Chapter 12 Filler Injection of the Nasolabial Fold
10.1055/b-0040-178130
Chapter 12 Filler Injection of the Nasolabial Fold
Introduction
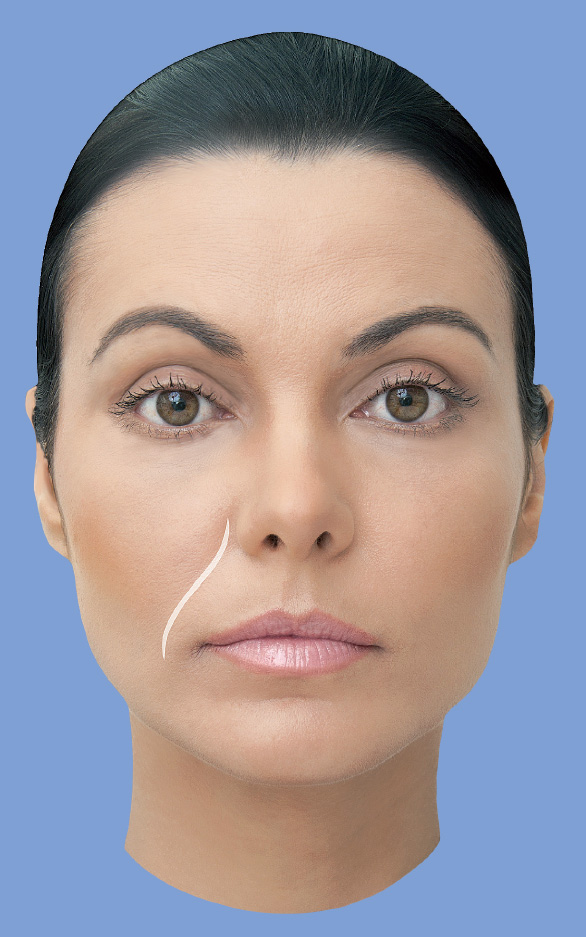
The nasolabial fold originates laterally to the ala of the nose and ends 1 to 2 cm laterally to the oral commissure. With aging, the progressive ptosis of the malar fat and overlying skin contributes to deepening of the fold, but the depth also varies according to race, gender, age, and weight. The superior region of the fold (perinasal triangle) acquires the shape of an inverted triangle, and is the deepest part of the fold as a result of bone remodeling of the piriform aperture and the maxilla (Fig. 12.7).1
Anatomy
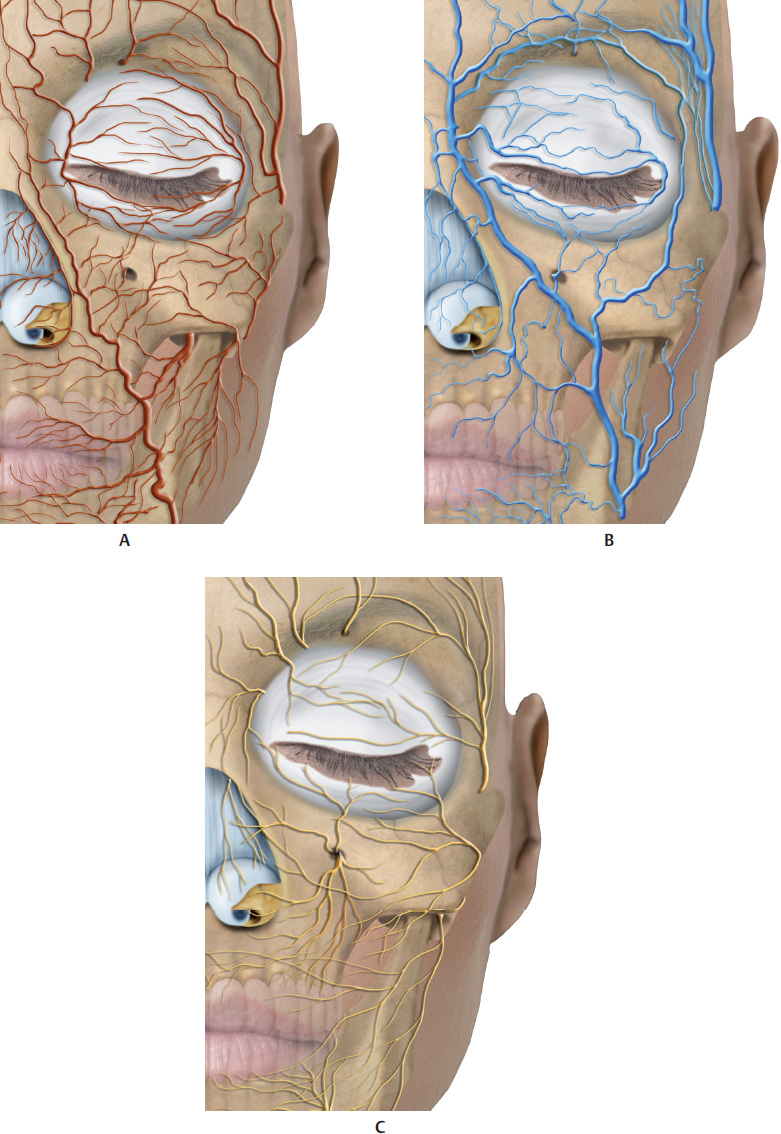
The nasolabial fold is supplied by the facial artery, a branch of the external carotid artery. After dividing into the inferior and superior labial branches, the facial artery follows its course in the region of the nasolabial fold and divides into a septal branch, which irrigates the nasal septum, and an alar branch, which in turn supplies the ala of the nose. After dividing into these two branches, the facial artery continues its ascending course and divides into the lateral nasal branch. This supplies the ala of the nose and nasal dorsum, and anastomoses with the contralateral side, with the septal and alar branches, the dorsal nasal branch of the ophthalmic artery, and the infraorbital branch of the maxillary artery. Because of this anatomy, intravascular injection or external vascular compression is among the possible complications of this filler injection, which manifest clinically as necrosis of the ala and the tip of the nose.
