Chapter 37 FAT GRAFTING FOR BREAST AUGMENTATION IN ASIANS
The number of patients requesting breast augmentation is increasing steadily in Asia, especially in China. Although breast augmentation with an implant remains the most popular cosmetic breast surgery, a significant percentage of patients in Asia refuse this operation because they worry about foreign materials in their body. Moreover, the use of a breast implant is also associated with an increased risk of certain surgical complications and both early (infection and incision separation) and delayed adverse effects (capsular contracture, silicone leaks, and scar formation).
Because they did not want postoperative incisional scars or a less natural shape and feel after augmentation with implants, some patients turned to augmentation with injectable materials. An estimated 500,000 patients underwent breast augmentation with injections of polyacrylamide hydrogel (Amazing Gel). However, clinical use of Amazing Gel has been prohibited by the Chinese government since April 2006, and some countries prohibit its use in the breast. It was found that this material could cause severe complications, including breast tissue necrosis and chronic pectoralis inflammation induced by its infiltration.
In recent years, good to excellent outcomes have been achieved with fat grafting for breast augmentation by many plastic surgeons worldwide. This technique has been found to create long-lasting enhancement of breast size, shape, and texture. Zheng et al, Illouz and Sterodimas, Coleman and Saboeiro, and other authors have reported that fat grafting is an effective method for breast augmentation or reshaping. Most Asian women do not want an excessive increase in their breast volume, but rather desire a natural, moderate result. Therefore breast augmentation with fat grafting, which combines body sculpture and augmentation of small-sized breasts, may be the best option for many Asian women. In this chapter, we present our unique experience of fat grafting for breast augmentation in Asians, including special considerations, indications, preferred surgical techniques, and clinical outcomes.
Material and Methods
SPECIAL CONSIDERATIONS
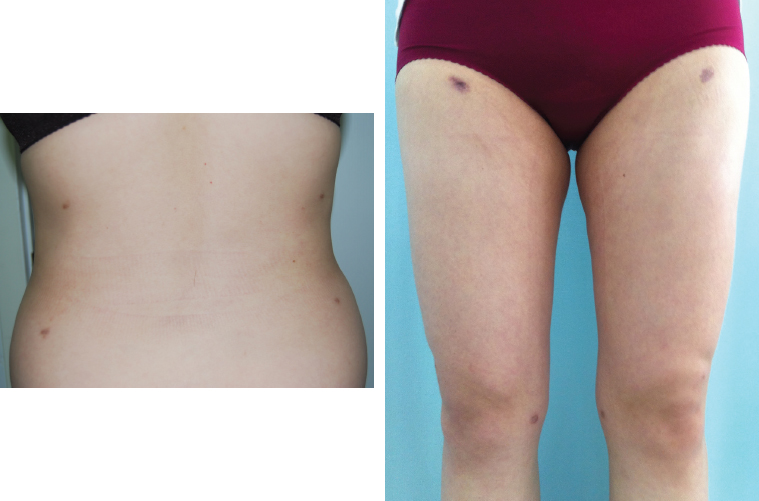
Scarring can be a serious problem that limits a patient’s clothing choices if the incisions for liposuction are not placed in areas that will be hidden by clothes. In this patient, the scars in her back and thighs are still visible 2 years after a fat grafting procedure.
Asian women have special characteristics that need to be considered when a surgeon performs fat grafting for breast augmentation. These patients are usually thin and small, with proportionally smaller breasts. The area to be liposuctioned should be large enough to provide adequate fat to ensure an obvious increase in breast volume. Therefore circumferential liposuction of the trunk or thigh is often required. As stated, because of possible poor scar formation, incisions for liposuction and fat grafting need to be placed in the hidden areas. Asian women are more likely to form hypertrophic scars than Caucasian women.
INDICATIONS
Fat grafting is more appropriate for women who desire only moderate breast augmentation or those who simply want to restore their previous shape of the breast after weight loss, pregnancy, breastfeeding, ptotic breasts as a result of aging, tuberous breast deformity, severe asymmetry, or simply implant-to-fat conversion. Fat grafting is also recommended for women who wish to obtain more natural results with no sense of a foreign body in their breasts.
It is prudent to consider baseline breast mammography, ultrasound, and MRI evaluation before lipoinjection.
DONOR SITE SELECTION AND PREOPERATIVE MARKING

Areas for liposuction and fat grafting to the breast are marked with the patients in the upright position. Typical areas for liposuction include the abdomen, flanks, trochanteric region, inner thigh, the medial aspect of the knees, and the upper arms, depending on the patient’s natural body fat distribution.
