Chapter 10 Filler Injection of the Malar and Zygomatic Regions
10.1055/b-0040-178128
Chapter 10 Filler Injection of the Malar and Zygomatic Regions
Introduction
A young and attractive face is characterized by a well-contoured and convex malar region. This area of the face is best visualized at a 75° angle and has been used since ancient times by artists to emphasize facial beauty and, more recently, by photographers and in the preparation of 3D digital models. At this angle, the facial contour presents the shape of the Greek letter ζ (sigma), also called the “cyma line.”
Nonetheless, bone remodeling caused by the aging process associated with atrophy and a downward shift of the local fat pads result in volume loss in this area, which gradually flattens and, in extreme cases, becomes concave. Weight loss and congenital predisposition can also cause this loss of volume.14
Volumization of the malar region requires the injector to have an in-depth knowledge of anatomy, a keen sense of esthetics, and technical skill (Fig. 10.7 and10.27). Overcorrection of the zygomatic region can broaden the horizontal diameter of the face, conferring a more masculine look to women. When treating the infraorbital region, it is essential to choose the correct application plane, as a very deep injection may not give the desired result, while a very superficial one, or an injection into the nasojugal groove, could cause persistent edema or visibility of the product.
Anatomy
Fat Pads
The adipose tissue in the middle third of the face consists of a superficial portion and a deep one. The superficial portion comprises the nasolabial, medial cheek, middle cheek, and temporolateral fat pads. The deep portion comprises the medial and lateral portions of the suborbicularis oculi fat (SOOF), also called prezygomatic fat, and the deep medial and deep lateral cheek fat pads.5,.6
When the superficial and deep portions are separated, it is possible to see the orbital portion of the orbicularis oculi muscle (OM) and the superficial muscular aponeurotic system (SMAS) encompassing levator muscle of the upper lip and the ala of the nose, the levator muscle of the upper lip, the zygomatic major and minor muscles, and the vessels and nerves.
The superficial nasolabial and medial malar fat pads cover the orbital portion of the OM, which originates below the palpebral portion, 0.5 to 1 cm below the inferior orbital rim. The SOOF is below the orbital portion of the OM, resting over the maxilla and the zygomatic bone.
The superficial medial cheek fat pad, superficial middle cheek fat pad, and SOOF are relevant for augmenting the malar region (Fig. 10.1,10.2,10.5, and10.8–10.15).
Vascularization
The superficial medial cheek fat pad and the medial SOOF are supplied by branches of the facialaand infraorbital arteries.
The facial vein crosses the middle third of the face more laterally than the artery, and after crossing below the zygomatic major muscle, it becomes more superficial bordering the SOOF medially. In its superior portion, it is located deep to the superficial medial cheek fat pad and superficially to the SOOF, then below the OM.
More laterally, the middle cheek fat pad and the lateral SOOF are supplied by the perforating branches of the transverse facial arteryband the zygomatico-orbital artery. In this region, the perforating arteries are sparse and large, contrary to what occurs in the medial region, where they are thin and numerous (Fig. 10.3–10.6).7–9
Innervation
Sensory
Sensory innervation is supplied by the maxillary branch of the trigeminal nerve.
Motor
Motor innervation is supplied by the temporal and zygomatic branches of the facial nerve (Fig. 10.4–10.6).
Malar Fold
The malar fold translates clinically as an extension of the nasojugal groove in the malar region. According to Furnas,10it is an imaginary oblique line that extends from the zygomatic ligamentcto the medial commissure of the eye. Its origin is still somewhat unclear, but it is thought to contribute to the formation of the malar fold.
Skin ligaments: Fibrous strand that covers the medial bundle of the OM whose fibers insert into the skin.
Malar septum: The malar septum seems to be primarily a structure of the OM. It originates in the periosteum of the inferior orbital rim (marginal arch) and takes a caudal direction, going around the medial portion of the OM, to then fuse with the fibrous septum of the superficial fat pad (SFP), inserting into the skin 2.5 to 3 cm from the lateral commissure. The malar fold divides the malar region into two: The external part, over the cheekbone and SOOF, and the internal and inferior part, which rests over the region of the levator muscle of the upper lip.1115
Technique
The objective is to restore the volume lost during the aging process or during weight loss, providing the patient with infraorbital projection and, if necessary, projection of the cheekbone area. Augmentation of the latter is necessary in specific cases where the additional volume does not confer a masculine look when the diameter of the face is increased. For a natural and balanced effect, it is necessary to concentrate on the area of volume loss, without changing the form of the patient’s face.
A filler injection using a cannula is preferable, due to the lower risk of intravascular injection and formation of hematomas. When treating the deeper planes, such as the medial SOOF, it is important to remember that the facial vein flows above the SOOF and below the orbital part of the orbicular muscle. There are fewer incidences of edema, and greater patient comfort is achieved, when using a cannula because it makes it possible to fill the entire infraorbital and zygomatic area using only one entry point.
While using a needle for the filler injection, avoid the infraorbital foramen. Aspire and inject slowly.