In a study by Yang et al, the facial artery was observed in the region of the nasolabial fold in 93.3% of cases. In 42.9% of cases, it was located medially to the fold, and in 23.2%, laterally. In the remaining cases, the facial artery crossed the nasolabial fold medially or laterally (Fig. 12.1–12.6 and12.8–12.11).2
Technique
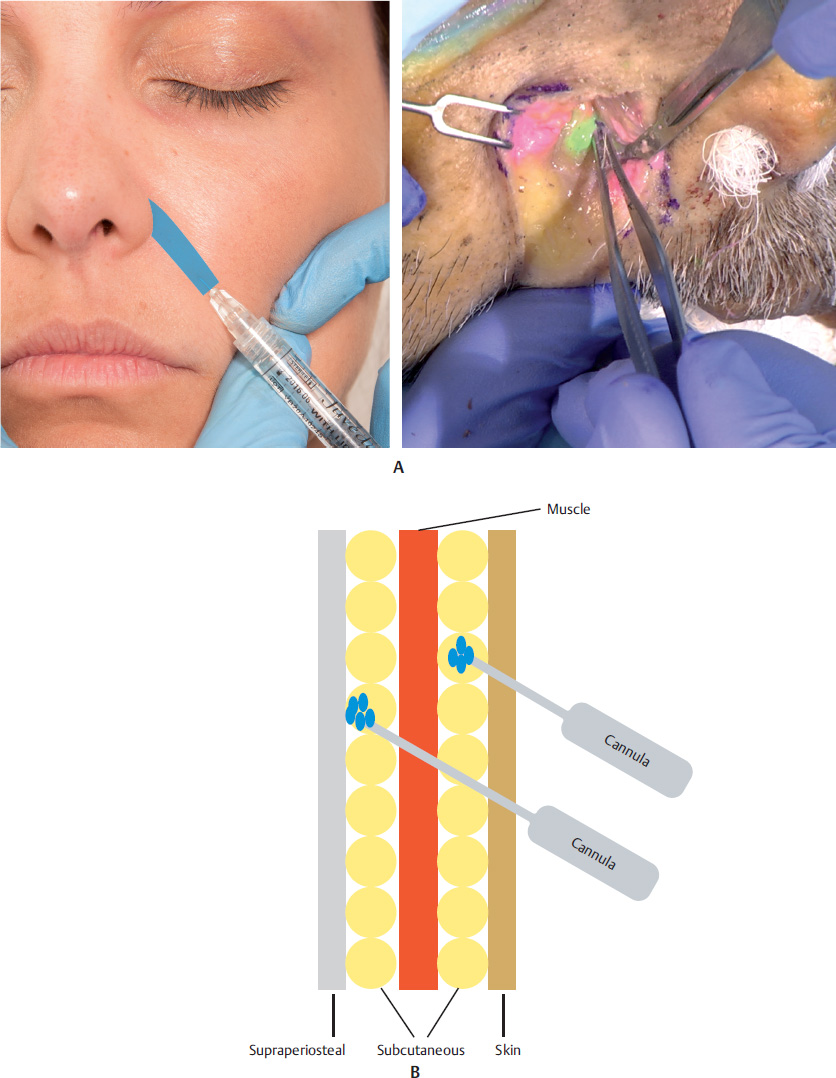
The perinasal triangle can be filled with hyaluronic acid (HA) via the middermis or deep dermis, using a linear retrograde injection fanning technique. In cases of more severe loss of volume, the subcutaneous and/or supraperiosteal space should be filled with a volumizer or filler for the deep dermis, using a microcannula or needle. In that case, insert the needle into the deep plane at a 90° angle, aspire, and administer a local bolus.
The rest of the fold can be filled with a linear retrograde or antegrade injection into the deep dermis.
