Chapter 13 The Technical Use of Croton Oil Peels
The only source of knowledge is experience.
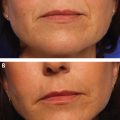
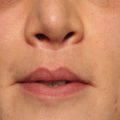
A E
PATIENT EVALUATION AND SELECTION
When patients present for facial rejuvenation, the surgeon must resist the temptation to categorize them into specific surgical procedures. As previously discussed, surgeons have a tendency to ignore the textural aspect of aging, but it is an integral component of the complete picture. Moreover, many patients give greater importance to improving obvious wrinkling and skin imperfections rather than sagging and jowling. The surgeon may see a “facelift” while the patient expects improvement in the perioral wrinkles. The disappointment and hostility when a costly procedure has done nothing to improve the lip lines is best prevented by really listening to the patient and having an honest discussion.
In reality, many patients can benefit from both structural (repositioning and volume) and qualitative improvement of texture. If the patient is amenable to comprehensive rejuvenation, it is logical to proceed with the surgical intervention first, because some indirect improvement in the texture of the central facial skin can be seen with gentle tension. After a waiting period of 4 months, a peel can be done to correct the remaining issues. The concept of peeling (or lasering) at the same time as a facelift is controversial because of the obvious dangers, but a limited role may be feasible and warrants further study.
Patients who are averse to surgery or simply want improvement in wrinkling and texture provide an interesting perspective for surgeons. After a well-done peel, many of these patients are delighted by the result and see the remaining structural issues as “normal” aging. Thus surgeons should refrain from interjecting their personal bias (and potential self-interest) in the planning.
INDICATIONS AND CONTRAINDICATIONS
The main contraindication for a croton oil peel is a patient who is expected to be noncooperative with the postoperative care or to pick the skin in early recovery. A relative contraindication is a patient with widespread actinic keratosis, in whom the peel may go too deep. These patients are candidates for staged lighter peels.
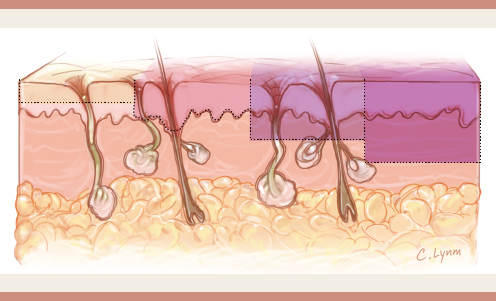
Once the decision has been made to proceed with resurfacing, the patient assessment is a tool for creating an aesthetic treatment plan. The first factor to consider is ethnicity: Light-eyed, light-skinned individuals have thin, translucent skin that is more susceptible to sun damage and extrinsic aging with well-defined and prominent wrinkling, solar elastosis, and dyschromias. Asians and subcontinent Indians have thicker, better quality skin with less wrinkling but are prone to pigmentary changes. Black skin, with its greater melanin composition, demonstrates a remarkable resilience and does not seem to age.
Gender is also a factor; males exhibit less wrinkling in the middle and lower face, possibly because of thicker skin and factors relating to the beard and frequent shaving. Histologically, male skin has a greater proportion of sebaceous glands. Significant peeling in men is centered on the forehead and periorbital area.
An assessment is made of obvious dynamic lines that occur perpendicular to the direction of the muscle fibers that created the motion. In the upper face, these include the horizontal forehead lines caused by frontalis contraction, vertical glabellar lines from the corrugator supercilii, horizontal lines from the procerus, and radial crow′s feet lines from the orbicularis oculi. The procerus lines commonly extend onto the dorsum of the nose. The lateral brow can also exhibit passive oblique rhytids described as “sleep lines.”
The lower eyelid deserves special attention when considering peeling. The lower eyelid skin is very thin, with the thinnest dermis in the body and a lack of supportive subcutaneous fat. The lid itself is suspended by its medial and lateral tendinous connection to bone, leaving the central portion dependent. With frequent contracture of the orbicularis muscle and prominent exposure to the sun, the lower eyelid skin is typically the first place to show signs of aging, crepiness, crisscrossing, and, as a late change, skin redundancy. Therefore the main intervention to be considered should be resurfacing rather than skin excision unless clearly indicated. Specific details of lower eyelid surgery are discussed later.
