Chapter 9 GROWTH FACTORS IN THE LIPOASPIRATE
Fat grafting is used for many different indications in soft tissue repair and has become a leading tool in plastic surgery because of its reliability and safety. However, many long-term studies have shown a loss of volume in the transplanted tissue especially in the early stages after grafting. A number of reasons have been discussed and studied as critical causes of this loss.
Local anesthetics, which are infiltrated into the donor as well as in the recipient site by many plastic surgeons, have been considered as relevant factors for diminished graft viability. A number of publications have focused on this specific issue. Although Livaoğlu et al 1 and Shoshani et al 2 did not observe negative effects of lidocaine and epinephrine on the take or the survival of fat grafts, Keck et al 3 reported a decrease of adipose-derived stem cell (ADSC) viability. Gugerell et al 4 and Girard et al 5 further observed detrimental effects of lidocaine on ADSCs. 4 , 5 Taken together, at present in cannot be ruled out that the use of local anesthetics exerts a toxic effect on fat grafts, especially on adipose progenitor cells.
A more commonly accepted explanation for diminished graft viability is insufficient oxygen supply after transfer of the fatty tissue. The supply of oxygen by diffusion is limited to a few millimeters, with tissue farther away inevitably becoming hypoxic. As a consequence of prolonged hypoxia, transplanted cells undergo apoptosis and necrosis, resulting in the loss of volume and cicatrization. In this context, Kato et al 6 described a three-zone model that consists of a superficial surviving zone, a regenerating zone, and a central necrotizing zone. Thus sufficient neovascularization is indispensable for transplant survival and a stable result. The formation of blood vessels from preexisting vasculature, also called angiogenesis, is a highly complex process that is critically dependent on myriad factors. Angiogenesis also directly depends on the presence of growth factors.
This chapter will provide insight into current knowledge about growth factors during fat grafting, summarize potential risks, and provide an outlook of future developments in this field.
Growth Factors
Growth factors are naturally occurring proteins or steroid hormones that act by autocrine or paracrine signaling. They bind to specific receptors of target cells and stimulate, among other processes, cellular growth, proliferation, differentiation, and, what is essential, angiogenesis.
One of the most prominent growth factors involved in angiogenesis is the vascular endothelial growth factor (VEGF). VEGF knockout in mice is lethal, underscoring the overall importance of this protein. During angiogenesis, VEGF initiates the proliferation, migration, and differentiation of endothelial cells and mediates tubulogenesis by regulating vascular permeability. An important stimulus for an increased VEGF production is, among other factors, tissue hypoxia. It has also been found that VEGF secretion positively correlates with the rate of adipocyte differentiation. 7
Another crucial factor for angiogenesis and adipose tissue expansion is the basic fibroblast growth factor (bFGF), which is known to stimulate proliferation and migration of endothelial cells. Moreover, bFGF enhances the proliferation of ADSCs and the mitosis of adipocytes.
Insulin-like growth factor 1 (IGF-1) contributes to angiogenesis by stabilizing new blood vessels. In addition, it possesses a positive effect on the survival of adipocytes and thereby enhances the viability of fat grafts after transplantation.
Platelet-derived growth factor BB (PDGF-BB) is involved in angiogenesis through recruitment of pericytes, which contribute to stabilization and maturation of newly formed blood vessels. Moreover, it has an antiapoptotic effect on existing cells in the stromal vascular fraction (SVF), stimulates the proliferation of ADSCs, and acts as a survival factor.
Other important growth factors in adipose tissue are stromal cell–derived factor-1-alpha (SDF-1-alpha) and the epidermal growth factor (EGF). SDF-1-alpha plays an important role in angiogenesis, while EGF is an important factor for the induction of mitosis.
Taken together, growth factors such as VEGF, bFGF, IGF-1, PDGF-BB, SDF-1-alpha, and EGF facilitate angiogenesis through cell recruitment and further maturation as well as stabilization of neovessels. They represent important survival factors for transplanted tissue and promote adipose tissue expansion.
