Chapter 4 NOMENCLATURE OF THE STROMAL VASCULAR FRACTION
Autologous stem cells are being used globally for numerous clinical indications, and the popularity of more readily procured stem cells, such as adipose-derived stem cells (ADSCs), is increasing dramatically. Table 4-1 details the clinical trials worldwide as of April 2017 that utilized ADSCs or adipose stromal vascular fraction (SVF) as a therapeutic.
The SVF and ADSCs are heterogeneous populations of multipotent mesenchymal stem cells. After harvesting, there are a number of methods (see General Isolation) used to obtain the raw clinical “isolate,” which is the SVF. The SVF can subsequently be used as a direct therapy to correct facial lipoatrophy, to decrease inflammation and pain associated with osteoarthritis, and even to treat scleroderma. Although many clinical trials are actively recruiting to assess the efficacy of the SVF in treating these conditions, a standardized procedure to isolate and characterize these cells has not been established.
In this chapter we will describe the components and general isolation of the SVF, review the variables associated with SVF isolation, and discuss how SVF treatment and characterization is intricately linked to successful clinical outcomes.
Stromal Vascular Fraction and Adipose-Derived Stem Cell Characterization
The stromal vascular fraction, or “raw isolate of adipose tissue,” is a heterogeneous population of cells, including but not limited to, endothelial cells, macrophages, pericytes, and ADSCs. Despite the widespread use of the SVF in therapeutics, there has been a lack of consensus on their characterization.
To characterize the SVF with flow cytometry before analysis, single cells are isolated, and cell clumps and autofluorescence are removed. DAPI exclusion is used to identify viable cells (top left box). CD45 is subsequently used to exclude cells of hematopoietic origin (top right). Endothelial mature cells are CD31+CD34−, whereas progenitors are CD31+CD34+. The pericyte proportion is represented by CD31−CD146+ population, while ADSCs are CD31−CD146−CD34+.
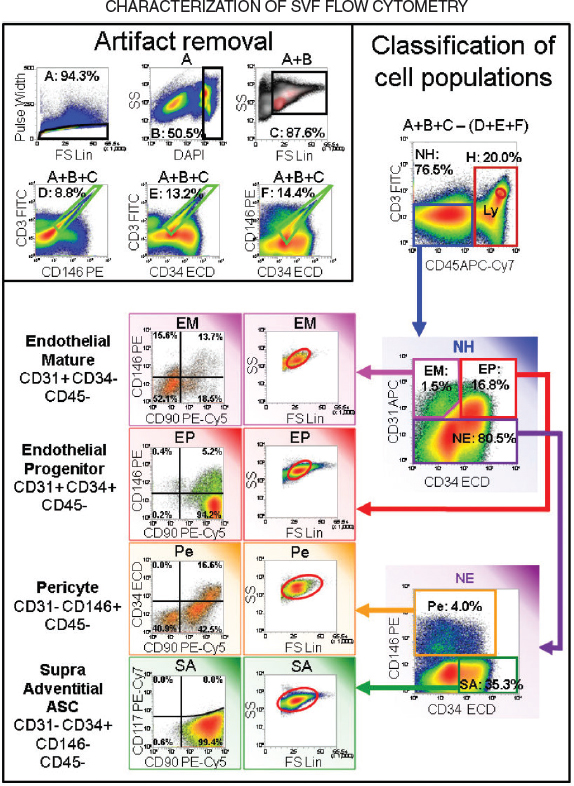
Traditionally, the most common way to distinguish cells, in both the laboratory and the clinic, is by flow cytometry. Functional assays specific to the cell type being studied are also used to assess the potency of a particular cell population. Flow cytometry is a quantitative tool that allows the user to rapidly analyze cellular populations and determine their viability, as well as the presence of cellular cluster of differentiation (CD) markers when used in conjunction with fluorescent antibodies. Cluster of differentiation or CD markers are cell surface molecules that can be used to classify cell populations. Viability should be greater than 70% to allow for differentiation of cellular populations.
Multicolorimetric flow cytometry for several surface antigens is indicated for particularly heterogeneous cellular populations, including the SVF. The use of numerous markers, both positive and negative, is important because there is not one single marker that is entirely inclusive of all SVF subpopulations.
Common leukocyte antigen (CD45), eliminates cells of hematopoietic origin, except red blood cells (RBCs), which can represent 25% to 45% of the SVF depending on a number of factors, including the donor site, patient characteristics, and isolation protocol used. To exclude red blood cells from later analysis lysis with an ammonium chloride solution is occasionally advocated. However, it remains unclear whether all RBCs are removed with the lysis procedure and how this solution affects other cells during the analysis. Instead, glycophorin A (CD235a) can be used as an exclusion marker for RBCs. To make the analysis clear, additional markers should be used to eliminate other cells of hematopoietic origin, including macrophages, which can be excluded based on their positivity for CD11b or CD14. It should be noted, however, that a large proportion of endothelial progenitors also express these markers. In this case, a panel of surface markers, including stem progenitor markers (CD105, CD90, CD73, and CD34) as well as endothelial markers (CD31) should help to distinguish these populations.
Endothelial cells represent approximately 10% to 20% of the SVF. To differentiate endothelial cells and their progenitors, CD-31 (also known as PECAM-1 or endothelial cell adhesion marker) should be used in concert with stem markers, including CD105 or CD34. Traditionally, CD31+CD34+ cells are defined as endothelial progenitors, whereas CD31+CD34− antigens are associated with mature endothelial cells. 2 CD-31 expression has also been used as criteria for separating cells with greater “stemness” from the SVF. Boquest et al 3 found that CD45−CD34+CD105+CD31− cells highly expressed genes related to stemness and were able to differentiate into bone, fat, and neural-like tissue, whereas CD45−CD34+CD105+CD31+ cells overexpressed endothelium and MHC-class II (HLA-DR) markers and were unable to proliferate in culture.