By contrast, the upper eyelid skin fares better, because it has more superficial subcutaneous tissue and the lid is physically supported by the eyeball. The result is that textural issues are less important, making upper blepharoplasty a good option. Nonetheless, the “shrinking” quality of peeling can elicit a good effect in the upper lid.
Recent anatomic studies by Bryan Mendelson have led to greater understanding of the process of facial aging and by extension to the changes of the skin of the middle face. Mendelson described that the tissues overlying the parotid gland are densely attached by a multitude of ligaments anchoring all layers and preventing motion over the years. Examination of the skin in this region reveals relatively little wrinkling, and this needs to be kept in mind when peeling. Anterior to the parotid, the ligaments become more sparse and specifically arranged to allow fine movements. This decreased support is the root cause of centrofacial aging. This change in ligamentous support has repercussions on the skin as the cheek skin medial to the parotid shows stippling and crosshatching that does not follow a pattern of dynamic movement.
The nasolabial fold is a crease, not a wrinkle, and therefore is not necessarily improved by peeling. However, if a superficial line remains etched on the skin when the cheek substance is gently retracted laterally, this can be improved with peeling.
The soft tissues overlying the oral cavity, much like those over the orbits, lack underlying support and are suspended only from the periphery of the cavity to perform the necessary complex fine movements. The surface expression of this is the common and troublesome perioral lines caused by the contracture of the orbicularis oris muscle.
The oral commissures are complicated areas that lose fatty support with age, leading to irregularities and wrinkles perpendicular to the fibers of the depressor anguli oris muscle.
The chin area is more anchored but is subject to complex movement by the orbicularis oris, mentalis, and depressor muscles. The result is the transverse mental crease and irregular peau d′orange, which, although stubborn, can be greatly improved with peeling.
The earlobes age by general involution, thinning of the dermis, creasing, and elongation. Interestingly, they exhibit all three aspects of aging, and although they can be nicely improved with surgical reduction and filling, they respond very well to peeling.
Aging changes of the neck are best treated with surgery. The neck skin does not have the recuperative qualities of facial skin and cannot be peeled to improve wrinkles. Peeling of the neck is extremely light and should be used only to prevent a demarcation line at the mandible.
The relative thickness of the skin in the various areas should also be assessed. The perioral area bordered by the nasolabial and melolabial folds has the thickest skin of the face and can be deeply peeled, to the upper or midreticular dermis.
The forehead area changes from medial to lateral. The glabellar area, including the upper nose, is thicker and can be peeled to the upper reticular dermis. The lateral forehead is thinner, and peeling to the papillary dermis is more appropriate. Also, this area rarely has deep wrinkles (other than the transverse lines). Gentle pinching of the skin between the thumb and index finger, starting centrally and moving laterally, easily reveals the difference in thickness, and this correlates with the correct depth of peeling. The temporal area is thin and delicate and should be peeled with caution. Conveniently, this area rarely needs deep peeling.
The immediate preauricular area is very stable and tends not to wrinkle. This is also a delicate area, and caution is warranted. Pinching the skin as described will show that the skin is bound down and adherent over the tragus and preauricular area. Advancing medially, the skin thickens, is more mobile, and contains more subcutaneous tissue. This is clearly seen in the “cheek proper,” where affectionate pinching is done. The dividing line between the anterior and posterior face begins from the lateral canthus, curving posteriorly and then crossing the juncture of the body of the zygoma and arch, and extending to the geniomandibular border. The anterior portion of the face, being more mobile, often shows fine crisscrossing, wrinkles curving from the lateral canthus as an extension of crow′s feet, and occasional sleep lines. This area is thinner than the perioral and glabellar area; therefore the papillary dermis or upper reticular dermis is usually the limit for peels.
The lower nose is thick like the perioral area, and if needed can be peeled to a similar depth. The eyelids are an interesting area because of the thinness of the dermis but can be safely and predictably peeled with dilute solutions. The eyes are the focus of the face, and the lower eyelids are commonly the main sign of aging, especially in younger patients. Fortunately modern croton oil peels are particularly efficient in this region. Pinching the eyelid skin and continuing inferiorly to the infraorbital rim will demonstrate the change in thickness. This is also a convenient time to test for excessive laxity of the lower lid.
