Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Throughout the history of plastic surgery, autologous tissue has been the preferred material for reconstructing traumatic or congenital defects or augmenting the face or body for cosmetic purposes. 1 Since 1895, surgeons have reported transplanting autologous fat to the breast as a means to enlarge, reshape, or reconstruct the breast. 2 In 1912 Eugene Holländer described the first injection of fat into a breast for the correction of a depressed, adherent breast scar (see the Introduction of this book). In the early twentieth century, Lexer reported fat grafting into breasts with an excellent, natural-appearing result that was still present 3 years later. 3 By the middle of the last century, surgeons began describing the use of fat grafts for cosmetic augmentation of the breast. 4 , 5 In their atlas of procedures, May et al 6 demonstrated fat grafting to the breast for purely aesthetic augmentation. Although good long-term results from transplanting autologous fat to the breasts were described in the past, by the 1970s silicone and saline breast implants began to overshadow autologous tissue augmentation.
In the early 1980s, liposuction provided a new source of autologous tissue, and surgeons soon described placement of this fatty tissue into the breast. 7 – 10 However, in 1987, a position paper by the American Society of Plastic and Reconstructive Surgeons (ASPRS) Ad-Hoc Committee on New Procedures issued an opinion that fat grafting to the breast might interfere with breast cancer detection and therefore should not be performed 11 (see Chapter 40). The result was that grafting to the breast was condemned by the position paper, because the procedure might result in mammographic changes—something that every single surgical procedure to the breast can create. This position paper in essence created a worldwide moratorium on fat grafting to the breast. As a direct result of the 1987 position paper by the ASPRS, fat grafting to the breast was rarely performed from 1987 to 2007.
With the safety concerns that arose in the early 1990s about silicone breast implants, I reviewed the literature and found that with all breast procedures there was a risk of causing mammographic changes. Also concerning was the fact that breast implants, which have been widely accepted, result in incomplete visualization of the breast tissue during mammography. With these things in mind, as well as positive experience with fat grafting and queries from my patients, I decided to rethink the idea of grafting fat to the breasts.
Between November 1995 and June 2000, I performed fat grafting to the breasts of 17 patients. Indications included micromastia, postaugmentation deformity, tuberous breast deformity, Poland syndrome, and postmastectomy reconstruction deformities. With my earliest patients I had great successes and began discussing them discreetly with colleagues as early as 1997. After lectures that I gave on fat grafting to the breast at Georgetown and Marseilles, Scott Spear and Emmanuel Delay began grafting fat to the breast. I followed my earliest patients over the next 5 to 10 years, compiled my observations retrospectively, and published them. 12 There was significant improvement in breast size and/or shape in all women treated, and all had breasts that were soft and natural in appearance and feel. Postoperative mammograms identified the changes one would expect after any breast procedure.
Based on 14 years of experience with fat grafting to the breast (and with an official moratorium still in force), I began speaking about this procedure at international meetings and was subsequently invited to present my experience in May 2006 at the ASPS meeting and published my series in March 2007. 12 After I presented my experiences at major national plastic surgery meetings in North America as well as in Europe and Asia, the ASPS was persuaded to establish a task force to scientifically reevaluate fat grafting to the breast. At the initial meeting in October 2007, the task force “reviewed the scientific literature, critically appraised the information available, and developed evidence-based practice recommendations.”
The task force report was approved by the ASPS/Plastic Surgery Education Foundation (PSEF) and the American Society of Aesthetic Plastic Surgery (ASAPS) in October 2008, which led to reversal of the earlier moratorium. This new statement confirmed that fat grafting was considered safe enough to become part of our clinical practices. The following excerpts are from this report, published in Plastic and Reconstructive Surgery in 2009 13 :
Fat grafting may be considered for breast augmentation and correction of defects associated with medical conditions and previous breast surgeries; however, results are dependent on technique and surgeon expertise…. Fat grafting to the breast could potentially interfere with breast cancer detection; however, no evidence was found that strongly suggests this interference….
Radiological studies suggest that imaging technologies (ultrasound, mammography, and MRI) can identify the grafted fat tissue, microcalcifications and suspicious lesions; biopsies may be performed if needed for additional clarification.
The position statement issued by the plastic surgery societies, along with the positive results of the increasing world experience with fat grafting to the breast, has served as a springboard for plastic surgeons to initiate more definitive studies of the procedure’s efficacy and safety.
Now a large percentage of plastic surgeons worldwide are grafting fat for augmentation and breast reconstruction, and it has become part of the standard of care. Many scientific reports have emerged on the efficacy of fat grafting for breast reconstruction, 14 – 22 for the treatment of radiation damage to the chest, 18 reduction of breast capsular contracture, 18 and soft tissue coverage of breast implants. 18 , 20 , 23 – 27
Indications
In this chapter I will address the aesthetic augmentation of a breast for shaping with the Coleman technique (see Chapter 1). The case I present is that of a patient with a mildly tuberous breast, which represents a special challenge by having a constricted lower pole, but the principles are basically the same as in fat grafting for simple breast augmentation.
