Chapter 19 Risk Areas
Introduction
Classification of the face according to risk areas, which is routinely used for plastic surgery and dermatological surgery studies, mainly focuses on facial innervation. However, in the case of facial filler injections, the most feared complication, and one that can have devastating consequences, is intravascular injection with embolization of the product. Consequently, in this chapter we describe the anatomical areas at risk when performing a facial filler injection.
Anatomical Areas at Risk
The areas of greatest risk are: (a) areas supplied by the branches of the internal carotid artery (ICA), (b) areas where the external carotid system anastomoses with the internal carotid system, and (c) areas where the arteries emerge from the cranial foramens.
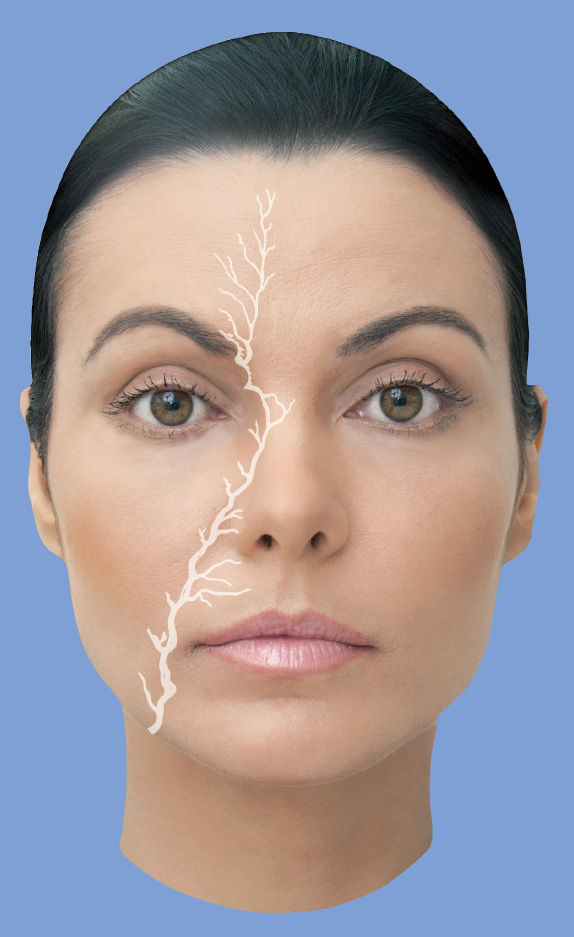
Arterial occlusion can lead to ulceration, tissue necrosis, and even amaurosis in cases of product embolization and retrograde flow into the retinal artery (Fig. 19.1). Arterial/venous occlusion can be caused by intravascular injection and by external compression of the vessel by the filler and/or edema. For more details, please (see Chapter 18).
Frontal Region
This area is vascularized by the supraorbital and supratrochlear arteries, and by the frontal branch of the superficial temporal artery (STA), which are found in the subcutaneous tissue and are also entwined in the frontal muscle.
We recommend using the supraperiosteal plane for injec ting with cannulas. A margin of 1.5 cm should be kept above the eyebrow to avoid compressing the supraorbital/supratrochlear nerves and their respective arteries.
The supraorbital and supratrochlear arteries are branches of the ICA, and the frontal branch of the STA is a branch of the external carotid. Despite the STA being a tributary of the external carotid, its branches anastomose with the supratrochlear and supraorbital arteries, and there is a risk of product embolization and retrograde flow into the retinal artery (Fig. 19.2). 1 ,. 2
Glabella
The glabella is vascularized by the supratrochlear, infratrochlear, and dorsal nasal arteries. It is a high-risk area because the vessels at this location are small and collateral circulation is scarce. Moreover, in case of intra-arterial injection, there is a risk of retrograde flow, with occlusion of the central retinal artery (CRA).
Hong et al reported a case of amaurosis and paresis of the contralateral upper limb caused by an autologous fat injection into the glabella. 3 The intravascular material embolized in the retinal artery and the central cerebral artery because of high injection pressure. These types of cases have to be treated as medical emergency. 3 ,. 4
To correct superficial wrinkles that persist after injection of botulinum toxin into the corrugator muscle, we recommend injecting low-elasticity hyaluronic acid (G′) into the intradermal plane, in microdroplets, after prior aspiration. However, we recommend the supraperiosteal technique (Fig. 19.3), with a cannula, for volume replacement following bone remodeling and resorption of local fat. For more details, please see Chapter 9. 5 ,. 6
Nasal Dorsum
The nose is supplied by the internal and external carotid arteries. The nasal dorsum is irrigated in its superior portion by the dorsal nasal artery (DNA), which is the terminal branch of the ophthalmic artery (OA). It emerges from the orbit above the medial palpebral ligament and, after branching to the upper part of the lacrimal sac, divides into two branches: One crosses the root of the nose and anastomoses with the angular artery (AA) and the other runs along the nasal dorsum, supplying its outer surface, and anastomosing with the artery on the opposite side and with the lateral nasal branch of the facial artery (FA).
Consequently, the nasal dorsum is the riskiest area for filler injections of the nose. Inferiorly, the nose is vascularized by the branches of the external carotid and the lateral nasal artery, which is a branch of the FA. The columella is supplied by the branches of the superior labial artery (SLA). The tip of the nose is supplied by the branches of the lateral nasal artery, DNA, and SLA (Fig. 19.3).
Nasolabial Fold
The nasolabial fold is supplied by the FA and its branches. The AA is the terminal part of the FA, and receives this name after dividing into the SLA. It ascends in the direction of the medial angle of the orbit in the midst of the levator muscle fibers of the upper lip and the ala of the nose, accompanied by the angular vein (AV) more laterally. Its branches anastomose with the infraorbital artery (IOA) and then, after supplying the lacrimal sac and the orbicularis oculi muscle (OM), end by anastomosing with the dorsal nasal branch of the OA. In the extension of the nasolabial fold, the artery is in the subcutaneous plane; therefore, the most recommendable application plane is the deep dermal plane. If a needle is used in the piriform aperture, the supraperiosteal plane is recommended, whereas if a cannula is used, the subcutaneous plane should be preferred (Fig. 19.4).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