PREOPERATIVE PLANNING AND PREPARATION
A chemical peel is, at its core, a controlled chemical burn done in the hope of effecting an anatomic change in the dermis, namely an increased deposition of collagen and elastin in an orderly fashion. The more advanced the wrinkling and solar damage, the deeper the peel must go without causing most feared sequelae, hypopigmentation and scarring.
Chemical peeling causes a true injury followed by a significant albeit tolerable recovery. Adequate preparation of the skin and the patient are important factors in the ultimate success. The patient must be motivated and counseled to have a long-term perspective. The reward is a dramatic and lasting improvement in skin texture, which is not easily replicated by any other modality.
The immediate postpeel phase, although not particularly long, can be trying for the patient; therefore the surgeon must describe it realistically and accurately. Detailed photographs of the day-to-day recovery are shown to the patient and, if possible, to any caregiver who will be present. The prospective patient should speak or ideally meet with patients who have had a similar peel. Seeing someone in person who has successfully gone through the process is an invaluable encouragement that although the recovery is difficult, it is well worth it. Overall the peel is well tolerated and the experience is a positive one if the patient is well informed and the proper tone is set.
Preparation of the skin before the peel is a means of preventing complications such as pigmentary changes, namely hypopigmentation and hyperpigmentation. This involves applying tretinoin and hydroquinone 4%. The epidermis is stabilized, the dermis is stimulated to increase collagen content, and the melanocytes are suppressed.
On a cellular level, the stratum corneum of the epidermis is compacted, the melanocytes are suppressed, and a more even blending of pigment deposition occurs. The fibroblasts create more collagen and elastin, and angiogenesis increases the circulation in the dermis. In essence, the skin is “revved up” for the injury to come.
The preparation begins 4 to 6 weeks before peeling with tretinoin 0.05% or 0.1%, 1 inch (approximately 1 gram) applied to the whole face. The application includes the earlobes, tragus, and hairline and continues to 1 inch below the mandibular border and 1 to 2 mm below the ciliary edge. Application should avoid the upper lids to prevent possible irritation. The neck can be prepared in a similar fashion, decreasing the frequency depending on irritation.
Hydroquinone 4% is applied twice daily to suppress and regulate melanocytes. In countries where hydroquinone is regulated or banned, kojic acid is a possible substitute.
These preparatory treatments accelerate cellular turnover and result in erythematous and flaky skin, which must be accepted by the patient. If a patient is overly bothered by the reaction and wants to stop, he or she should be counseled to decrease the frequency rather than stopping. In offices in which drug compounding is allowed, a weaker tretinoin concentration (0.05%) can be mixed with hydroquinone 4% in an emollient cream and used twice a day. This has resulted in less irritation and greater patient compliance. An exfoliating agent (glycolic acid 8% or phytic acid 2%) may be used to help remove the desquamated cells in the stratum corneum. The preparation should be stopped 4 to 5 days before the peel to allow the epidermis to normalize. The preoperative clinical photographs should be obtained before this preparation to avoid the flaky, irritated appearance.
This skin preparation is certainly a nuisance, and its absolute necessity is controversial. Some practitioners successfully peel or laser resurface without it; a consensus will require greater cumulative experience and controlled studies. My experience has been that omitting or shortening the preparation leads to excessively long erythema. However, for fair-skinned, light-eyed individuals, the hydroquinone can be omitted.
Medical History
The surgeon must be aware of any previous episode of abnormal scarring. Recent use of isotretinoin (Accutane) is potentially problematic because of the inhibition of collagenase, which can lead to excessive scar formation. A 6-month waiting period is usually cited, but a true safe interim is not known. A history of herpes simplex is notable, although all patients are placed on antiviral prophylaxis.
Medications
Antiviral prophylaxis is routinely prescribed to all patients. Valacyclovir hydrochloride, 500 mg two times per day, is begun 3 days before the procedure and continued for 7 days after peeling. Although the post-peel phase is not particularly painful, narcotic pain medication is prescribed along with ibuprofen, 800 mg three times daily. Sleep medication is prescribed, and a mild sedative is a consideration to help cope with the inconvenience and isolation of the recovery.