The degree of sculpting possible with Coleman fat grafting is clear when applied to women who have tuberous breast deformities. In this situation, little or no no fat is placed under the nipple-areola complex, while the skin envelope of the breast is selectively expanded with fat placed immediately beneath the skin. Fat grafting is thus able to change the relative proportion of the breast to the areola, creating a more natural-appearing and shapely breast.
In patients with breast asymmetry, fat grafting allows either dramatic or subtle shaping to produce a more aesthetic, symmetrical contour. These small changes are very difficult to achieve without the use of transplanted fat. Fat grafting to the breast is a valuable adjunct to breast reconstruction (see Chapter 40), and with or without alloplastic breast implants, grafting may provide a substitute for much more extensive procedures, such as free flaps.
Patients with deformities resulting from their breast implants often have inadequate soft tissue coverage over the implants and/or obvious capsular contractures. Grafted fat can provide additional subcutaneous thickness to disguise visible edges and wrinkling of implants and decrease the palpability of the underlying implant. This is especially true in thinner patients. In addition, the placement of fat around breast implants can result in a softening of the breast capsules, which has also been reported by Delay et al 16 and Rigotti et al. 18
Material and Methods
TECHNICAL GUIDELINES
Preparation
Harvesting sites are selected only to enhance body contour and avoid iatrogenic donor site deformities, since no overriding clear correlation between donor site location and longevity of the implanted tissue has been demonstrated. 28 , 29 I prefer to harvest fat from the torso, especially the back, love handles, and abdomen, because a reduction in these areas enhances a woman’s body proportion and accentuates the larger breasts with a narrower waist.
Anesthesia
I usually use a general anesthetic or propofol because of the large volumes that must be harvested for fat grafting to the breast. I infiltrate a solution of 0.2% lidocaine with 1:400,000 epinephrine in Ringer’s lactate solution into the donor and recipient sites.
Incisions for Harvesting
Incisions are made with a No. 11 blade scalpel, and a blunt nine-holed Coleman harvesting cannula is used to diffusely inject Ringer’s lactate solution with 1:400,000 epinephrine in a ratio of 1 ml of solution for each 1 cc of fat harvested. For the posterior torso, I usually make one incision in each sacral dimple and one incision in the midline of the back. These may be supplemented by incisions laterally to facilitate harvesting in the hip or flank.
From the anterior approach, I most often place incisions in the pubic hair and umbilicus, with occasional incisions in the flanks or hips to facilitate removal from the more lateral regions.
Cannulas for Harvesting

Fat is harvested in most of the cases with a 10 cc syringe attached to a nine-holed, blunt-tipped Coleman harvesting cannula. The larger-gauge cannula is used here. A combination of slight negative pressure and a curetting action allows parcels of fat to move through the cannula, through the Luer-Lok aperture, and into the barrel of the syringe, resulting in minimal mechanical damage to the fatty tissue.
Harvest
After harvesting, the fat is centrifuged in the 10 cc syringes for 3 minutes at 1300 g. The oil layer is decanted and the aqueous component drained. Codman pads are used to wick off the remaining oil, and the refined, unwashed fat is then transferred to 3 cc Luer-Lok syringes.
Incisions for Infiltration
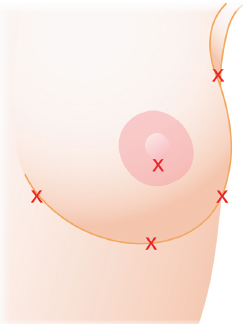
The incisions are positioned to allow placement from two directions into each area to be grafted. Usually three inframammary incisions, an areolar incision, and an axillary incision on each breast are enough to provide access to the entire breast. Incisions on the sternum, décolleté, or surface of the breast should be avoided.
Cannulas for Placement
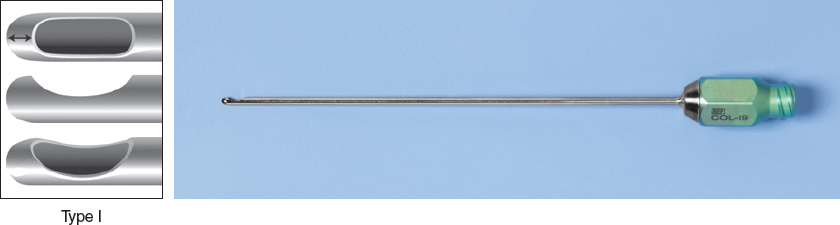
Blunt 17-gauge infiltration cannulas, 9 or 15 cm in length, are used to place the fat through 2 mm incisions. Blunt cannulas not only allow more dispersion of the grafted tissue in small aliquots, but also reduce the possibility of an intravascular injection. 30 A type I Coleman cannula is most often used, but if there is scarring or other tissue resistence, a type II or even type III Coleman cannula may facilitate the surgeon’s ability to push the cannula through the denser tissues such as scars and breast parenchyma.