Some practitioners suggest filling the medial cheek fat pad below the SMAS, which requires larger volumes of hyaluronic acid (HA). We do not use this approach not only because of the abovementioned reasons, but also because it is riskier given the presence of the vessels and nerves in the SMAS.6
The techniques used are described below:
Superficial Cannula Technique for the Malar Region
Mild to moderate edema may occur immediately after the procedure that is associated with the volume injected, the patient’s individual susceptibility, the injection planes, and the type of product. Pain or discomfort at the site of injection are common and resolve spontaneously within 2 to 3 days. Hematomas can be minimized by using a cannula, but they can still occur at the entry point of the cannula, albeit to a lesser extent.
A rare complication is the occurrence of delayed-onset edema, months after the procedure.
Conclusion
Familiarity with the fat pads of the middle third of the face, as well as with the local musculature, vascularization, and innervation is fundamental for achieving adequate and safe volumization of the malar and zygomatic regions. An injection into the correct fat pad and plane yields excellent results, leading to both patient and physician satisfaction (Fig. 10.35–10.37).
References
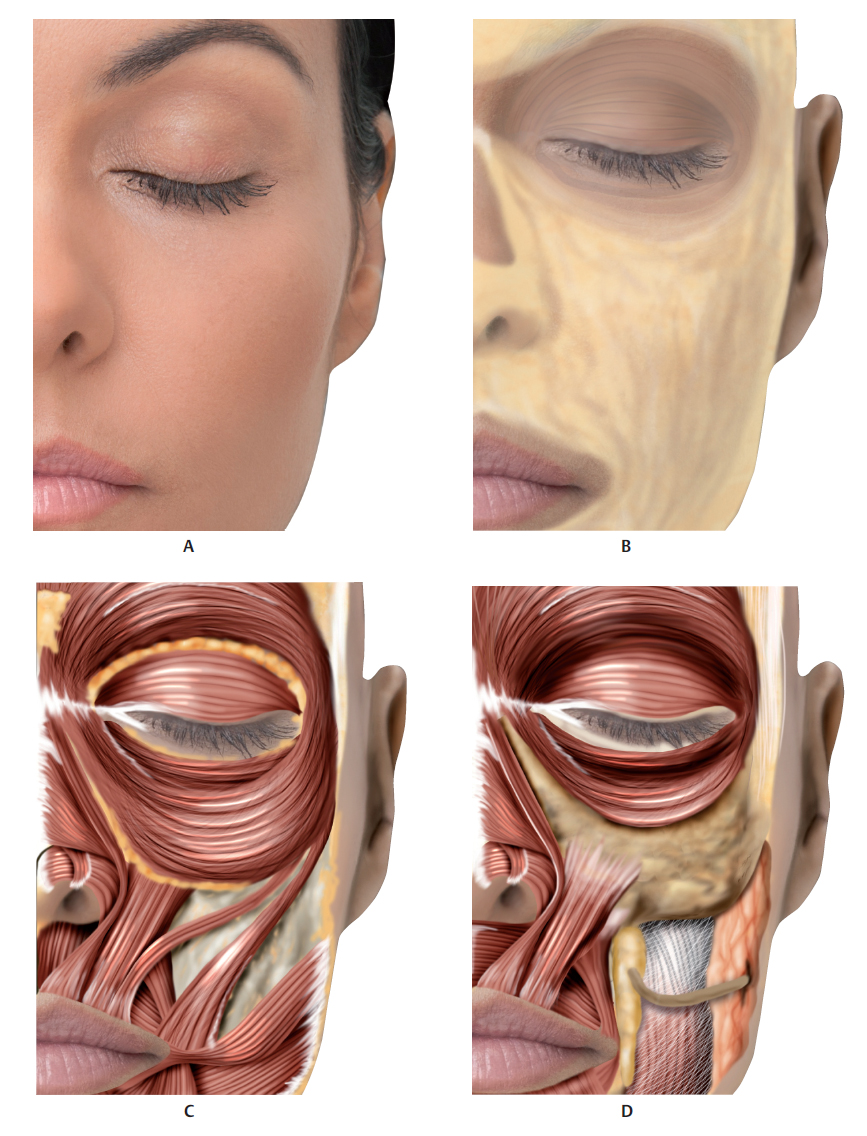
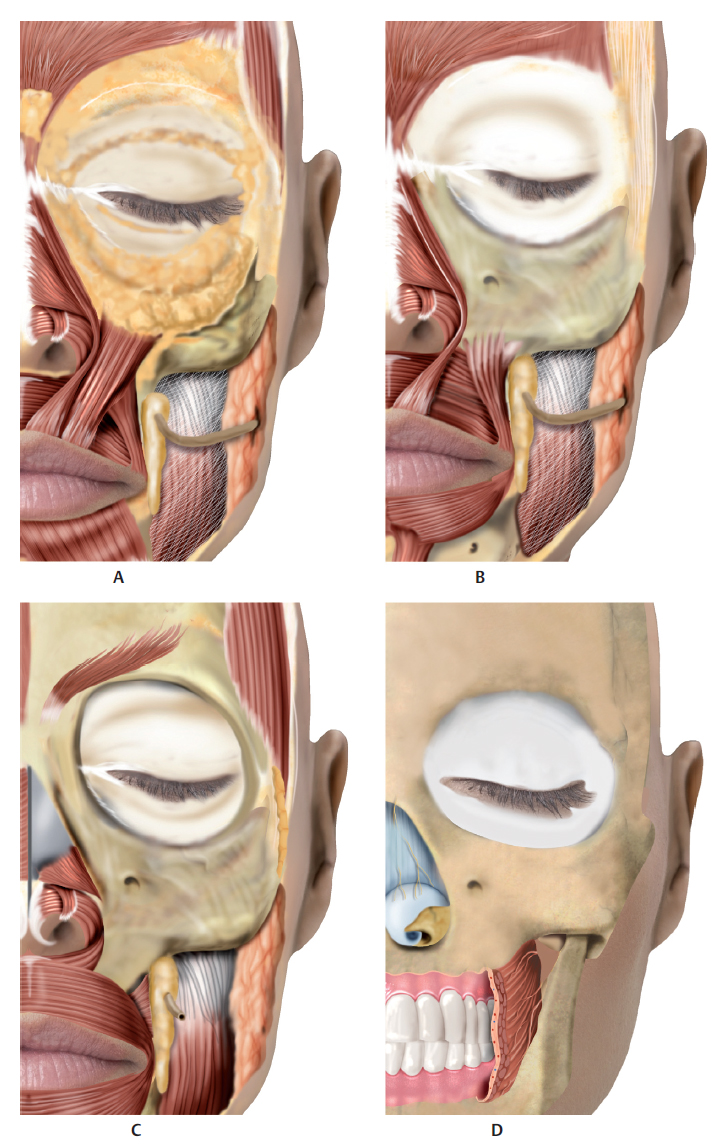
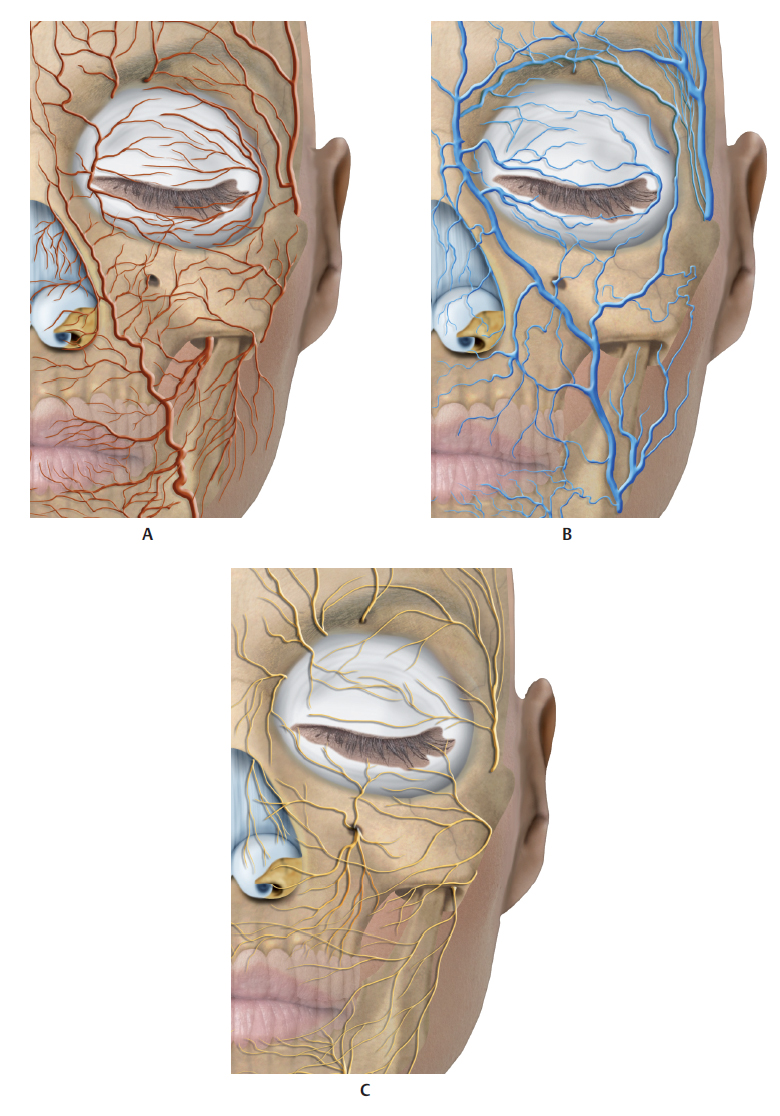
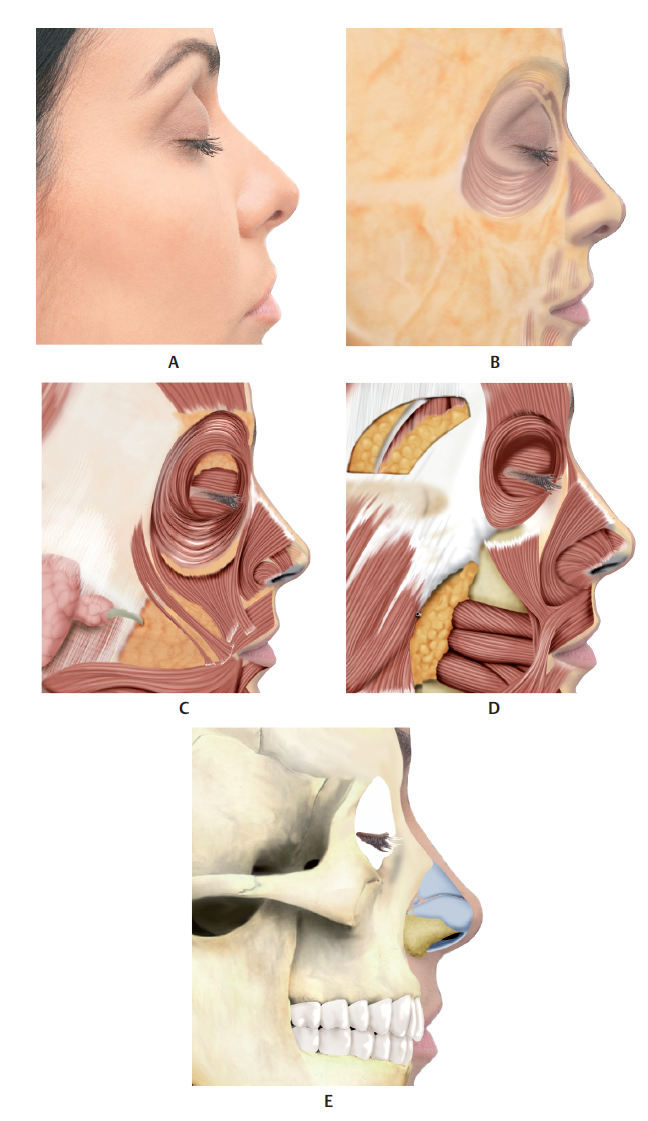
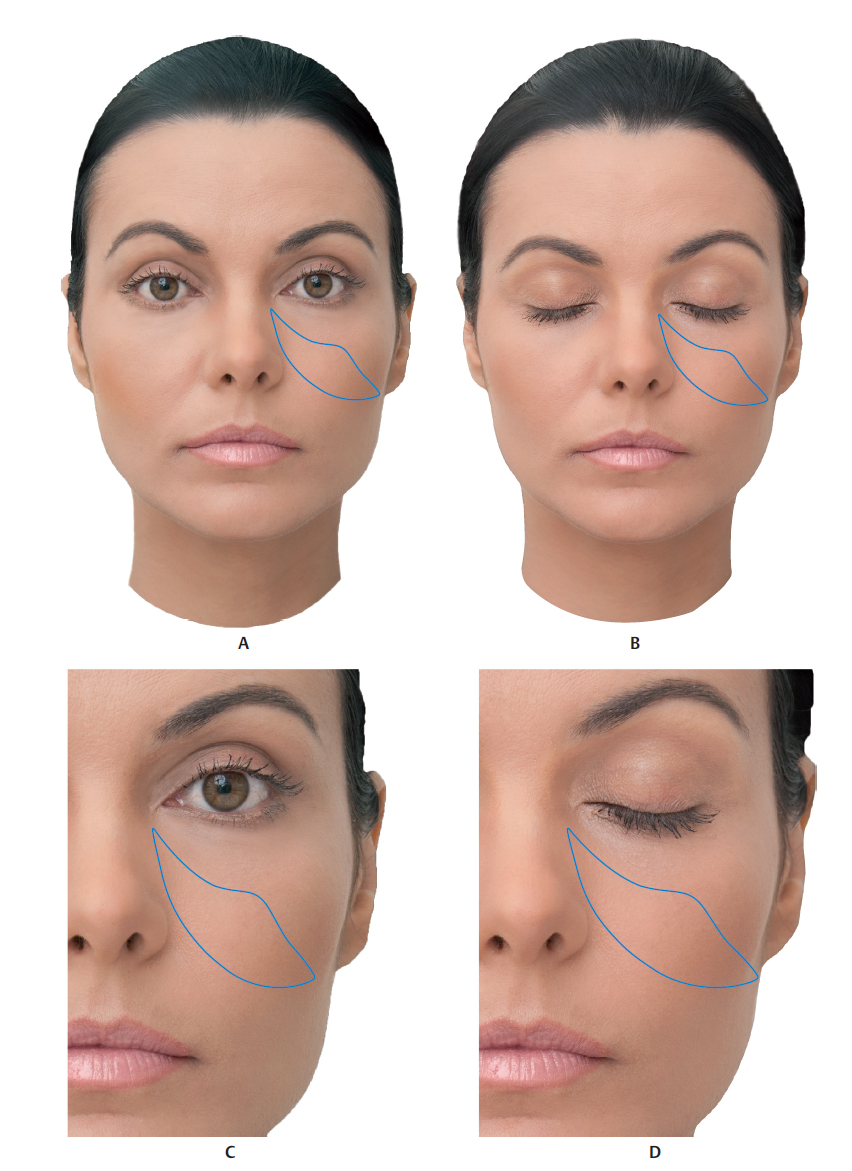
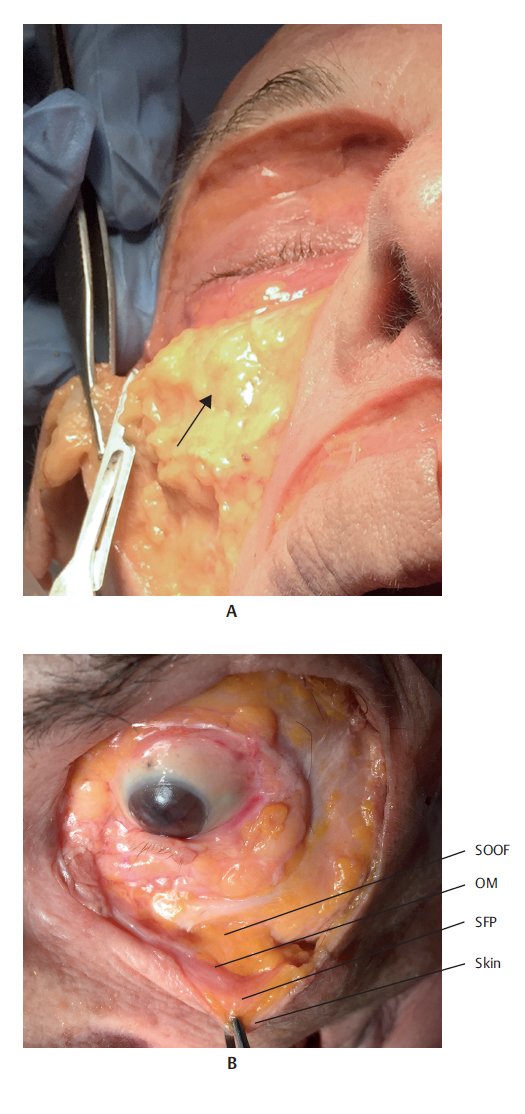
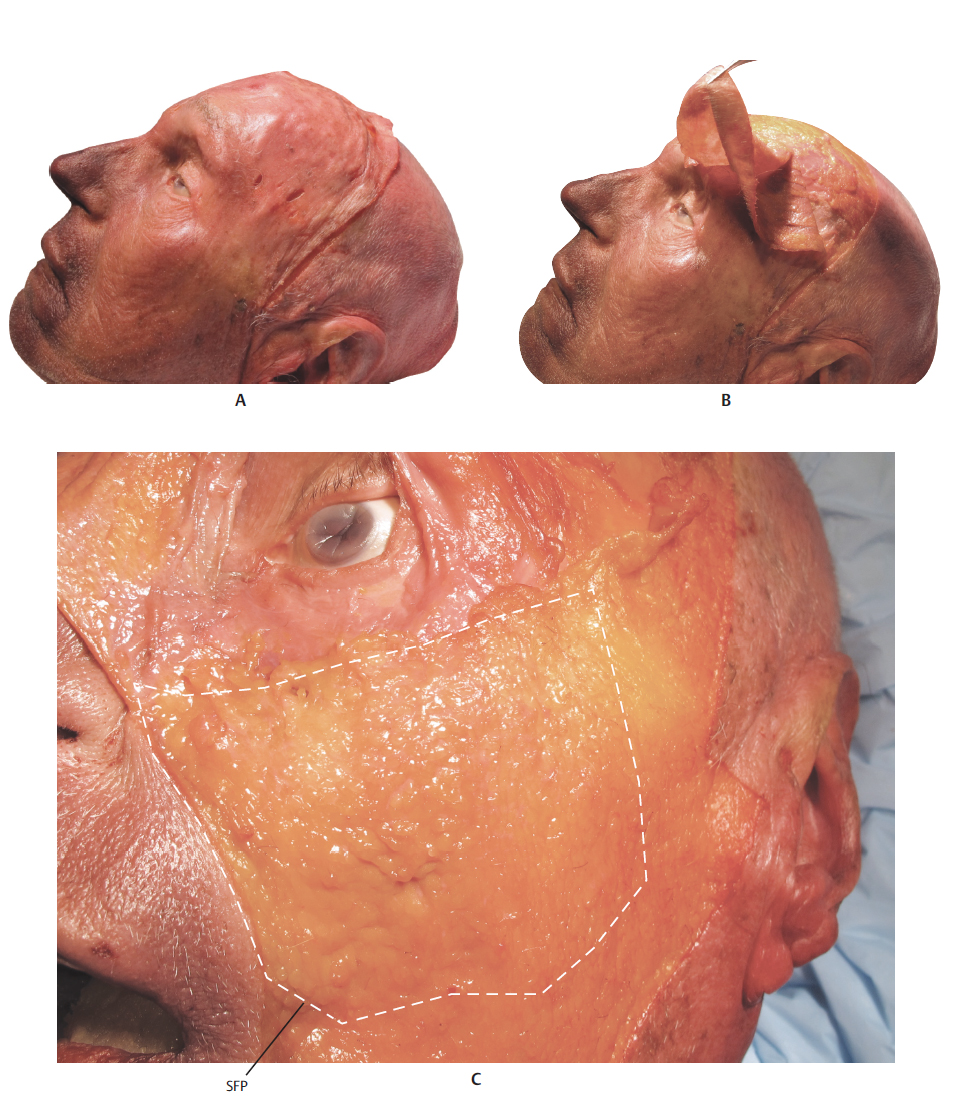