TECHNIQUE
Peeling Without Anesthesia
The use of general anesthesia, intravenous sedation, and sensory nerve blocks has been the standard for many years, because the caustic nature of croton oil is very stimulating. Several observations, however, are notable and worth considering. There is no record of lay peelers using any particular form of anesthesia, local or general, because they were not physicians, but they nonetheless carried out significant peels. Also, unlike laser resurfacing, croton oil peels in the modern lower concentrations are not typically painful in the days after the procedure. The most significant observation is that an area of the face can be repeeled the day after (and possibly later) without discomfort. What is the cause of this phenomenon? Some clues are available by examining phenol′s other uses. Common over-the-counter sore throat sprays and cold sore solutions contain phenol at a concentration of 0.5% to 1.0% because of its inherent anesthetic property. More specifically, otorhinolaryngologists very commonly apply 20% to 25% phenol directly to the eardrum as an anesthetic to perform minor procedures in an outpatient setting.
Attempting to create a solution that would be effective on pigmented spots in the hand, I experimented with various dilutions of phenol on my own hand. The application of 60% phenol on spots caused minor stinging that promptly subsided, after which a frost appeared. The skin then darkened and remained dark for some weeks until it was shed, with improvement or disappearance of the spot. The more important personal finding was that after 10 to 15 seconds, the skin touched by the phenol was completely anesthetized, even when pricked by a needle to the point of bleeding. The biochemical explanation is that the free hydroxyl of phenol interacts with the myelin surrounding axons, resulting in a neurolytic effect that prevents the transmission of the nerve impulse. This effect is reversible, or more likely, the nerves regenerate. Historically, phenol concentrations of 35%, 50%, and even 88% have been applied to the face safely.
Based on this information and experience, I begin peeling procedures by first applying a single pass of 60% phenol to one segment of skin (such as one half of the forehead). The patient experiences mild to moderate predictable stinging for 10 to 15 seconds, after which the pain disappears completely. Once the stinging subsides, the area treated with phenol is completely numb and can be peeled, even deeply, without discomfort.
If the entire face will be peeled, it is first treated gradually with 60% phenol for anesthesia and then peeled. The stinging sensation is tolerable (less stimulating than a 20% to 25% trichloroacetic acid [TCA] peel, which is commonly performed without anesthesia), but the overall experience is improved if oral sedation is incorporated. The degree of oral sedation depends on the surgeon′s comfort level, facility, and staff available. The degree of sedation does not have to be so deep as to require oxygen supplementation, and if appropriately planned and executed patients tend not to remember the act of peeling.
The standard routine for a full-face peel involves greeting the patient, having the patient change into a hospital gown, and giving the oral sedation. The typical regimen includes lorazepam, 0.2 mg, and triazolam, 0.5 mg. Triazolam was once a common benzodiazepine sleep medication that eventually lost favor because of a significant amnesia effect. Dentists have adopted triazolam for this very reason, and it was at the suggestion of a dental colleague that I include it. Patients may fall asleep or become sleepy. They are responsive, quite comfortable, and do not require oxygen. The only inconvenience of the sedation is that it requires someone to drive the patient home. A narcotic such as hydromorphone, 4 to 8 mg, or other common analgesic can be used depending on surgeon preference and patient tolerance. Celecoxib, 400 mg the day prior and 200 mg on the morning of the peel, is useful.
The operating table or exam chair is made up like a bed with a comfortable blanket and pillow. The cardiac rhythm, oxygen saturation, and blood pressure are monitored. Pleasant, calming music is played; although the patient is watched, he or she is left undisturbed to relax or fall asleep. After an appropriate waiting period (approximately 20 to 30 minutes), the skin is degreased with acetone, and ketorolac, (Toradol) 30 to 60 mg is given IM. A first pass of phenol is applied patiently, concentrating on small areas at a time and waiting for the stinging to go away before proceeding to the next area. All areas to be peeled are treated in this way. The eyelids are treated last, because they are more sensitive. Once the entire face (or areas to be peeled) have been treated in this manner, and after the initial frosting has subsided, the surgeon can proceed with the peel, observing the patient for discomfort. If an area is particularly sensitive, local anesthesia can be injected, but it is rarely needed. The use of a cryocooler (an apparatus that blows cold air, used in laser treatments) or similar machines can be a soothing adjunct. Distraction with a vibrating device touched to the vicinity of the area being treated is also useful.