The adverse effects associated with the procedure, such as hematoma, erythema, edema, and localized sensitivity, resolve spontaneously within 7 to 10 days. Cording is usually caused by an inadequate technique, a very superficial injection, or the use of material that is too thick for the site. It can be eliminated with local massage and/or hyaluronidase. The most severe complication is tissue necrosis resulting from interruption of blood supply, either because of direct vascular obstruction or external compression. A few hours after the procedure, the area that has suffered ischemia takes on a reticulated, purplish, erythematous appearance and, if not treated in time, can progress to necrosis and tissue loss.3
References
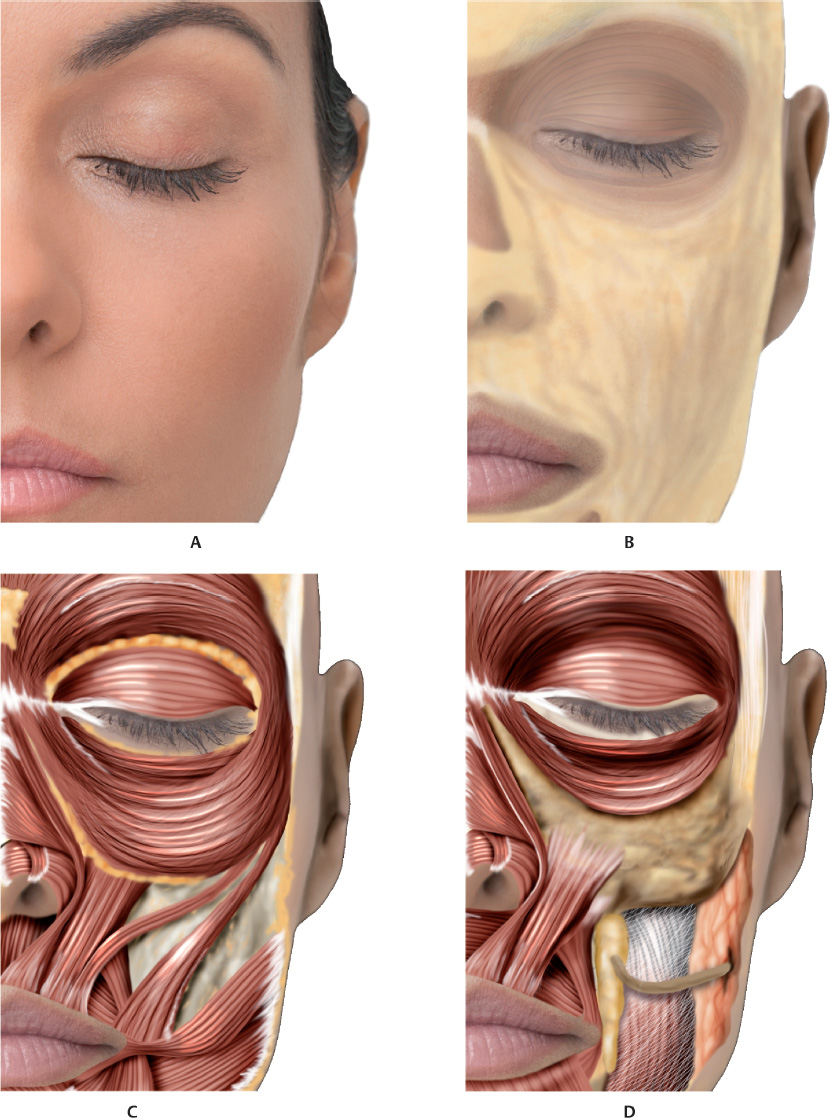
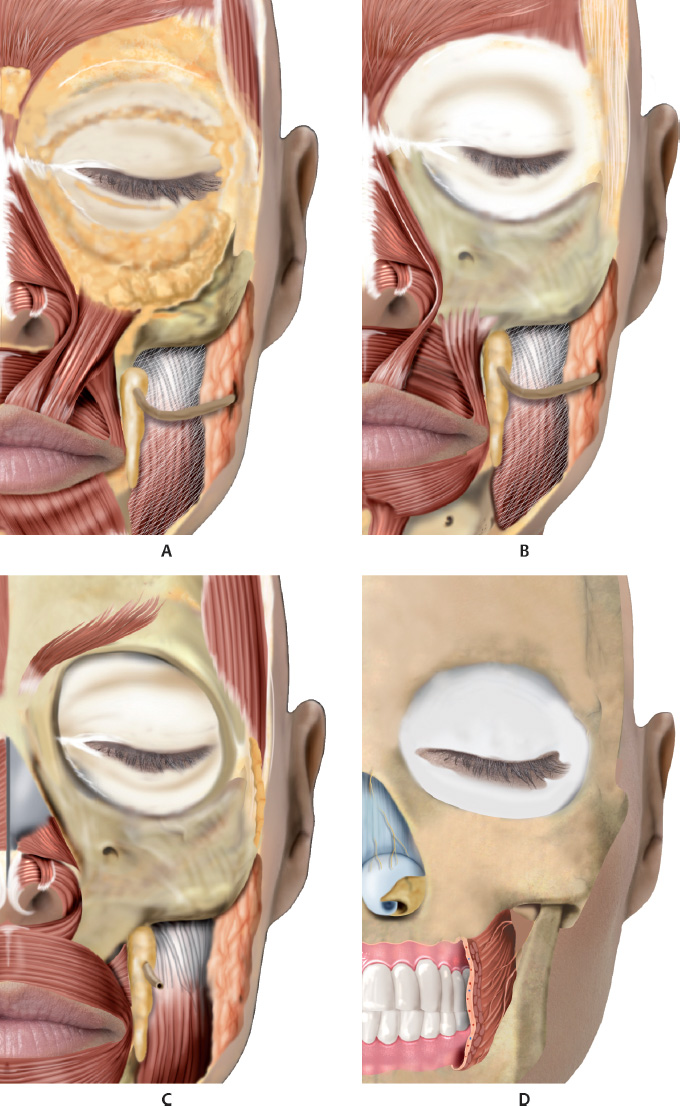
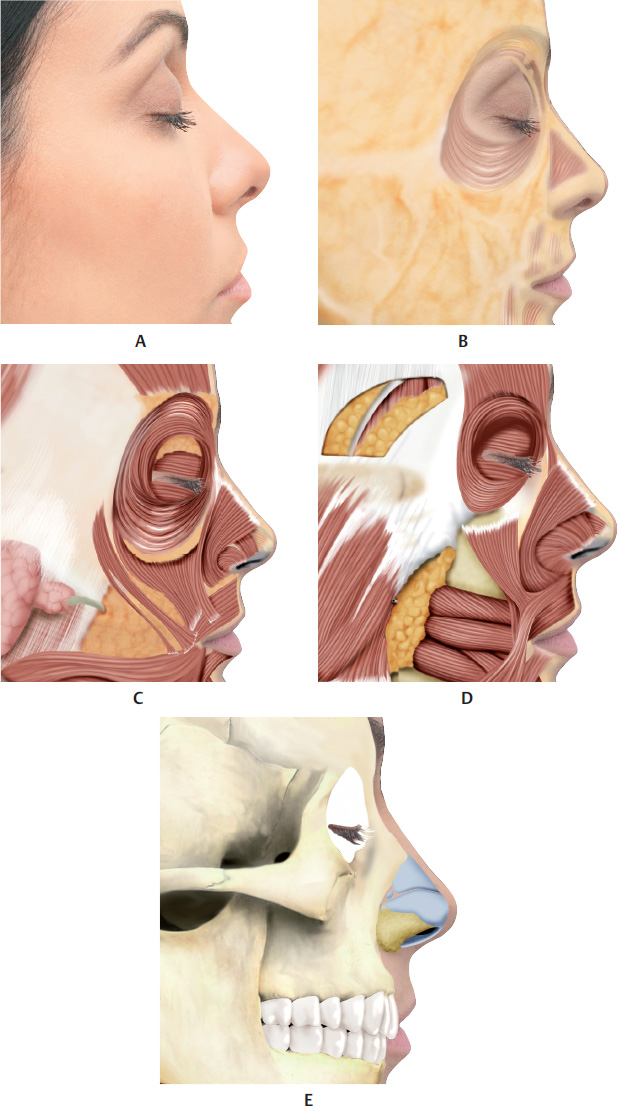
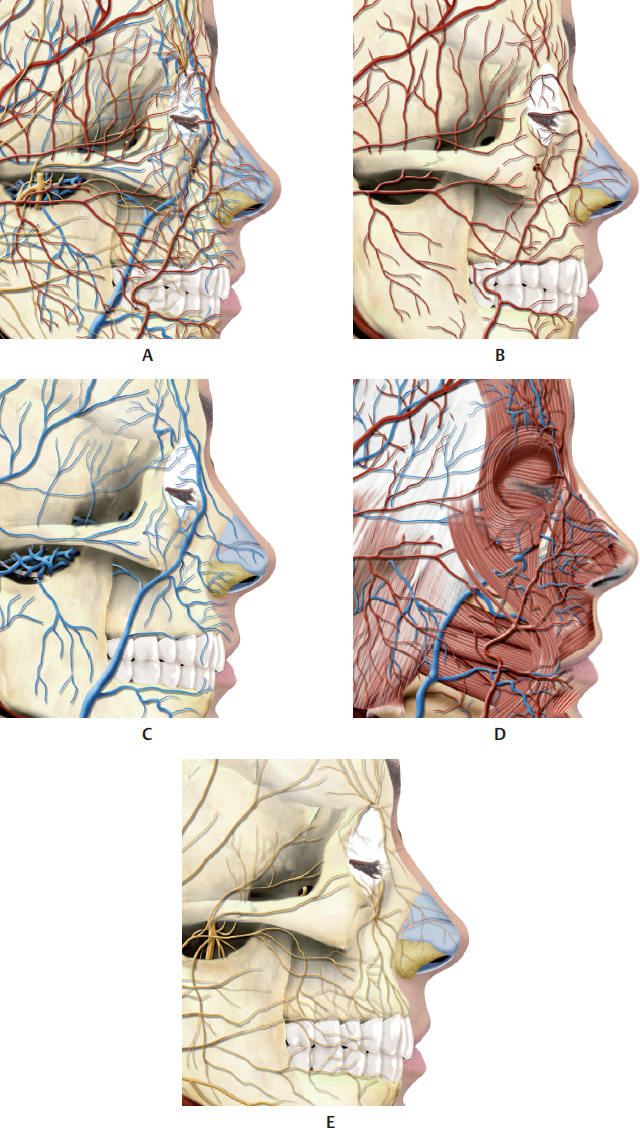
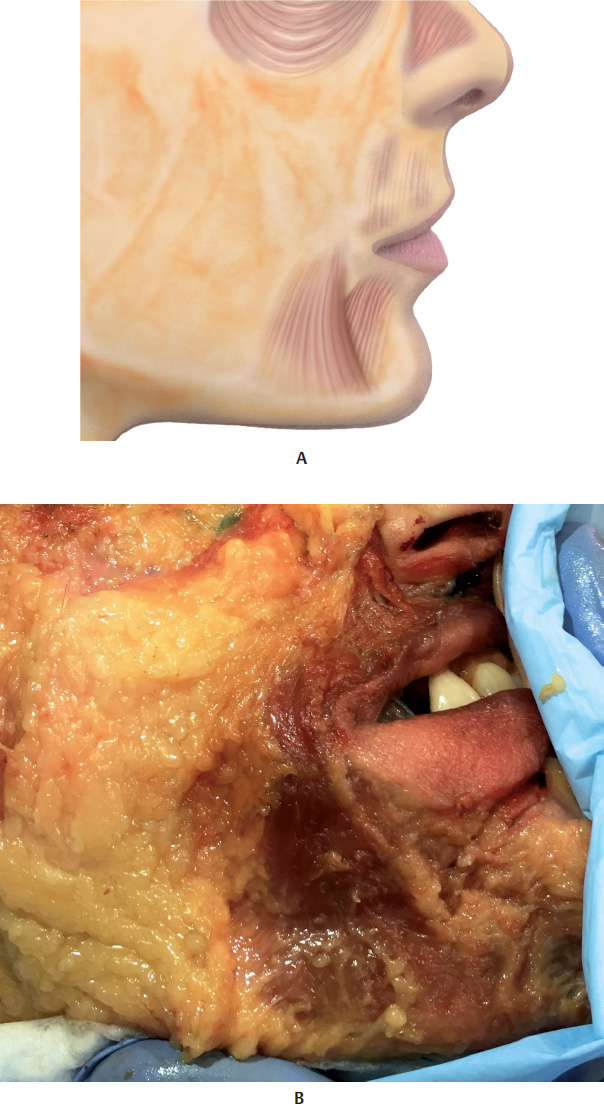
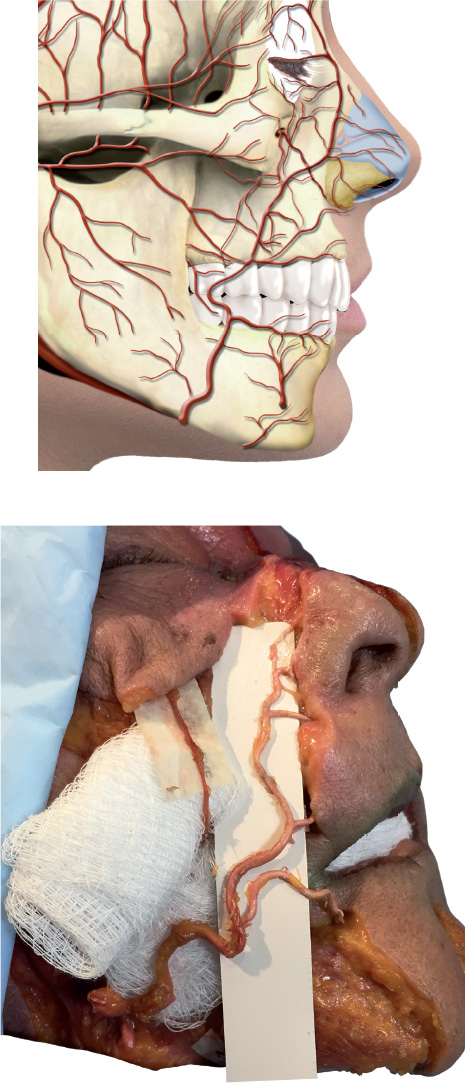
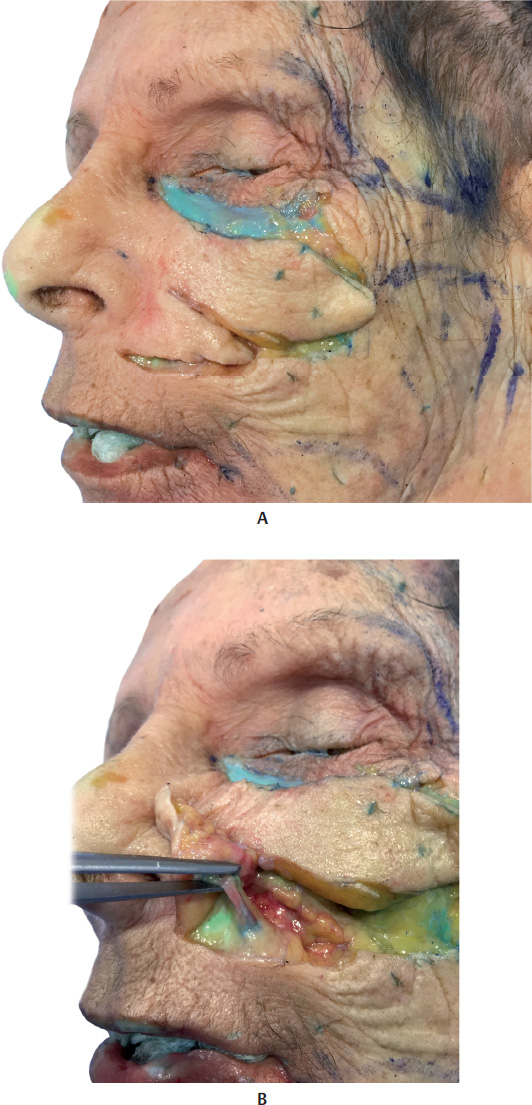
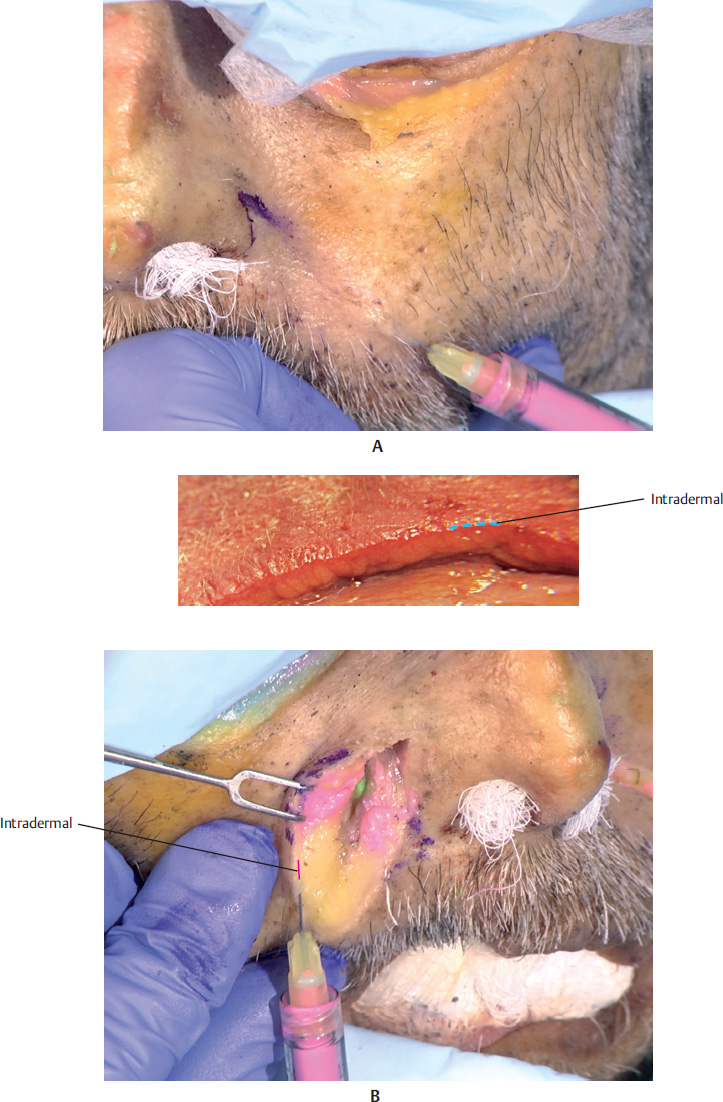
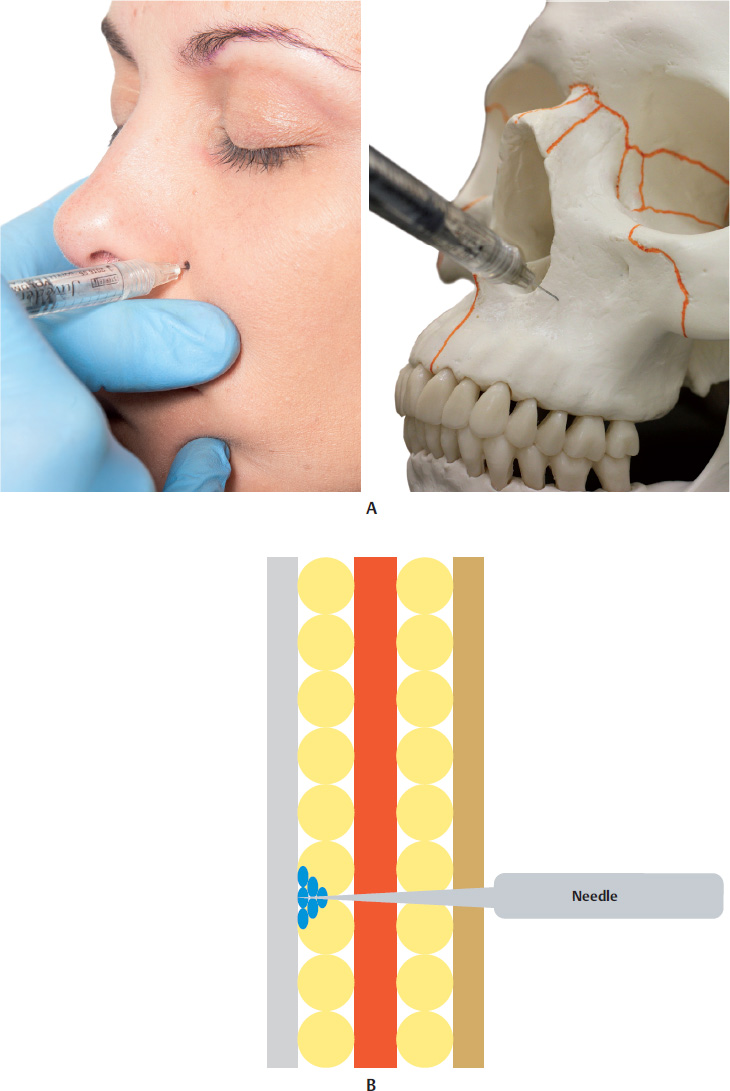
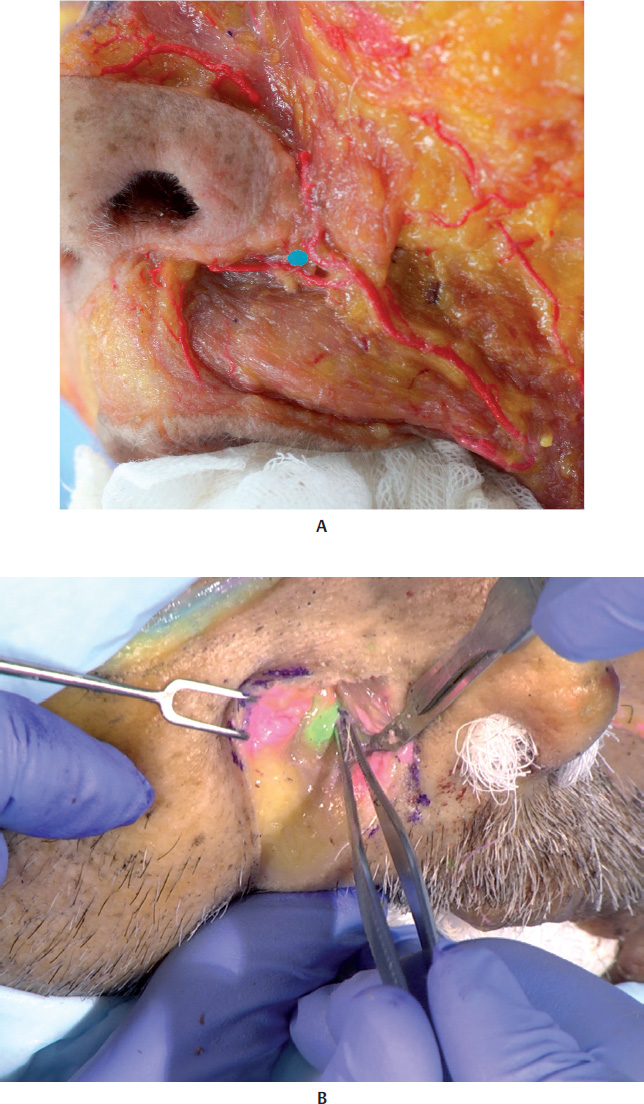