No clear correlation has been shown between the donor site location and the longevity of the implanted fat; thus the donor site can be selected based on identification of the region with sufficient adipose tissue or even on the patient’s preference. We prefer to perform circumferential abdomen liposuction at the first session of fat grafting and circumferential liposuction of the thighs if there is a second session.
For circumferential abdominal liposuction, entrance incisions are needed for liposuction of the anterior abdomen and flank; one is placed in the pubic hairline, another in the umbilicus, and the third in the intergluteal fold for liposuction of the flank in the prone position. For circumferential thigh liposuction, two 0.4 cm incisions are placed near the pubic hair above the inguinal fold for liposuction of the anterior aspect of the thigh, and two incisions are placed in the infragluteal fold (in the perpendicular line from the tubercle of the ischium) for liposuction of the posterior aspect of the thigh.
ANESTHESIA
Because significant quantities of fat are required for breast augmentation, the liposuction area usually needs to be large, so we perform the procedure with the patient under intravenous sedation through the tumescent technique.
INCISIONS FOR FAT HARVESTING
Incisions are made in the donor sites using a No. 11 blade. For abdominal fat harvesting, two incisions are made: one in the middle of the pubic hairline and one in the umbilicus. For harvesting of fat from the thighs, an incision is made in each subgluteal fold for liposuction of the posterior area, and an additional incision is made near the pubic hair above the inguinal fold for liposuction of the anterior area of the thigh and medial area of the knee. If there are any previous scars in the donor sites, they certainly can be used as the incision sites.

To prevent skin abrasion at the incision, before liposuction a skin protector made from a 1 cc syringe is inserted into the incision and secured with sutures.
HARVESTING AND PROCESSING
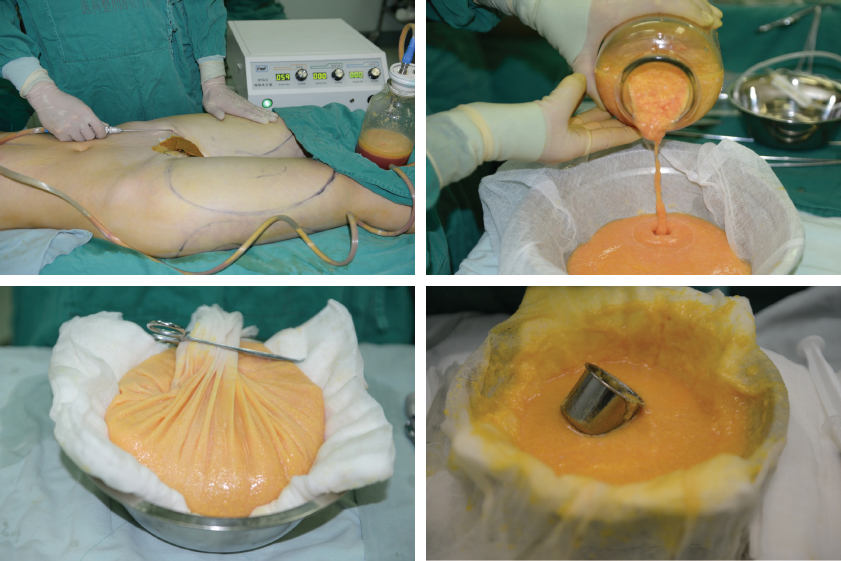
After intravenous sedation has been administered, the harvest sites are infiltrated with tumescent solution (20 ml of 2% lidocaine with epinephrine, 1:100,000/L of normal saline solution). The fat is aspirated using a three-holed blunt cannula (with a 2.5 to 3 mm inner diameter) connected to a suction machine with low negative pressure (–400 mm Hg). The processing procedure we use to prepare fat for injection is similar to the method described by Kuran and Tumerdem. The surgery is performed under intravenous sedation, so no sodium bicarbonate is used as a buffer to alleviate injection pain during the infusion of the tumescent solution. All aspirated fat is rinsed one or two times with 4° C cool normal saline solution to remove blood, lidocaine, and extracellular oil. It is then collected within a sterile container lined with a single layer of cotton gauze. After filtering, the washed lipoaspirate packed in the gauze is left to dry on a cotton pad, which is changed with a dry one every 5 minutes, until it reaches a semisolid state.
Related posts:
 Chapter 38 COMPOSITE BREAST AUGMENTATION
Chapter 38 COMPOSITE BREAST AUGMENTATION
 Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


