Chapter 38 COMPOSITE BREAST AUGMENTATION
Although the concept of composite breast augmentation (CBA) is simple, it has revolutionized our approach to breast surgery. CBA combines the advantages of immediate volume enhancement provided by implants with the unique properties of fat grafting, which makes it possible to contour the breast shape as desired. Not only does the patient benefit by breasts that have a natural feel and appearance as a result of fat grafting, but also derives the concomitant advantage of liposculpture of the body from the harvest of autologous fat.
As many surgeons will attest to, one of the most challenging problems with the use of breast implants is having adequate soft tissue coverage of the underlying implant. Previously this issue was addressed by submuscular placement of implants. However, CBA enables premuscular implant placement, with camouflage of the implant afforded by fat grafting. This avoids the pitfalls associated with submuscular implants, such as a higher incidence of hematoma, pain, and animation of the implant with activity.
I initially described CBA in 2009 in a French publication. 1 Subsequently I detailed the concept and formally introduced the term composite breast augmentation. 2 In 2015 a further review of CBA was published describing its utility in aesthetic breast surgery. 3 , 4
This chapter will outline the place of CBA in aesthetic breast surgery, addressing its utility in primary aesthetic surgery for hypoplastic breasts and reviewing its use in secondary aesthetic cases. It is outside the scope of this chapter to address CBA for the correction of congenital malformations such as Poland syndrome.
PRIMARY COMPOSITE BREAST AUGMENTATION
Until 2000, most breast implants were placed in a submuscular position. Furthermore, because the use of silicone implants was banned in such countries as France and the United States for at least 6 years, all implants used at that time were saline filled. Several problems were encountered with submuscular implants: an increased incidence of hematoma, which subsequently led to increased capsular contracture rates (reported to be up to 5%); increased pain noted by the patient for several days postoperatively; dynamic activity of the implant; and an appearance of “bottoming out and down” in a concerning number of patients.
The introduction of new-generation cohesive silicone gel implants resulted in prostheses with improved shell coverage and reduced silicone bleed. Surgeons rapidly observed a significant decrease in the appearance of rippling, and we were able to use anatomic shaped implants. This resulted in the introduction of premuscular, subfascial implant positioning, as described by Graf et al 5 and Góes and Landecker. 6 The first presentation by Delay et al 7 at a French Congress in 2008 introduced the use of isolated fat grafting for aesthetic breast augmentation. Since this revelation, breast surgeons have begun to use fat grafting in combination with implants to improve aesthetic outcomes, particularly in thin patients with inadequate soft tissue coverage.
Material and Methods
Before one can embark on any surgical procedure, appropriate patient selection must take place. This includes assessment of medical conditions such as diabetes and coagulation disorders and whether the patient is a smoker. In addition, we do not recommend fat grafting in patients with a personal or family history of breast cancer. During the consultation, patient expectations and desires in terms of volume and shape of the breasts must be discussed.
Clinical examination is especially important in an aesthetic breast patient. In particular, the following should be noted:
Symmetry of the areolas, level of the inframammary folds, and volume of the mammary glands
Preexisting rotation of the chest from scoliosis or pseudoscoliosis; failure to recognize this will result in obvious breast asymmetries
Breast base diameter, which helps to determine prosthesis selection
Nipple-to-clavicle distance (this is typically 14 to 16 cm, depending on the patient’s height)
Areola-to-inframammary fold distance to help in selecting an appropriately shaped implant (for a natural-appearing result, this distance should be at least 7 cm)
Following patient selection, one must select an appropriate implant. CBA allows the surgeon to sculpt the shape of the breast through the use of fat grafting. Subsequently, specific anatomic implants are less frequently used. In other words, round implants can be used in the overwhelming majority of cases, thus avoiding the consequences of implant rotation, while the anatomic shape can be provided with the addition of fat grafting. In my practice, before the introduction of CBA, anatomic implants were used in 50% of cases, whereas now we use them in fewer than 10%. Approximately 10% of patients will present with a reduced areola-IMF distance of less than 3 to 4 cm, and in these women, anatomic implants are recommended.