Early experience showed that at the end of the peel, a 1-hour period of discomfort and burning was common that required use of an oral narcotic. After this, patients typically have no pain. A way to manage the immediate discomfort after the peel is to apply a thin coat of a standard compounded topical anesthetic cream (“BLT,” benzocaine 20%, lidocaine 8%, tetracaine 4%). Due to the lack of an epidermal barrier, these topical agents are very effective, and a thin layer is sufficient and safe. After a short waiting period, the postpeel ointment is applied. This technique can also be used if the peel is done under anesthesia. The nerve blocks are thus avoided and the patient emerges from anesthesia comfortable. Further experience with these approaches has shown that using weaker phenol concentrations, such as 50% or 40%, are equally effective.
Benefits of an Anesthetic-Free Technique
The implementation of peeling without formal anesthesia has been transformative and represents a major advance in facial resurfacing; it simplifies the procedure and avoids the expense (and potential risk) of anesthesia. The ability to control the environment makes these peels more user-friendly and less intimidating. As a consequence, the surgeon can perform more peels in a more profitable manner.
This approach also has a conceptual safety factor, especially for novice surgeons. Because the ingredients of the peel have negligible cost and operating room expenses can be avoided, the pressure on the surgeon to obtain an ultimate result at the outset is greatly reduced. In the event of an incomplete peel, planned or otherwise, the surgeon can simply apply some phenol in the office and paint the remaining wrinkle with the croton oil solution. The recovery from this is much simpler, and sedation is not needed. This approach is ideal for correcting stubborn radial lines on the lip and texturing of the lower eyelid, where the margin of error is narrow. Surgeons can offer the “guarantee” that they will continue to treat until the patient is satisfied. This degree of latitude is invaluable for the doctor-patient relationship.
Preparation of the Solutions
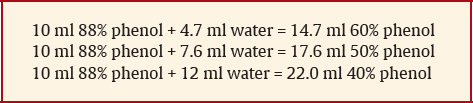
Phenol concentrations other than 88% are not typically available, but they are easily made with simple computations. In 10 ml of 88% phenol, there are 8.8 ml of phenol and 1.2 ml of water: 8.8/10 =.88, or 88%. To make 60% phenol, the compounder must use this equation to determine how much water must be added to 10 ml of 88% phenol to dilute it to 60%: 8.8/x = 0.6; x = 8.8/0.6, or 14.66. Thus to the 10 ml of 88% phenol, approximately 4.7 ml of water must be added to result in a total of 14.7 ml of solution containing 60% phenol. For 50% phenol, the computation would be x = 8.8/0.5, or 17.6; therefore 7.6 ml of water is added to the 10 ml of 88% phenol. For 40% phenol, the equation is x = 8.8/0.4, or 22, so 12 ml of water are added to the 10 ml of 88% phenol. Using these formulas, any concentration of phenol is possible.
The preparation of the acid peeling solutions is a critical step that should be performed by the operating surgeon or entrusted only to another individual who is intimately acquainted with the process. The ingredients are the same as in the Baker peel and include water, phenol, croton oil, and Septisol.1 Phenol, also known as carbolic acid, is an aromatic organic compound with the molecular formula C6H5OH. Phenol exists as a white crystalline solid that is soluble in water. The need to work with crystals to create liquid phenol possibly deterred physicians from wanting to perform peels. However, ready-made solutions of 88% or 89% phenol are now readily available from many pharmacies and dermatologic suppliers.
Phenol is a weak acid that exhibits a corrosive effect on skin by its protein-denaturing effect. It is this property that allows phenol to pass into the dermis. An interesting historical anecdote is that in the early days of Listerian sterile surgery, the entire operative field was sprayed with a fine mist of carbolic acid (described as weak), because surgeons operated with bare hands. When William Halsted′s favorite scrub nurse developed severe dermatitis because of the phenol exposure, he was despondent and sought the aid of the Goodyear brothers, who developed a practical rubber surgical glove. Soon thereafter, sterile surgical gloves became the norm, and Halsted married his nurse!
Croton oil is a natural oil extracted from the seeds of Croton tiglium, a small tree native to the Indian subcontinent and Malaysia. It is used as a veterinary purgative and has been mentioned in American literature as a poison. During World War II, croton oil was added to the alcohol propellant of torpedoes to discourage sailors from drinking the fuel (although the sailors found a way to separate the alcohol from the croton oil in makeshift stills).