For safety reasons to avoid intravascular emboli, at no time are sharp needles used for injection into the breast. The fat is infiltrated only while the cannula is being withdrawn, not during the advancement of the cannula. Approximately 0.2 cc is placed with each withdrawal of the cannula. This approach maximizes the surface area of contact between the surrounding tissues and the grafted fat. The goal is to allow each parcel of fatty tissue access to a blood supply, thus maximizing the potential for survival and minimizing the possibility of fat necrosis. Also, for safety reasons, cannulas of more than 15 cm in length should be used with extreme caution, because pneumothoraxes have been reported by even the most experienced surgeons while infiltrating fat in the thorax.
Method of Infiltration
The Coleman technique used for placement must be one that facilitates survival of the fatty tissue, not only by minimizing trauma during harvesting and refinement, but also by placing the living tissue in a manner that optimizes the potential for vascularization. When fat is placed into the recipient site in large clumps, some of the fat cells may be too far from a blood supply. This can lead to fat necrosis, causing not only lumps and calcifications, but also the formation of liponecrotic cysts. Bircoll 7 advocated the placement of fatty tissue in amounts as small as 1 mm per pass. At the time, the idea of making 130 passes in the breast to place 130 cc of fat was considered “ludicrous.” 31 , 32 The technique described in this chapter is based on an even smaller aliquot, with each pass of the cannula depositing from ⅕ to ½ cc per pass, depending on the length of the deposited path. Dramatic volume corrections are possible, but the time requirement for such a procedure should not be underestimated. The time to harvest, refine, and place fat into the breasts in this fashion takes many hours. In general, placement of fatty tissue into the breasts using this method takes approximately 2 hours for the first 100 cc and approximately 45 minutes for each additional 100 cc placed.
Level of Infiltration
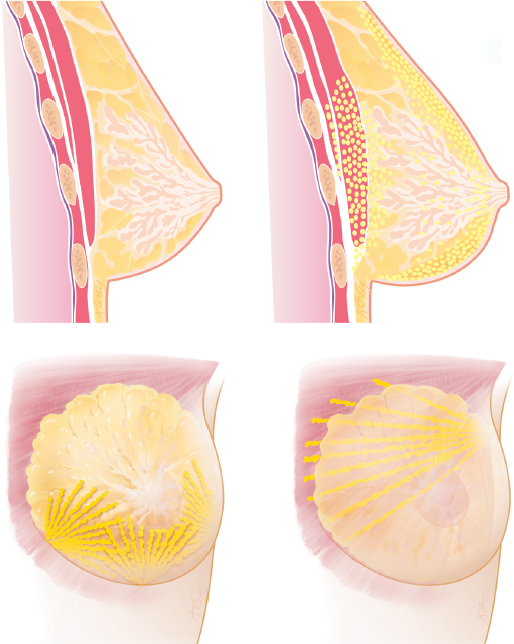
The breasts are shaped by layering the fat into different levels until the desired contour is achieved. Although a breast implant augments by expanding the retromammary or retropectoral space, the structural fat grafting technique allows selective augmentation and contouring from the chest wall to the skin. In most of my earlier cases, the largest portion of the fat was infiltrated into the pectoralis major muscle, followed by infiltration into the retropectoral and prepectoral spaces. Those volumes were located close to the chest wall and provided a diffuse increase in the chest size without specific shaping. Shaping of the breast is accomplished by placing aliquots subcutaneously into the superficial breast planes. Placement into the parenchyma of the breast should be limited but is necessary at times to increase projection.
Volume Ranges
With structural fat grafting, corrections with as little as 50 cc to more than 400 cc of fat grafted diffusely in the breast and surrounding tissues produce long-lasting results. The amount placed always depends on the effect desired. As with any surgical procedure, the technique used, the execution of the technique, the experience of the surgeon, and even variations between patients affect the outcome.
TECHNIQUE
A basic strategy of the fat grafting technique is the placement of fat in small aliquots rather than large clumps. Minimizing the amount of fatty tissue grafted with each pass of the cannula maximizes the surface area of contact between the grafted fat and the recipient tissue. Decreasing the size of each injected volume of fatty tissue decreases the distance of the innermost fat cells to the surrounding capillaries. The proximity of the newly grafted fat to a blood supply encourages survival and minimizes the potential for fat necrosis and later calcification.