Growth Factors and Lipoaspirates
Adipose tissue is known to be a rich reservoir for growth factors. Therefore fat grafting encompasses the transfer not only of tissue mass with a volumetric effect, but also growth factors and growth factor–producing cells. However, during fat harvesting, processing, storage, and injection, adipose tissue undergoes significant manipulation, which may impose unknown effects on the growth factors of the lipoaspirate.
We previously published a report demonstrating that lipoaspirates contain significant amounts of growth factors. 8 In our study, lipoaspirates were harvested and processed according to the Coleman protocol. As a result of centrifugation, the lipoaspirate can be divided into four fractions: an upper oily fraction, a layer of the purified fat, a watery fraction, and a cellular pellet. 9 The cellular pellet consists of various cells that some plastic surgeons use as the “red pellet” to enrich the fat graft, although other surgeons do not use it. The literature also speaks of the cellular pellet as a distinct fraction/layer. The highest concentrations of growth factors were detected in the purified adipose tissue fraction after centrifugation or in native adipose tissue, which was not further centrifuged after harvest.
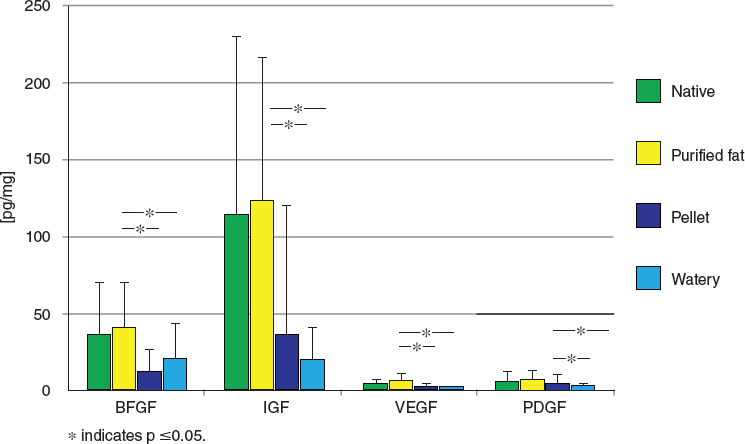
Considerable quantities of VEGF, bFGF, IGF-1, and PDGF-BB were found in native adipose tissue and purified fat samples in different concentrations. The highest growth factor content was measured in purified fat, whereas the pellet as well as the watery fraction contained significantly lower amounts. The level of IGF-1 was highest, followed by bFGF, whereas VEGF and PDGF-BB were present in significantly lower concentrations.
Furthermore, growth factors were analyzed from native adipose tissue or purified adipose tissue after incubation in growth medium for 3 and 5 days, respectively. Importantly, purified and native fat secreted significant amounts of growth factors even after 3 and 5 days of culture. 8
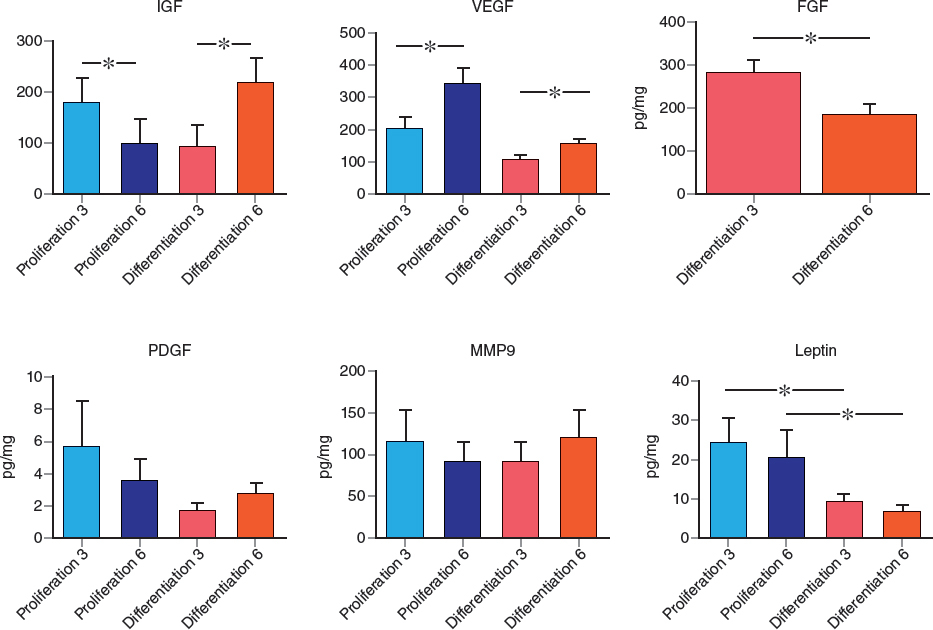
In a recent study we focused on the content of growth factors in the SVF. 10 The SVF was incubated in either differentiation or proliferation media, and levels of VEGF, IGF, PDGF, leptin, and matrix metallopeptidase-9 (MMP-9) were measured by ELISA after 3 and 6 days. We found that the type of culture medium had a significant influence on growth factor secretion. While the concentration of VEGF increased from day 3 to 6 in differentiation and proliferation media, leptin levels decreased over the same period in both media types. Levels of IGF, PDGF, and MMP-9 increased only when cultured in differentiation medium. We concluded that cultivation of the SVF with differentiation medium results in elevated growth factor concentrations and thus promises a more stable outcome. This aspect is of importance for in vitro SVF expansion in tissue engineering approaches and stem cell therapy.