Croton oil is highly caustic and if applied full strength on skin will create a painful full-thickness ulcer. When correctly diluted and appropriately applied, however, croton oil can create dramatic aesthetic results. Surgical soap consisting of hexachlorophene in a liquid form (such as Septisol) is used as a surfactant to make the aqueous components and the oil components more miscible. Ordinary tap water is used for preparation of the solutions.
These ingredients are relatively inexpensive and can be obtained from compounding pharmacies or dermatologic suppliers. Delasco is a reliable supplier in the United States and can ship internationally. Shipping croton oil overseas can be problematic because of local regulations, so inquiries to each country′s customs department should be made.
The preparation of the solutions is logical and straightforward, yet experience during lectures and live surgery workshops has shown that participants are very intimidated by the prospect of mixing the solutions and inquire about purchasing ready-made products. However, the best way to ensure accuracy is for the surgeon to prepare the solution. In addition, the formulas can be altered and manipulated for specific uses as needed.
Preparation of the solution requires a comfortable workspace on a surface that is lined for protection or on glass (which is impervious to the acids.) Different sizes of small glass bowls are ideal for mixing. Standard syringes in various volumes (1, 3, 5, and 10 cc), a small glass or metal funnel, surgical gloves, and containers to store the various solutions may also be helpful. Various sizes of opaque glass containers are inexpensive and available from commercial providers, including bottles with phenolic-cone–lined leak-proof caps.
The environment must allow the preparer to devote undivided attention during the mixing process. The ingredients are arranged in glass bowls in the order they will be added; this arrangement should be repeated every time to prevent confusion. Surgical gloves must be worn for protection from the caustic acids. (In my early experience, I always “double-gloved,” but with time I became more cavalier and now have “softened fingerprints”—a sign of a seasoned peeler.)
Once prepared, the acids can be stored in the opaque containers with leak-proof caps for extended periods of time, but variation in concentrations my occur from evaporation if stored more than 6 months.
Historically, formulas were based on drops of croton oil. However, droppers can be awkward to use, especially with small volumes and with the considerable variability in the volume of a drop depending on the specific dropper. Also, it is impossible to split a drop, limiting one′s options. A significant step by Hetter toward simplifying the process was to create a standard phenol-croton oil solution using larger volumes that would then be further diluted with the other ingredients (Table 13-1). This standard solution, or “stock solution,” is made by mixing 24 ml of 88% phenol and 1 ml of croton oil. Standard 89% phenol can be used as well with no practical consequence. By using larger volumes of the ingredients, they are easily measured with accuracy and consistency using standard syringes. Phenol has a tendency to corrode the rubber in the syringes; therefore the syringes may need to be changed if the plunger is no longer moving easily. If the plunger begins to stick, it should not be forced; this may result in splashing. High-quality, old-fashioned glass syringes are ideal if available.
Standard tables are available that further delineate the specific volumes of each ingredient needed to arrive at a specific croton oil concentration. The approximate phenol concentration when using these formulas is 35% unless otherwise noted. The surgeon can simply follow the recipes for a standard concentration or delve further into the mathematics of the formulas to obtain an infinite number of different combinations applicable for specific needs.
In the croton oil concentrations of 0.2%, 0.4%, and 0.8% listed in Table 13-1, the volumes of water and Septisol remain constant at 5.5 ml and 0.5 ml, respectively. The values that change are the relative volumes of phenol and stock solution (which contains phenol and croton oil). The sum of the volumes of the 88% phenol and the stock solution is 4 ml in each of the formulas.
The stock solution consists of 24 ml of phenol and 1 ml of croton oil. Each ml of stock solution has 0.04 ml of croton oil, making this a 4% croton oil solution. For example, looking at the formula for 0.8% croton oil, it is made up of 5.5 ml of water, 0.5 ml of Septisol, 2.0 ml of phenol, and 2.0 ml of stock solution. The 2.0 ml of stock solution contains 0.08 ml of croton oil (2 × 0.04 ml). Because the total volume of the solution is 10 ml, the final concentration of croton oil is 0.08 ml croton oil in 10 ml total volume, or 0.8%. Thus by comparing the volume of stock solution in any of the formulas with the known content of croton oil in the stock solution, the final concentration of croton oil can be easily determined. Notably, the croton oil concentration in the stock solution is extremely high at 4% and should never be directly applied to the skin without further dilution. For instance, the Baker formula had a croton oil concentration of 2.1%.