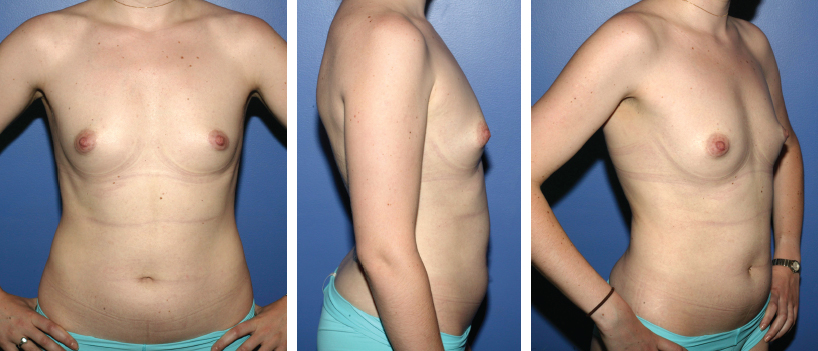
This 27-year-old woman presented for primary breast augmentation with autologous fat. She had undergone reconstruction for tuberous breasts elsewhere 5 years earlier, but she was not happy with her small breast size. She wore an external vacuum expansion device for 8 hours a day for 4 weeks before surgery to maximize the tissue envelope for fat placement. Her preoperative mammograms showed scattered benign calcifications, probably related to her previous surgery. Because the tuberous condition had been previously treated, the preoperative markings were no different from those for a typical “normal” patient.
Planning
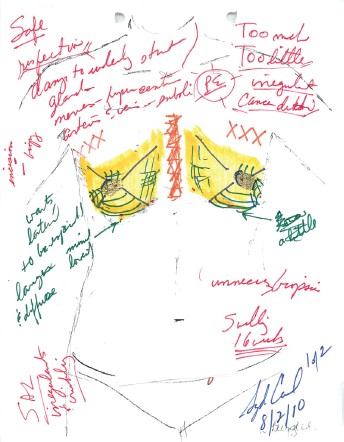
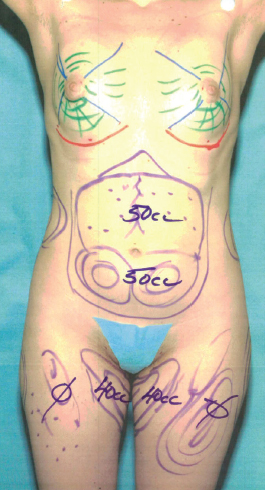
The goal was to create a fuller, natural teardrop shape by placing fat into each quadrant of the breast (focusing on the more deficient medial and inferior areas) as well as into the cleavage, and the retroareolar space (for projection). We marked donor sites (purple marker) in the love handles, posterior hips, sacrum, posterior medial thighs, lateral thighs (all approached from the prone position) as well as the upper and lower abdomen and anterior and medial thighs. The breasts were divided into four quadrants, and the areas for placement were delineated with green marker. The inframammary folds were marked in orange.
Anesthesia
A general anesthetic was used for this patient, with a laryngeal mask airway (LMA). The donor sites were infiltrated with 1:400,000 epinephrine in Ringer’s lactate solution and 0.2% lidocaine (about 500 ml total was used in the donor sites).
Donor Sites

The donor sites were chosen to enhance the patient’s feminine shape by removing most of the harvested fat from the area of the waist down to the hips and up to the breasts.
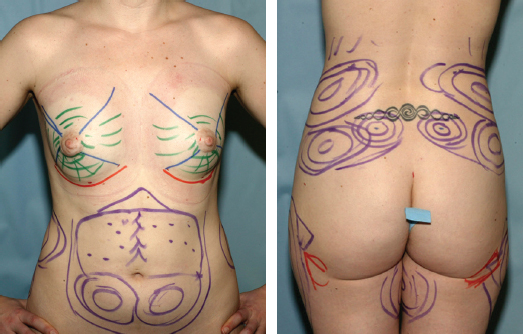
Purple marks the areas to be removed, red marks possible incision sites, and orange indicates areas in which care was necessary to avoid excessive removal, such as the transition zone between the back and the love handles.
Harvest
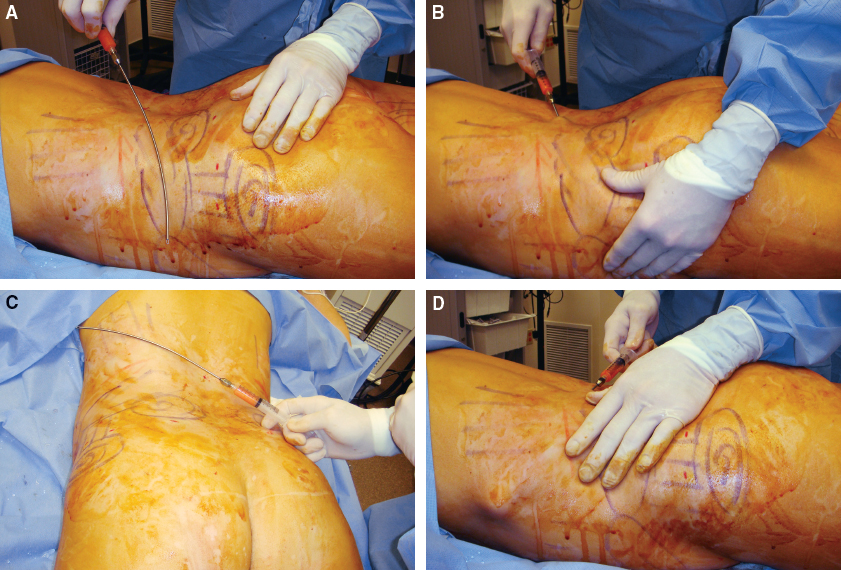
When a midline back incision and a curved 23 cm cannula are used, the entire love handles and flanks can be approached without lateral incisions.
