal area colored inturquoise after an injection of hyaluronic acid (HA) of the same color.B. Dissected glabellar area. Syringe simulating an intradermal injection with HA (red circle) . Note that the dermis is only 1 to 2 mm thick.Fig. 9.12 A. Upper third of a model on whom the glabellar area to be filled has been marked. A 27 GX 13 mm needle was inserted into the supraperiosteal plane, simulating an injection of the product using a bolus technique, after aspiration. Remember that negative aspiration does not rule out the risk of intravascular injection.B. Detail ofA in profile.C. Upper third of a fresh cadaver, frontal view, with needle inserted into the glabellar region, simulating a supraperiosteal injection.Fig. 9.13 A. Upper third of a fresh cadaver, frontal view, with needle inserted into the glabellar region, simulating a supraperiosteal injection. Skin has been folded back to reveal the superficial fat pad (SFP) of the glabella.B. Needle inserted into the glabellar region simulating a supraperiosteal injection. Skin and SFP of the glabella have been folded back, showing the procerus muscle.Fig. 9.14 A. Upper third of the left side of the face of a fresh cadaver with the frontal muscle being pinched.B. Frontal muscle being folded back to reveal the frontal bone.C. A bone depression is visible (blue circle) where the superficial fat pad (SFP) of the glabella is thicker.Fig. 9.15 A. Upper third of a model, frontal view, on whom the glabellar area to be filled has been marked. 25 GX 40 mm cannula inserted into the supraperiosteal plane, simulating injection of the product with a bolus technique.B. Upper third of a fresh cadaver, frontal view, with a 25 GX 40 mm cannula inserted into the glabellar region, simulating a supraperiosteal injection.Fig. 9.16 A. Upper third of the face of a fresh cadaver, frontal view, with a 25 Gx 40 mm cannula inserted into the glabellar region, simulating a supraperiosteal injection. Skin has been folded back to reveal the superficial fat pad (SFP) of the glabella.B. Skin and SFP of the glabella have been folded back, showing agreen-colored hyaluronic acid (HA) injection into the supraperiosteal plane.C. Profile view ofB showing that thegreen-colored HA was injected into the supraperiosteal plane. This is the safest plane for filler injections in this region.Fig. 9.7 Patient before (A) and after (B) a filler injection with a needle in the superficial wrinkles of the glabella, which persisted after injection of botulinum toxin type A.
Only gold members can continue reading. Log In or Register to continue