To make weaker concentrations, the preparer first mixes 0.4% or 0.2% solutions, and these are further diluted by using the formulas indicated in Table 13-1. The final volume of the new solution is 4 ml, and the final phenol concentration is kept at 35%. Ultimately, whatever starting concentration is used with this diluting formula will be diluted by one fourth, because 1 ml of x% croton oil solution + 1.2 ml phenol + 1.8 ml water will yield a ¼x% solution. If larger volumes are desired, all of the values in the formula can be multiplied by the same factor to retain the concentration.
Confirming the phenol concentration in any formula depends on determining the total volume of phenol present. Using the formula for 0.4% croton oil as an example, 3.0 ml of phenol and 1.0 ml of stock solution are used. Because the phenol is not pure but is 88% phenol, the 3.0 ml are multiplied by .88, yielding 2.64 ml. The stock solution is phenol, or 96%. Multiplying the 1.0 ml stock solution by .96 yields 0.96 ml. This 0.96 ml is 88% phenol, and therefore is multiplied by .88 to yield 0.84 ml. Thus the total volume of phenol is 2.64 ml + 0.84 ml, or 3.48 ml. In a total volume of 10 ml, the phenol concentration is 34.8%. Each of the formulas vary slightly, but for convenience, they are considered 35%.
A useful variation is to add olive oil at a final concentration of 10% by volume. The addition of olive oil has a tempering effect on the absorption and allows more even distribution of the solution. In 10 ml formulas, this concentration is achieved by changing the water volume to 4.5 ml and adding 1.0 ml of olive oil. In the weaker croton oil solutions, such as 0.1%, in which the total volume is 4 ml, the water volume added is 1.4 ml, and the olive oil volume is 0.4 ml.
The use of 35% phenol concentration stems from Hetter′s observation that a high concentration of phenol was not necessary to result in a good peel.2 It is possible to alter the formulas to obtain a lower concentration, potentially for a lighter peel (although the croton oil concentration is the primary determinant). Another option is to prepare a solution with a higher concentration of phenol, such as 60%, with a weak concentration of croton oil, such as 0.1%, 0.05%, or even weaker to use in instances where pigmentation is more of an issue than wrinkles. To change the phenol concentration to 60% in the 0.1% croton oil 4 ml formula, the total volume of phenol needed (x) is determined by x/4 ml =.60; thus x = 2.4 ml. Because 0.35 ml of phenol comes from the 1 ml of 0.4% croton oil solution (which is a 35% phenol solution), this leaves 2.05 ml of phenol lacking. The equation .88x = 2.05 represents the volume (x) of 88% phenol needed for this amount, in this case 2.33 ml. In the formula, the volume of phenol and the volume of water add up to 3 ml; substituting 2.33 ml of phenol and 0.67 ml of water in the formula results in a 60% phenol solution. This formula concept can be used to customize solutions for specific individuals and clinical situations.
Intraoperative Routine
Traditionally, the Baker peel and the more recent iteration have been done under general anesthesia or intravenous sedation because of the considerable pain of the chemical burn. Regardless of which approach is chosen, adequate blocking of pain is important to prevent excessive stimulation and to allow a pain-free emergence from anesthesia. If the patient wakes up comfortable, the entire recovery and general experience is better. Some patients report mild tingling or burning the first night but are usually comfortable by morning.
After induction of anesthesia, complete local sensory nerve blocks are performed with bupivacaine with epinephrine. These include the supraorbital, supratrochlear, infratrochlear, zygomatico-temporal, zygomatico-facial, infraorbital, dorsonasal, mental, and cervical branches. An excellent discussion of this topic can be found in the journal Cosmetic Dermatology authored by Joseph Niamtu III.3–6 Subcutaneous infiltration of dilute plain bupivacaine throughout the entire operative site is very useful. Color changes of the skin are important indicators of depth reached; therefore epinephrine is not used in this superficial infiltration to prevent blanching. Intramuscular ketorolac tromethamine, 30 to 60 mg, is administered as an adjunct to anesthesia.