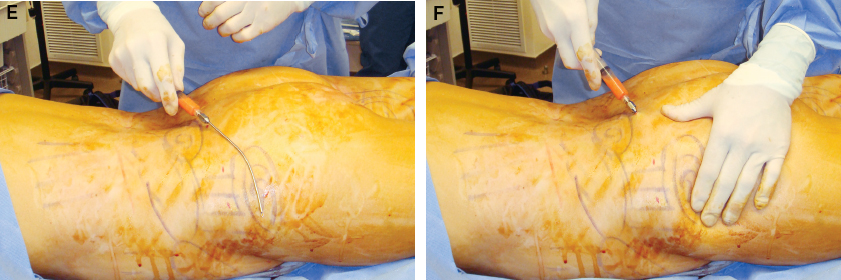
The incisions in the sacral dimple can be used to harvest not only from the sacrum and lumbar regions, but also from the hip and flank.
Surgery began with the patient in the prone position, after successful induction of anesthesia and placement of an LMA. The patient was maintained under deep intravenous sedation and breathed on her own. After infiltration with tumescent solution (Ringer’s lactate solution with epinephrine 1:400,000 and lidocaine 0.2%), using blunt Coleman multiholed cannulas, the following volumes were removed with manual suction: right love handle, 170 cc; left love handle, 210 cc; right hip, 100 cc; left hip, 70 cc; right sacral dimple, 70 cc; left sacral dimple, 70 cc; right medial thigh, 50 cc; left medial thigh, 50 cc; right lateral thigh, 100 cc; and left lateral thigh, 120 cc, for a grand total of 1010 cc. The fat was processed in the standard fashion, separating out 2.5 cc aliquots based on density. The fat was noted to be fibrous. (This is a common finding in healthy, fit patients.) The incisions were closed with 5-0 Ethilon interrupted sutures.
The patient was carefully turned to the supine position and reprepped and draped for further suction. A total of 50 cc was removed from the upper abdomen, 50 cc from the lower abdomen, and 40 cc from each medial thigh, yielding a total of 180 cc harvested in the supine position. (We did not suction the preoperatively marked anterior thighs, since sufficient volume was obtained without using this area.) The donor incisions were closed with interrupted 4-0 Ethilon sutures. The grand total volume harvested (from both prone and supine positions) was 1190 cc, and processing yielded 615 cc of usable fat.
Volumes to Be Placed
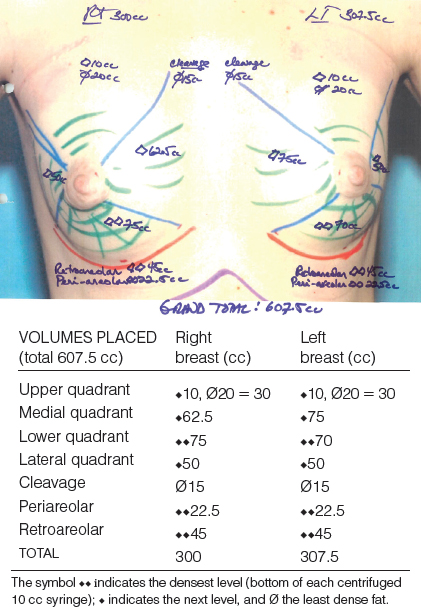
The chest was then prepped and draped in the usual sterile manner. Stab incisions for placement of fat were made in the medial, lateral and central inframammary folds (as indicated by red dots in the preoperative markings), as well as in the upper medial areolas. The breasts were infiltrated with a small volume of the tumescent solution to reduce bleeding. Using blunt Coleman placement cannulas, a total of 300 cc was placed into the right breast/cleavage, and a total of 307.5 cc was placed on the left side.
Placement
The decision about what level of fat density to use in an area is based on whether one is looking to improve texture, or just create volume. Almost any level of density can be used in the breast, unless scars are being treated—high-density fat is preferred for treating scars. In this case, the higher-density fat was used in the lower quadrants and retroareolar areas, where the most significant structural changes were planned.