1 Shaw RB Jr, Katzel EB, Koltz PF, et al. Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg 2011;127(1):374–3832 Yang HM, Lee JG, Hu KS, et al. New anatomical insights on the course and branching patterns of the facial artery: clinical implications of injectable treatments to the nasolabial fold and nasojugal groove. Plast Reconstr Surg 2014;133(5):1077–10823 Grunebaum LD, Bogdan Allemann I, Dayan S, Mandy S, Baumann L. The risk of alar necrosis associated with dermal filler injection. Dermatol Surg 2009; 35(2, Suppl 2):1635–1640Fig. 12.1 A. Anterior view of the anatomy of the region of the nasolabial fold.B. Same. region after removal of the skin.C. Same. region after removal of the skin and the superficial fat pads (SFPs).D. Same region after removal of the skin, SFPs, orbital portion of the orbicularis oculi muscle (OM), zygomatic muscles, risorius muscle, and buccinator muscle.Fig. 12.2 A. Anterior view of the anatomy of the region of the nasolabial fold after removal of the skin, superficial fat pads (SFPs), palpebral and orbital portions of the orbicularis oculi muscle (OM), and zygomatic muscles.B. Same. region after removal of the skin, the SFPs, the palpebral and orbital portions of the OM, the medial and lateral suborbicularis oculi fat (SOOF), the levator muscle of the upper lip, and the zygomatic major and minor muscles.C. Same. region after removal of the levator muscle of the upper lip, the ala of the nose, and the levator muscle of the angle of the