These anesthetic techniques are the common; I have used them successfully for more than a decade. An innovative alternative approach that allows the surgeon to comfortably perform even deep peels with oral sedation and no local anesthesia is described in detail later in the chapter.
Ophthalmic ointment and corneal protectors are not used, because the phenol may dissolve in the ointment and prevent complete flushing out if necessary. Extreme caution around the eyes is imperative.
The fear of cardiac toxicity has been historically associated with phenol peels, but rare reports of death are anecdotal and it is impossible to implicate phenol toxicity rather than anesthesia complications. Traditional peels were performed with general anesthesia or sedation but without local blocks. There is speculation that the catecholamine release caused by the intense stimulation of the high concentration of croton oil may have been the cause of the arrhythmias. With a lower concentration of phenol (35% versus 49%), lower concentrations of croton oil, and thorough local anesthesia of the face (or the newer technique discussed later), cardiac complications have not been seen. Thomas Baker,1 who popularized the traditional peel, has stated that in his many years of experience, he never encountered cardiac arrhythmias that required treatment. Recent studies show that when peeling is performed under anesthesia but without blocks, arrhythmias are not uncommon, but they are benign in nature. General recommendations include cardiac monitoring, adequate hydration, and peeling a full face in no less than 45 minutes. Following these guidelines, I have not seen any cardiac complications in nearly 17 years of peeling.
The patient is instructed not to apply anything on the skin on the morning of the procedure; before peeling the skin is thoroughly degreased with acetone. If operating room regulations forbid the use of acetone, it can be applied in the preoperative area and the skin again degreased with alcohol in the operating room. The process of peeling should be orderly and systematic. Of primary importance is safety, particularly in protecting the eyes, preventing inadvertent peeling where not desired, and preventing splashing of the acids. As previously explained, corneal protectors and ophthalmic ointment are not used, so great care must be exercised. Specific measures include gentle elevation of the head to prevent acid rolling into the eyes, never using an applying sponge so wet that it can drip, and never crossing over the eyes with an applying sponge in hand. The operating surgeon′s hands must be free of acid to prevent application where not desired. The hands can be wiped dry by an assistant or a surgical towel or other cloth can be clipped to the surgeon′s scrub shirt shoulder and then draped over the front for wiping the hands. The acids need to be placed in clearly labeled glass bowls and arranged in a consistent manner to prevent confusion. The surgeon′s demeanor is particularly important: It should never be hurried or brusque, always focused, deliberate, and free of distractions.
The applying materials include 2-inch by 2-inch gauze (preferably synthetic fiber, which is less abrasive), large cotton-tipped applicators, and small cotton-tipped applicators (both the sponged and wooden ends). Toothpicks and aesthetician sticks (such as those used for applying wax) are also useful. The gauze is folded twice to decrease the surface area of contact and ensure greater accuracy. It is then dipped in the solution and carefully wrung out. The solution is stirred before each application to ensure even mixing of the oil and aqueous components. The gauze should be moist, but not so saturated that it could drip. The gauze should be set in a safe place and the hands dried to prevent the application of acid where it is not wanted. This is particularly important in segmental peels, in which errors are obvious. Again, the surgeon should never cross over the eyes with the wet gauze (or applicator) in hand.
Once the gauze is passed over the skin, the action of the acid is evident in 10 to 15 seconds, depending on the wetness of the gauze and the concentration of the croton oil solution. When it comes in contact with the skin, the acid coagulates and precipitates the protein, forming a frost (varying degrees of a white appearance to the treated area). As the application progresses, multiple passes are made, and the depth of the skin reached is gauged by the degree and quality of the white appearance. The frosting appearance becomes progressively more dense, solid, and opaque. Histologically, this corresponds with the coagulating action of the acid first passing through the epidermis to the papillary dermis (the juncture between the epidermis and the dermis). As the peel passes from the papillary dermis into the upper and midreticular dermis, the frosting becomes a dull, flat white without any appearance of shine or depth. Unlike TCA peels, there is no need to wait several minutes to see the final effect of the application. Once the acid solution is applied, there is no “going back”; no neutralizing agent is available, and the effect is irreversible. The only recourse is that if the application is too wet (and has the potential to go deeper than intended), quickly blotting it will diminish the depth. As explained later in this chapter, this technique can be very useful on deep wrinkles.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