In selecting the correct implant, one must consider both the breast diameter and the desired breast projection. Projection corresponds to the desired cup size; breast diameter is measured by determining the expected breast width. To appreciate the implant volume required to achieve a certain cup size, it is useful to know that for a given patient who presents with an A cup, an implant projection of 3 cm will result in a B cup, a 5 cm implant projection will convert to a C cup, and a 4 cm projection will provide the patient with a result in between the two.
The CBA procedure is performed with the patient under general anesthesia. She is initially positioned according to which areas have been determined as harvest sites for lipoaspirate. For example, if fat is to be harvested from the buttocks or posterior thighs, the patient will initially be in the prone position. If sufficient fat can be attained from the abdomen or anteromedial thighs, the entire procedure can be performed with the patient in the supine position.
The infiltrate for analgesic and liposuction purposes should contain a long-acting analgesic (lidocaine) and epinephrine, mixed in normal saline solution. The fat is then harvested using a 3 or 4 mm diameter cannula. The resulting lipoaspirate is washed and decanted, then distributed among 10 cc syringes for later infiltration.
Preparation for implant insertion can now take place. I use a transaxillary approach, so the patient is positioned with her arms in 45 degrees of shoulder abduction and 90 degrees of elbow flexion. The use of arm boards may be required.
A 4 to 5 cm L-shaped incision is made in the hair-bearing skin of the axilla, and a thick flap of skin and subcutaneous fat is elevated. The lateral border of the pectoralis major muscle is identified after careful dissection. The premuscular subfascial plane can then be entered and the implant pocket created, as described by Graf et al 5 and Góes and Landecker. 6 An illuminated retractor is useful during pocket dissection because it allows visualization at all times. This ensures adequate hemostasis as well as accurate assessment of the dimensions of the pocket.
To ensure aseptic conditions, surgical gloves are changed immediately before the implant is placed. The implant is handled for a minimal time and is bathed in an antibiotic solution (gentamicin).
The operation concludes with multilayered wound closure. Fascia is closed with a 3-0 monofilament suture, the subcutaneous layer with a 4-0 slow-resorbing suture, and the intradermal layer with a rapidly resorbing 4-0 suture.
At this stage, fat grafting may commence. The goal is to camouflage the borders of the implant, especially the superior and medial borders, which might otherwise be visible in thin patients. A stab incision in the medial aspect of the IMF and another in the superomedial edge of the areola allow sufficient access. Grafting is performed in a radial direction in the subcutaneous plane. Care must be taken not to violate the implant pocket. The cannula used for these injections is 15 cm long and 1.2 mm in diameter. The details of fat transplantation are summarized in Table 38-1.
Average amount harvested (range) | 550 cc (150 to 2000 cc) |
Average amount injected (range) | 125 cc (100 to 250 cc) |
Number of procedures performed | 199 |
A compressive bandage is applied and worn overnight. It is then replaced the following day with a medical bra that is to be worn continuously for 3 weeks to ensure maximal engrafting of fat and to maintain implant position.
Results

This is a superior intraoperative view of a patient undergoing CBA. One can see the powerful effect of fat grafting on the right breast; the contours of the implant are not visible, and the breast’s contour and cleavage are improved.
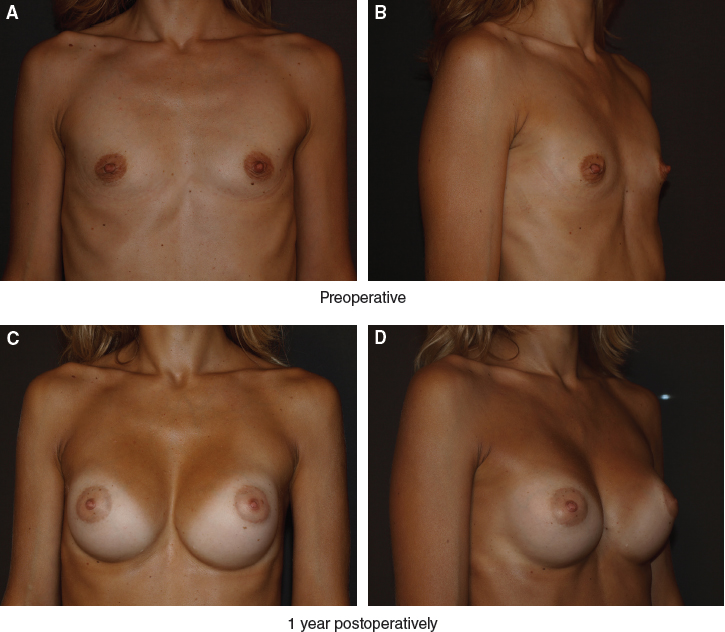
This 28-year-old patient presented with obvious breast hypoplasia. She underwent breast augmentation with 240 cc round implants placed bilaterally in a subfascial plane through a transaxillary approach. In addition, 70 cc of fat was grafted into each breast.
