CHAPTER 4 Embryology
KEY POINTS
The lymphatic system has several critical roles, including transporting tissue fluids and plasma protein back to the bloodstream and providing major pathways for the spread of metastatic tumor cells.
The development of the lymphatic vasculature is a stepwise process requiring the specification of lymphatic endothelial cell progenitors from the embryonic veins.
The embryology of the vascular and lymphatic systems during gestation must be considered collectively because they are interconnected.
The lymphatic system transports tissue fluids and extravasated plasma proteins back to the bloodstream and absorbs lipids from the intestinal tract. The lymphatic system also plays a crucial role in immune response and is one of the main routes for the metastatic spread of tumor cells.
The developmental origin of the lymphatic system remained unclear until the first years of the twentieth century, when Sabine proposed (after extensive ink injection experiments in pig embryos) that the jugular sacs arose from the anterior cardinal vein. Recent analyses of targeted gene deletions and genetic lineage tracing studies in mice have confirmed Sabine’s models. 1
Overview of the Lymphatic System
The lymphatic system is the third vascular system. A major function of the lymphatic vasculature is to transport extracellular fluid back to the cardiovascular system. When blood enters a capillary bed, high hydrostatic pressure on the arterial side of the capillary causes plasma to leak into the interstitial space. On the venous side of the capillary bed, the inward pull of the blood’s high osmotic pressure exceeds the outward push of its hydrostatic pressure, causing the previously filtered fluid to rush back into the capillary bed and reenter the systemic circulation. This system allows 90% of the filtered fluid to reenter the circulation; the remaining 10% is returned to the systemic circulation by the lymphatic system through a series of successively larger lymphatic vessels. Lymph is a fluid that is similar in composition to plasma but contains leukocytes and higher concentrations of macromolecules, such as proteins and lipids. Lymph enters the lymphatic system through lymphatic capillaries that are located near blood capillaries and is subsequently transferred to larger lymphatics, which are known as collecting lymphatic vessels (Figs. 4-1 and 4-2). These collecting lymphatic vessels then transfer the lymph unidirectionally toward the chest.
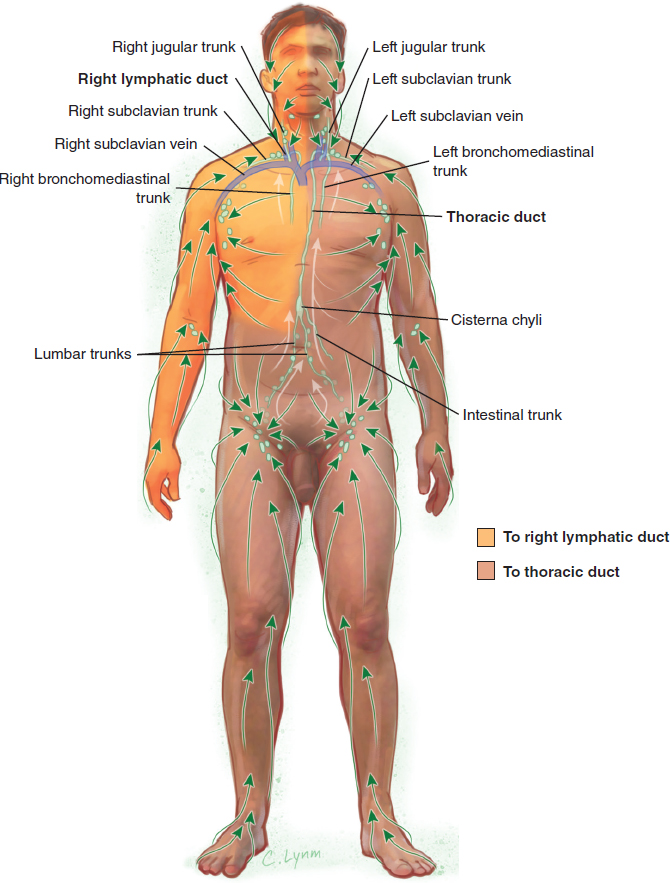
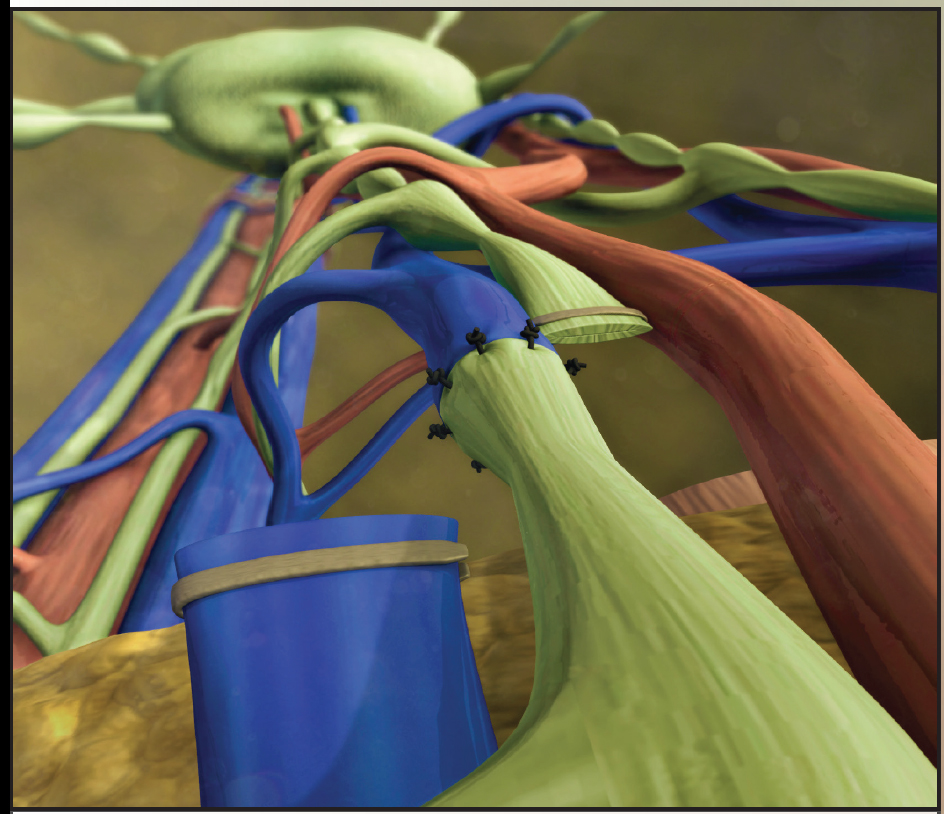
Collecting lymphatics from the left side of the body, the abdomen, and from both legs drain lymph into the thoracic duct, which then drains the lymph into the left subclavian vein. Lymph from the right side of the body, head, and thorax drains into the right subclavian vein after it first drains into the right lymphatic duct. On entering the subclavian veins by way of lymphaticovenous anastomoses, the lymph is drained back into the venous system and returned to the systemic circulation.