mouth.D. Bone. structure of the region of the nasolabial fold.Fig. 12.3 A. Anterior view of the left side of the face of the 3D digital model.B. Left side of the face showing veins, arteries, and nerves in the area of the nasolabial fold.Fig. 1.2 Anterior view of the face focusing on the nasolabial fold.A. Corresponding arterial vascularization.B. Corresponding venous vascularization.C. Corresponding. innervation.Fig. 12.5 A. Lateral view of the right side of the face.B. Same region after removal of the skin, showing the superficial fat pads (SFPs).C. Same region after removal of the skin and the SFPs. The palpebral and orbital portions of the orbicularis oculi muscle (OM) are visible, with the latter portion over the medial and lateral suborbicularis oculi fat (SOOF) pads. The levator muscle of the upper lip and ala of the nose can be seen, as well as the levator muscle of the angle of the mouth and the zygomatic major and minor muscles above the deep fat pads (DFPs).D. Same region after removal of the orbital portion of the OM, medial and lateral SOOF, SFPs, and DFPs. A part of the buccal fat pad (Bichat’s fat pad) can be seen above the buccinator muscle.E. Bone structure of the region of the nasolabial fold.Fig. 1.2 Profile view of the right side of the face focusing on the nasolabial fold.A. Corresponding vascularization and innervation.B. Corresponding arterial vascularization.C. Corresponding venous vascularization.D. Arterial and venous vascularization integrated in the frontal muscle, orbicularis oculi muscle (OM), nasal muscles, zygomatic major muscle, levator muscle of the lip, buccinator, and masseter muscle.E. Corresponding innervation.Fig. 12.7 A. andB. Anterior view of the delimitation of the nasolabial fold.C. andD. Close-ups ofA. andB..Fig. 12.8 A. Superficial fat pads (SFPs) of the face (see nasolabial region).B. Right side of the face of a fresh cadaver specimen with skin folded back to show the SFPs and the depressor muscle of the angle of the mouth.Fig. 12.9 Illustration and fresh cadaver specimen showing the angular artery, which is formed by the division of the facial artery into the inferior and superior labial branches. The angular artery supplies the region of the nasolabial fold and also divides into branches that supply the ala of the nose and nasal dorsum.Fig. 12.10 A. Left side of the face of a fresh cadaver specimen.B. Angular artery has been pinched after removal of the skin and the nasolabial fat pad.Fig. 12.11 A fresh cadaver specimen showing the angular artery.Fig. 12.12 A. Demonstration of a filler injection technique in the nasolabial fold using a needle in the