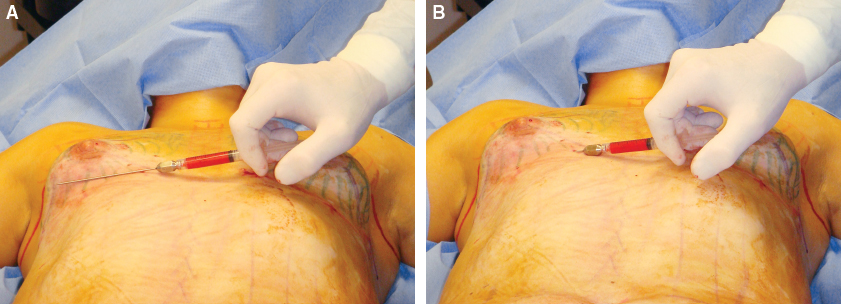
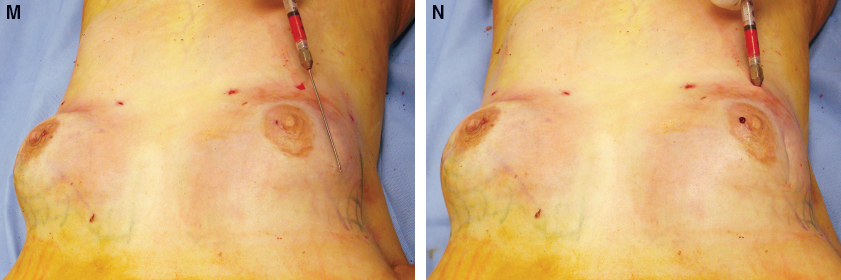
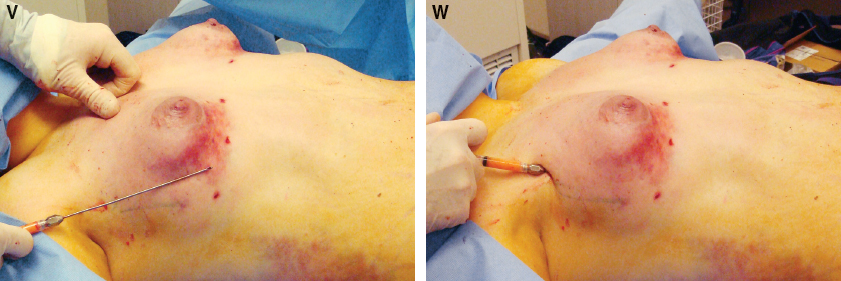
On almost every patient I begin with placement into the lower pole, but in this particular patient it was especially important, because this was the most important shaping that would take place in her breast. The placement began against the dermis from the medial incision with a 9 cm Coleman type I cannula, switching to a 15 cm cannula on occasion.
After placing 20 cc from the medial incision, I switched to the lateral incision for placement into the same area of the lower pole of the breast.
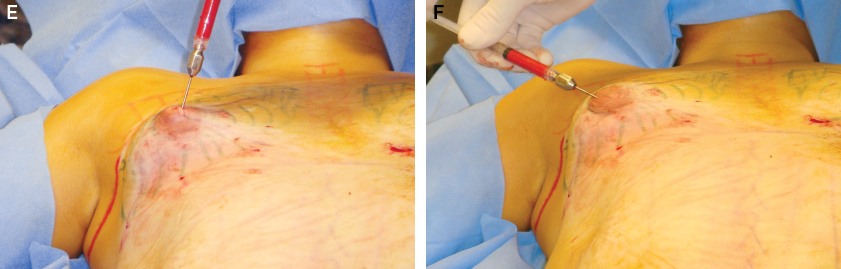
After another 20 cc of fat was infiltrated from the lateral incision, I approached the same area from the areolar incision. From all three incisions, fat was placed over the entire lower quadrant, with special attention in this patient to placement that would lower the inframammary fold to the new location several centimeters below the current location.
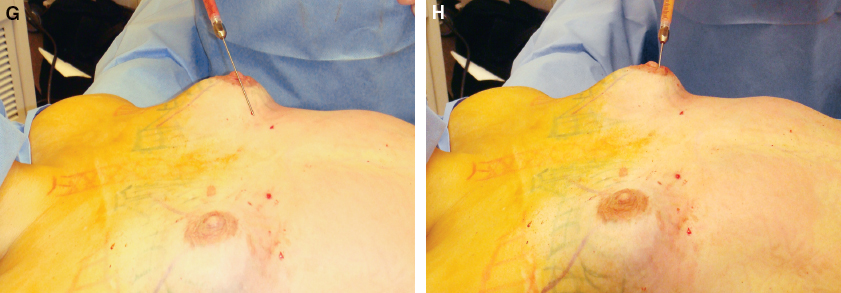
After 60 cc of fat was placed into each lower quadrant, the medial quadrants were infiltrated from the areolar, medial, and middle inframammary incisions. Again, all placement was subcutaneous. The medial quadrants were felt to be remarkably deficient, so larger amounts were infiltrated here (right, 55 cc; left, 50 cc) than was planned for the lateral quadrants.