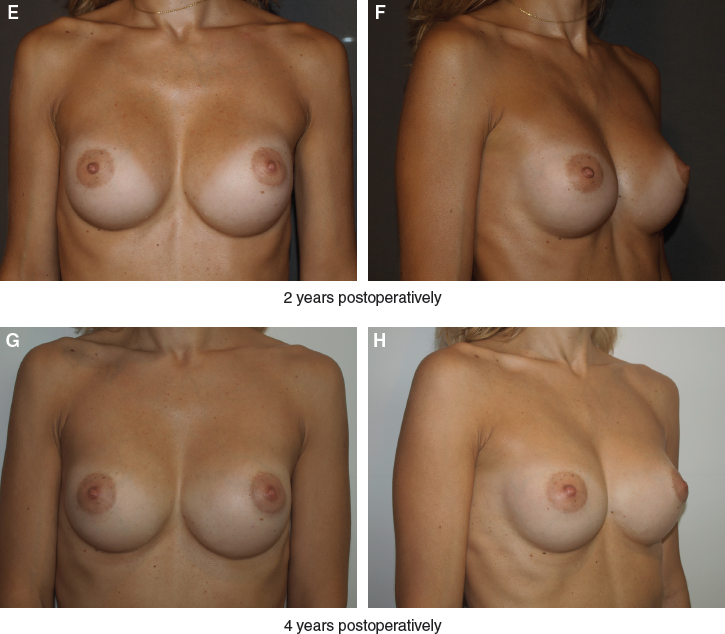
One can appreciate the stability of these results at 1, 2, and 4 years postoperatively, with no further lipo-filling required over this period.
The reasons only 10% of cases are appropriate for fat-only augmentation are twofold: (1) the necessity of harvesting at least 1 L of fat to provide sufficient fat to augment breast volume, and (2) an inability to provide more than a one-cup increase in size when harvest site volumes would be inadequate. Although the typical patient presenting for breast augmentation has a slender physique, a low BMI is not a contraindication for CBA. In fact, only 200 cc of fat is required to camouflage implant visibility and improve breast shape, as can be seen. One of the most noteworthy benefits of CBA is the concomitant liposculpture, a side effect welcomed by patients.

This patient had a significant weight loss of 50 kg that led to breast atrophy, ptosis, and skin excess. She underwent CBA in which 360 cc round implants were placed, and 120 cc of fat harvested from the thighs was grafted in each breast. She is seen 1 year postoperatively. CBA is particularly useful in augmentation mastopexy, where skin tightening is one of the main goals of the operation, the second aim being to provide volume. Through the use of fat grafting in the subdermal layer, CBA allows skin tightening by providing additional coverage between the implant and skin.
Between 2006 and 2013, we performed CBA on 199 patients. The data obtained from this group of patients are summarized in Tables 38-2 and 38-3.
Total number | 199 |
Age (average, range), years | 35 (20 to 76) |
Weight (average, range), kg | 53.7 (45 to 65) |
BMI (average, range) | 18.9 (16 to 22) |
Implant volume (average, range) | 270 cc (150 to 850 cc) |
Round | 100 |
Anatomic | 99 |
Related posts:
 Chapter 37 FAT GRAFTING FOR BREAST AUGMENTATION IN ASIANS
Chapter 37 FAT GRAFTING FOR BREAST AUGMENTATION IN ASIANS
 Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