intradermal plane.B. Application plan for the product in the intradermal plane. Insert the needle at a 30° angle. Both linear retrograde or antegrade injections are possible.Fig. 12.13 A. Left side of the face of a fresh cadaver specimen showing application of the product in the intradermal plane. The shadow of the needle can be seen through the skin.B. Right side of the face of a fresh cadaver specimen with the nasolabial fold cut and folded back to show the location of the needle in the intradermal plane, above the subcutaneous tissue.Fig. 12.14 A. Demonstration of a filler injection technique in the nasolabial fold (region of the perinasal triangle) with a needle in the supraperiosteal plane.B. Application plan for the product in the supraperiosteal plane. Insert the needle perpendicularly, applying the bolus, then aspire.Fig. 12.15 A. Left side of the face of a fresh cadaver specimen with skin and part of the subcutaneous tissue removed. See the application point (blue circle). The product was applied with a needle to the supraperiosteal plane.B. The product is visiblein green.Fig. 12.16 A. Demonstration of a filler injection technique in the nasolabial fold using a cannula in the subcutaneous plane. The product is visiblein pink.B. Application plan for the product in the subcutaneous plane. A linear retrograde or antegrade injection can be applied, as well as a bolus, in the area of the piriform aperture.Fig. 12.17 A. A patient with loss of volume in the middle third of the face.B. Filler injection in the right malar and zygomatic regions with a 25 G microcannula.C. Filler. injection in the right nasojugal groove (NJG) with a 27 G microcannula.Fig. 12.18 Right side of the face of the patient fromFig. 12.17before and after a filler injection in the malar region and nasojugal groove (NJG). Note the improvement in the nasolabial fold after the procedure.Fig. 12.19 A. Patient with loss of volume in the middle third of the face.B. Filler injection of the left malar, zygomatic, and nasojugal groove (NJG) regions.C. As. after treatment of the abovementioned areas the problems in the left nasolabial fold (N LF) persisted, we performed a filler injection with needle in the intradermal plane.Fig. 12.20 Left side of the face of the patient fromFig. 12.19before and after a filler injection in the malar, zygomatic, nasojugal groove (NJG), and nasolabial fold regions.Fig. 12.21 Frontal and left profile views of the same patient before and after a filler injection in the malar, zygomatic, nasojugal groove (NJG), and nasolabial fold regions.
Only gold members can continue reading. Log In or Register to continue