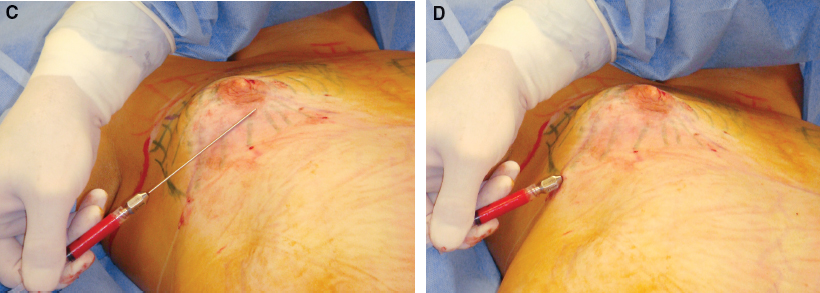
Next the lateral quadrant was infiltrated through the lateral inframammary incisions with a significantly smaller quantity of fat.
This placement extended up into the axilla to fill in the defect created by the interface of her large pectoralis muscles with her small breast.
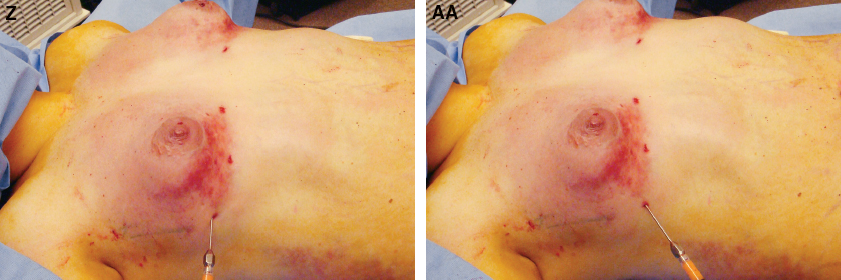
The lateral quadrant was also approached through the middle inframammary fold incision. The placement remains superficial, especially in this patient, to attempt to correct the tuberous deformity. Note the dimpling of the skin as the cannula passes superficial to the skin.
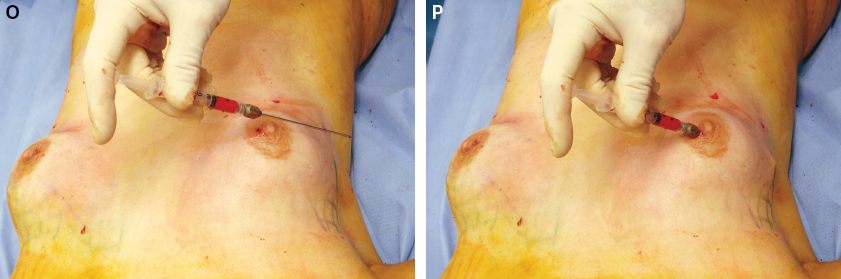
Even with the small amount placed into the lateral quadrant, the fat is infiltrated from three different incisions and presumably three different directions. Every attempt should be made to place the fat aliquots in small quantities with each pass and from at least two and even three directions when possible.

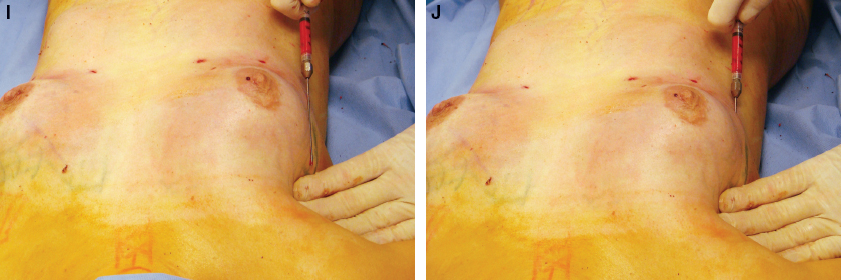
Switching to a 15 cm cannula extends the reach so that distant areas can be infiltrated with fatty tissue in several directions.
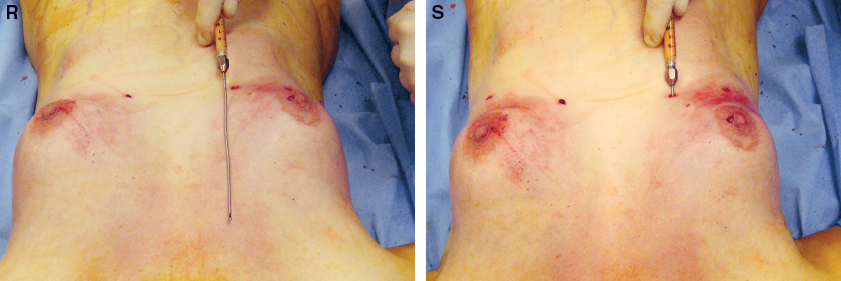
Finally, the lateral sternum cleavage area was approached. A 15 cm infiltration Coleman type I cannula is always used in these cases to reach the distant site. In this patient, 40 cc was placed on each side. This amount is about the usual for most patients.
The area was approached from the areolar incision with a 15 cm type I cannula to provide another direction of placement.