Graded densities is a new concept introduced by Allen et al. 11 The authors hypothesized that centrifugation leads to a separation of the purified fat fraction into phases of graded densities. Highest and lowest density fatty tissue was injected into mice and harvested after 2 weeks for short-term follow-up and after 10 weeks for long-term follow-up, respectively. Survival of highest density fat was higher than lowest density fat after both 2 and 10 weeks. Subsequent analysis revealed that the count of ADSCs as well as the concentrations of the VEGF, SDF-1-alpha, PDGF, and adiponectin were significantly higher in the highest density fat compared with the lowest density fat fraction. The authors concluded that the highest density phase of lipoaspirate resembles the most favorable fraction because of its high growth factor and progenitor cell content and yields longer-lasting results.
The technique used for harvesting and processing lipoaspirate further alters the content of growth factors in the lipoaspirate. Today a great variety of cannulas are available so that plastic surgeons can adapt to the specific needs of each procedure. The microfat grafting procedure consists of tissue harvest with a multiperforated cannula, leading to a more liquid lipoaspirate that allows fat grafting into superficial dermal layers.
Notwithstanding the unique benefits of this technique, Alharbi et al 12 reported that lipoaspirates harvested and processed by the conventional Coleman protocol contained significant higher amounts of VEGF and IGF-1 compared with lipoaspirates harvested by the microfat harvesting technique. No difference was seen in the concentrations of bFGF or PDGF.
These issues can be addressed by using different cannulas for distinct purposes. Large cannulas for harvest and injection according to the Coleman protocol ensure a high level of angiogenic factors, which has been found to lead to a higher graft take. This technique is favored when maximal graft take is the primary goal, as in breast augmentation. On the other hand, Magalon’s micrografting technique 13 can be used to thicken and repair the dermis with increased numbers of ADSCs.
Related posts:
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 5 ANTIINFLAMMATORY STEM CELL PRINCIPLES
Chapter 5 ANTIINFLAMMATORY STEM CELL PRINCIPLES
 Chapter 8 DETERMINATION OF FAT VIABILITY
Chapter 8 DETERMINATION OF FAT VIABILITY
 Chapter 2 ANALYSIS OF THE PATIENT
Chapter 2 ANALYSIS OF THE PATIENT
 Chapter 10 AN OVERVIEW OF FAT GRAFTING TECHNIQUES
Chapter 10 AN OVERVIEW OF FAT GRAFTING TECHNIQUES
 Chapter 1 THE COLEMAN TECHNIQUE
Chapter 1 THE COLEMAN TECHNIQUE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