CD146 can delineate pericytic populations within the SVF; however, there are discrepancies in the literature on how these cells are additionally characterized. General consensus suggests that pericytes should not express hematopoietic (CD45) nor endothelial (CD31) markers, but should express stem progenitor markers, including CD90. They should be positive for certain stem progenitor markers, including CD90. Variable CD34 expression is also evident. 2
Multiple stem-progenitor markers, including CD73, CD90, CD105, CD117, CD13, and CD34, can be used in combination with the above markers to identify tissue resident progenitors. CD90 and CD105 are also highly expressed on endothelial populations; thus multiple markers are needed to exclude and separate each subpopulation within the SVF.
One of the most common progenitor markers used to identify stromal stem cells is CD34, which represents about 20% of the total SVF population. A high proportion (70% to 80%) of stem progenitor markers (including CD73 and CD13) are associated with the CD45−CD31−CD34+ cell population. 4 Boquest et al 5 noted that cells with a CD45−CD34+CD105+ expression profile were able to proliferate rapidly in culture and differentiate into chondrogenic, adipogenic, and osteogenic lineages. Similarly, CD34 should be used in conjunction with other stem markers to appropriately characterize stromal progenitors with the SVF.
Fibroblastoid Colony–Forming Unit Assay
In addition to employing flow cytometry to characterize the SVF, progenitor number can be estimated using a fibroblastoid colony–forming unit assay (CFU-F). This procedure, which was originally adapted for use in bone marrow–derived mesenchymal stem cells, allows the investigator to determine the number of colonies derived from an original progenitor within the SVF. Following isolation, the SVF is seeded at a very low density (anywhere between 40 and 400 cells/cm2) and allowed to proliferate for 10 to 14 days. 2 Colonies containing 50 cells or greater are then counted. From this information, the percentage of stromal progenitor cells within the SVF can be obtained as well as the rate of early population doubling times. The literature suggests that the progenitors represent approximately 0.5% to 5% of the total nucleated SVF cell population. 6
Adipose-Derived Stem Cell Classification
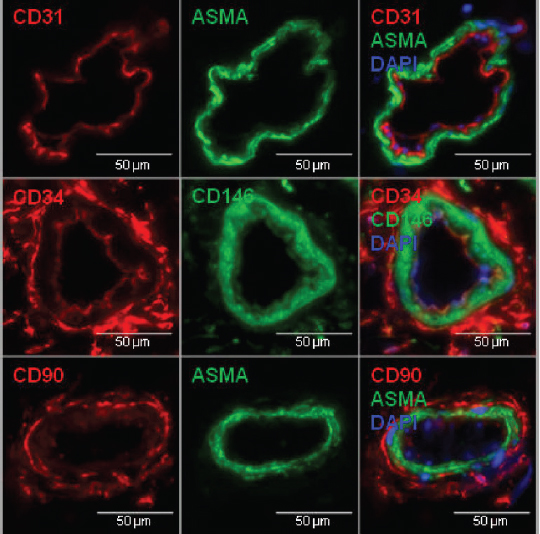
Immunofluorescence staining of adipose tissue shows CD31+ endothelial marker co-localized with alpha smooth muscle actin (alpha-SMA) on the blood vessel luminal wall. CD34 staining was visualized in the supradventitial layer adjacent to the luminal endothelial wall. CD90 and CD34 were similarly located in the supradventitial layer of vessels.
Characterization of cells can also be performed after SVF culture expansion to obtain a more homogeneous ADSC population; however, approximately 15% of the cell populations will not adhere to the culture plate and will be washed away. ADSCs are mainly categorized by their culture adherence and dramatic decrease in CD45+ (hematopoietic) cells. Surface markers can also be used to characterize ADSCs. The International Federation for Adipose Therapeutics and Science (IFATS) along with the International Society for Cellular Therapeutics (ISCT) specifies that ADSCs should have less than 2% contamination from hematopoietic (CD45+) cells, and greater than 90% expression of stromal stem/progenitor cell markers. 7 A low proportion of endothelial cells (CD31+) should also be observed in cultured ADSCs. Furthermore, to distinguish ADSCs from contaminating bone marrow–derived stem cells, many investigators have suggested using a combination of CD36 and CD106. ADSCs should primarily express CD36, whereas bone marrow–derived cells should express CD106. 7
When identifying the multipotent mesenchymal ADSC population, stem/progenitor markers (CD73, CD105, CD13, CD90, and CD34) should also be used in conjunction with markers stated above.
However, it should be noted that the proportion of cells expressing these markers can change with culture conditions and continued passaging. Thus analysis of these cells should be performed during the same passage, in the same culture media, and at the therapeutic time-point. This allows for a more accurate representation of the cells being used clinically.
Related posts:
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 5 ANTIINFLAMMATORY STEM CELL PRINCIPLES
Chapter 5 ANTIINFLAMMATORY STEM CELL PRINCIPLES
 Chapter 9 GROWTH FACTORS IN THE LIPOASPIRATE
Chapter 9 GROWTH FACTORS IN THE LIPOASPIRATE
 Chapter 2 ANALYSIS OF THE PATIENT
Chapter 2 ANALYSIS OF THE PATIENT
 Chapter 10 AN OVERVIEW OF FAT GRAFTING TECHNIQUES
Chapter 10 AN OVERVIEW OF FAT GRAFTING TECHNIQUES
 Chapter 1 THE COLEMAN TECHNIQUE
Chapter 1 THE COLEMAN TECHNIQUE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