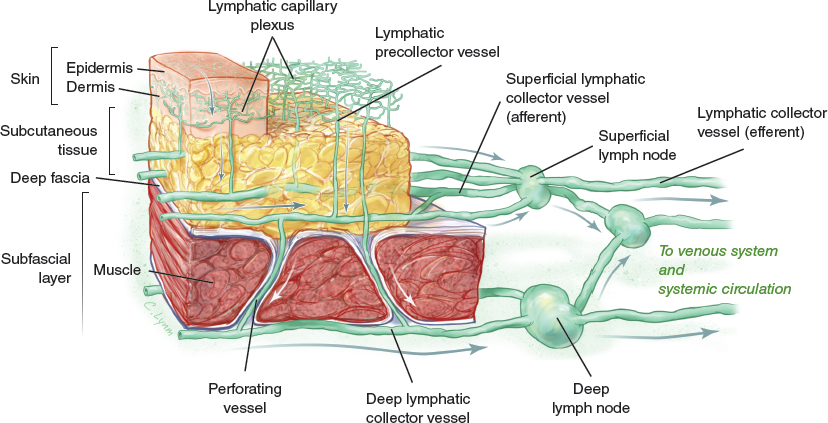
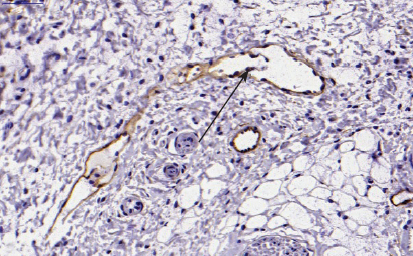
Lymphatic capillaries are thinwalled vessels that are composed of a single layer of lymphatic endothelial cells (LECs). These tiny vessels are only 30 to 80 µm in diameter, are not surrounded by pericytes or smooth muscles cells, and usually lack a basement membrane (Fig. 4-3). Lymphatic capillaries are discontinuous and contain gaps that make them highly permeable. This allows macromolecules and leukocytes to easily enter the vasculature. As lymph transits through the lymphatic capillaries, the fluid moves into precollector vessels. Unlike the capillaries, these vessels have some incomplete coverage by smooth muscle cells. The fluid then moves from precollector vessels to collecting lymphatics, which are larger vessels covered by smooth muscle cells that contain a basement membrane (see Fig. 4-3).
In addition, collecting lymphatics contain valves that maintain unidirectional flow (Fig. 4-4). Unlike the blood in the cardiovascular system, the lymph in the lymphatic system is not propelled forward by the heart. Instead, lymphatic fluid is moved by the relatively weak intrinsic pulsation of its smooth muscles cells in the lymphatic collectors. This force is greatly augmented by skeletal muscular contraction during periods of physical activity.
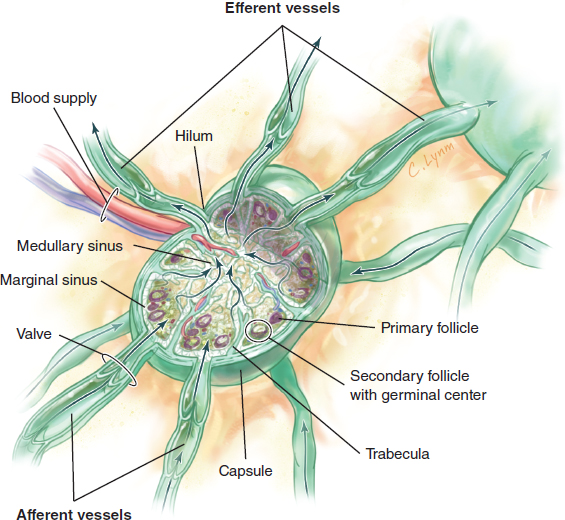
As lymph travels from lymphatic capillaries back to the venous circulation, the lymph is filtered in the lymph nodes (Fig. 4-5). Lymphatic fluid enters the lymph node through afferent lymphatic vessels that drain into the subcapsular sinus and leaves the lymph node through efferent lymphatics located in the medulla. A typical adult human has 600 to 700 lymph nodes, which have various functions. For example, lymph nodes filter out waste products found in the lymph entering from the afferent lymphatic vessel. In addition, lymph nodes provide an environment for leukocytes to interact with activated antigen-presenting cells, allowing the creation of immune responses to pathogens (see Chapter 10). This interaction is dependent on lymph node resident cells and migrating leukocytes that enter the lymph node through the high endothelial venules.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