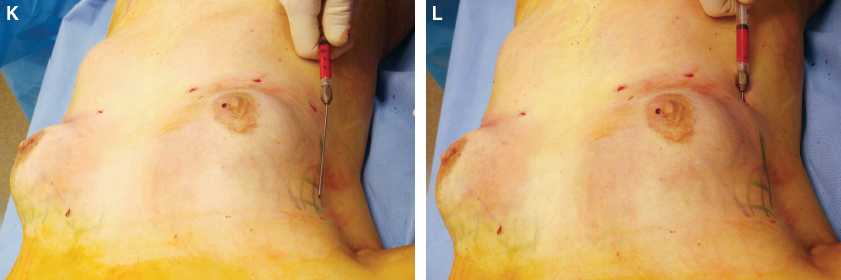
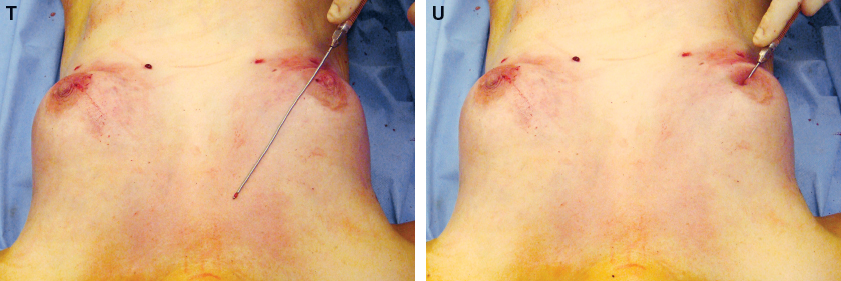
After placement was complete into all of the sites, some tissue was placed into the retromammary region. Axillary incisions facilitated finding the plane behind the breast. In this patient, 85 cc was placed on the right and 60 cc on the left in the lower half of the breast; into the upper half of the breast in the retromammary region, 70 cc was placed on the right and 43.5 cc on the left.

All of the incisions were used for this deep placement in the retromammary space with 15 cm 14-gauge type I cannulas. The larger cannulas are used for safety, because the stiffer, bigger cannulas allow greater control in placement. Recently I have begun using the old Coleman harvesting cannulas (bucket-handle type) for placement in this plane and around breast implants.
After fat placement into all of the planned areas, the patient was brought to a sitting position. We determined that her breast projection was deficient, and it did not appear that the lower poles had as much curvature or pseudoptosis as had been hoped.
Through the axillary incision and the other four, another 35 cc was placed into the constricted right lower pole and another 30 cc into the left lower pole. This was an extremely difficult placement, because there was not much space, and several times it was debated whether we should release the apparent adhesions in these areas to allow more curvature of the lower pole. I felt that this would destabilize the fat I had already placed and would probably not allow me to place more fat in a vascularized, healthy fashion. Therefore no release of any sort of adhesion or constriction was performed. However, to enhance projection, 30 cc was placed on the right and 10 cc on the left deep in the parenchyma. No tissue was intentionally placed behind the areola at any time.

Several times during the procedure, the patient is placed in a sitting position to evaluate the effect of the fat transplantation. In these views, taken toward the end of the procedure, one can see the beginning of a release of the constricted lower pole. More placement simply was not possible into the stiff lower pole.
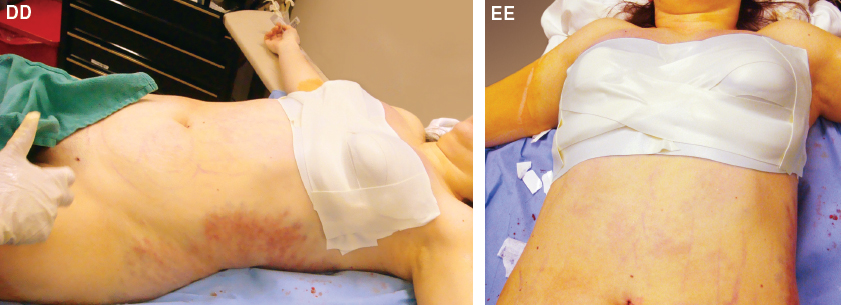
The breast incisions were closed with 5-0 Ethilon sutures. Reston foam was placed over the inframammary folds and between the breasts to prevent migration of fat. Compressed Reston foam was also placed over the areolas to prevent herniation, since the patient had a history of tuberous breasts. The Reston foam was secured with compression in all places with Tegaderm. The surgical bra cushioned with Kerlix was placed, as was a lower body compression garment.
The patient was seen for routine follow-up on the third postoperative day. We were able to attach the external vacuum expansion domes at that time. We instructed the patient to begin using the device nightly and to try to work up to 8 hours per day again. We saw her routinely during her initial postoperative course, and she was able to use the expansion device for 8 hours a day for about 4 weeks. Her postoperative course was unremarkable, and the patient was happy with her results.
Related posts:
 Chapter 37 FAT GRAFTING FOR BREAST AUGMENTATION IN ASIANS
Chapter 37 FAT GRAFTING FOR BREAST AUGMENTATION IN ASIANS
 Chapter 38 COMPOSITE BREAST AUGMENTATION
Chapter 38 COMPOSITE BREAST AUGMENTATION
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