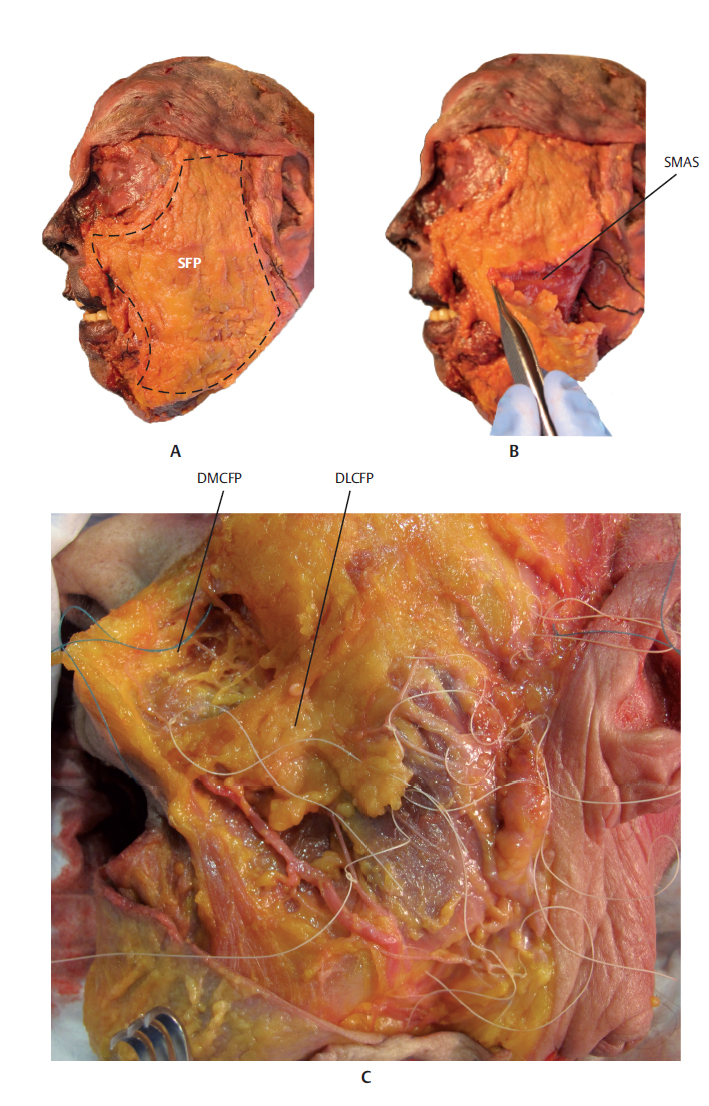
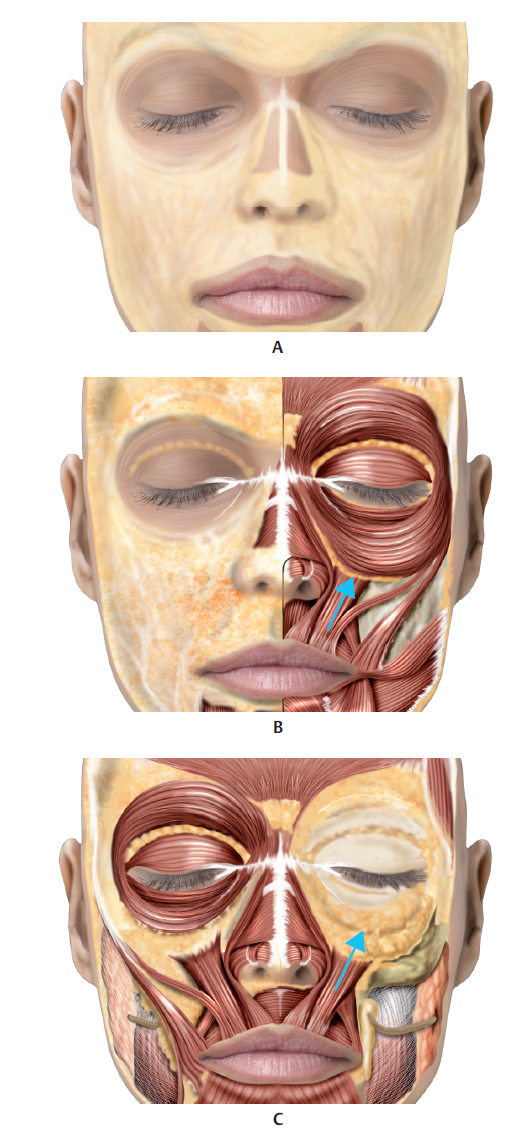
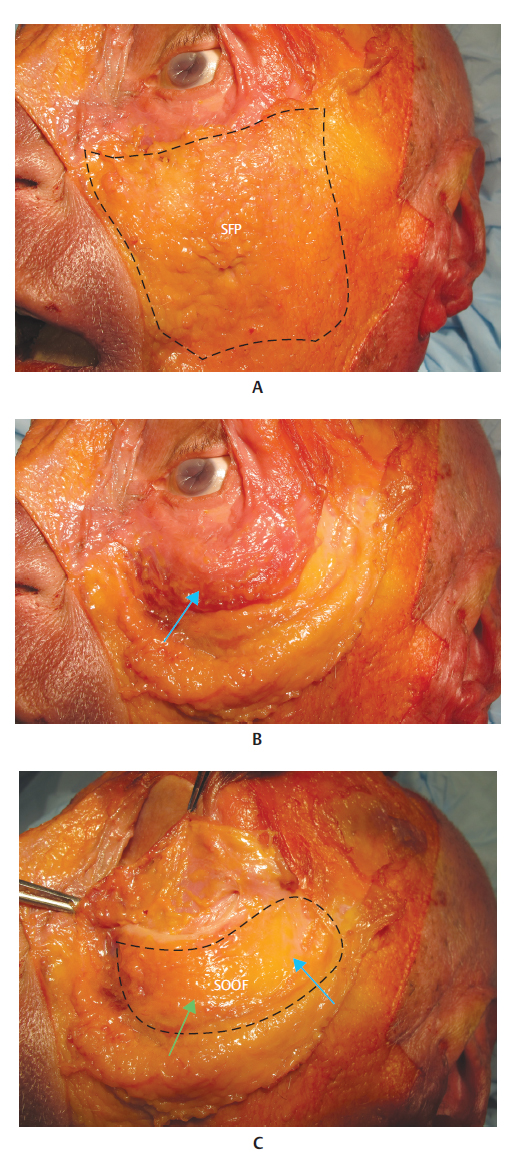
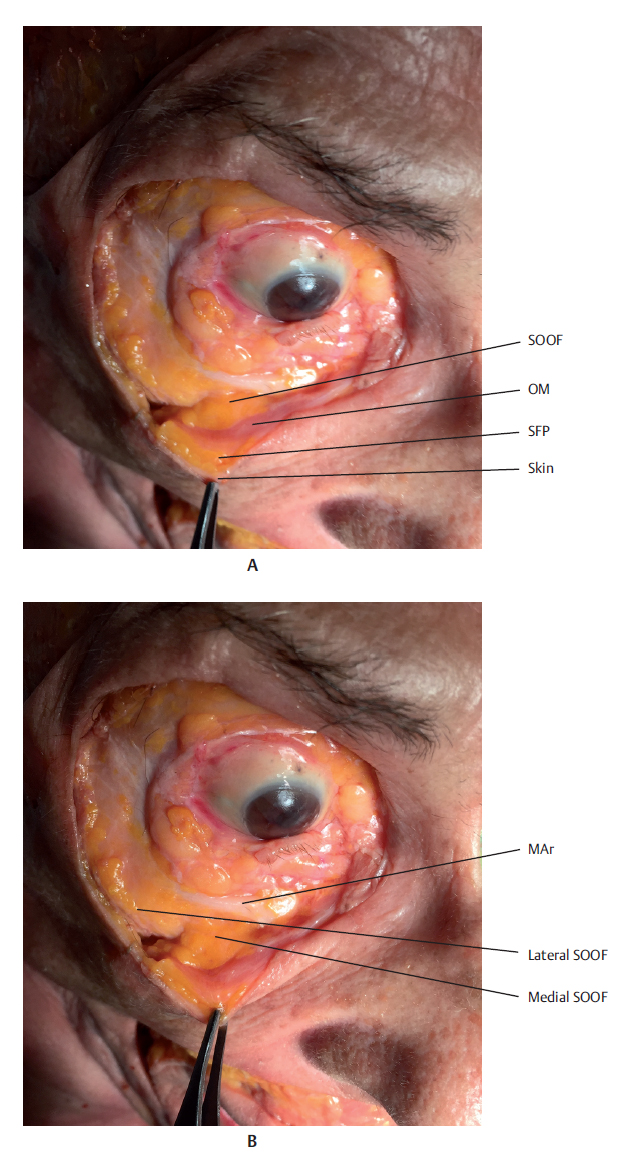
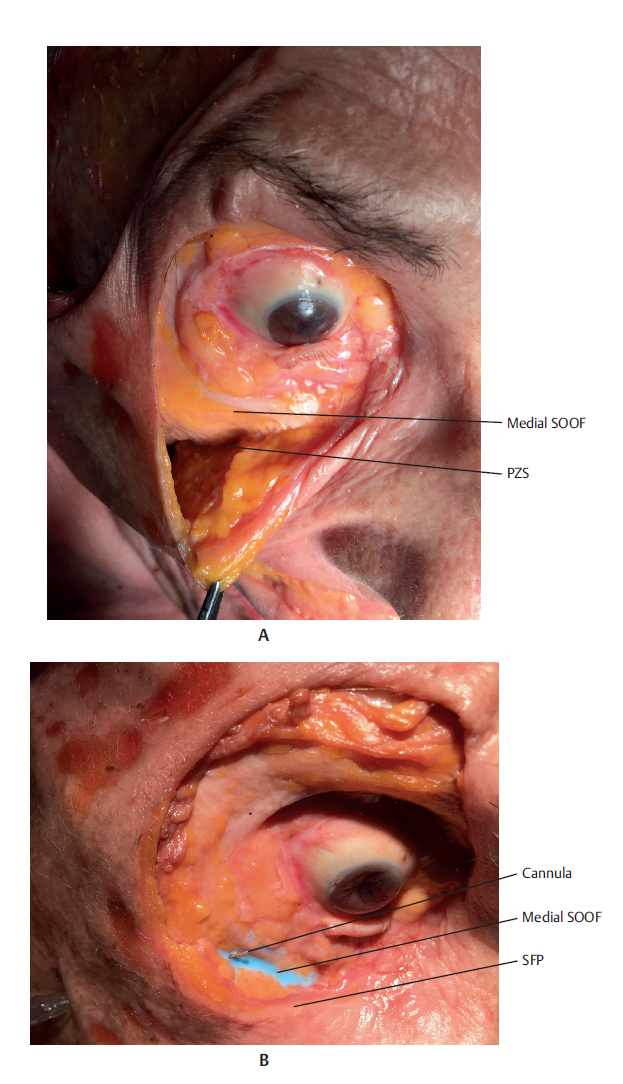
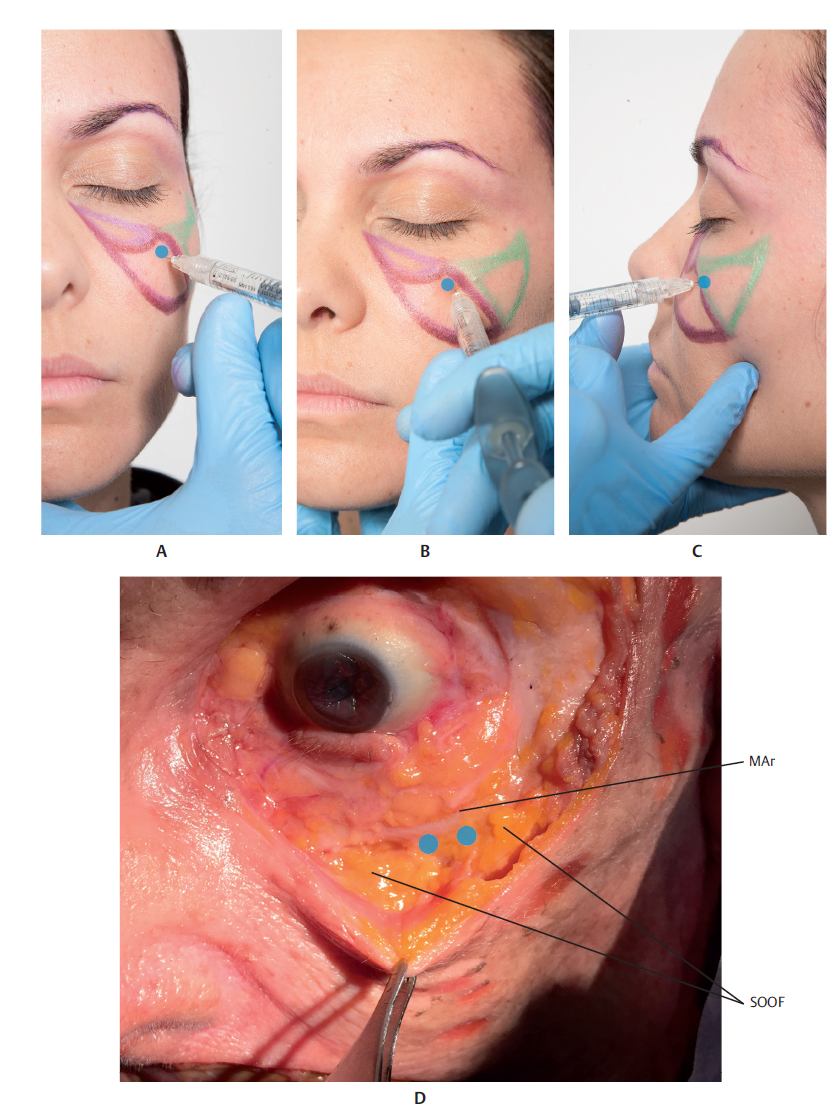
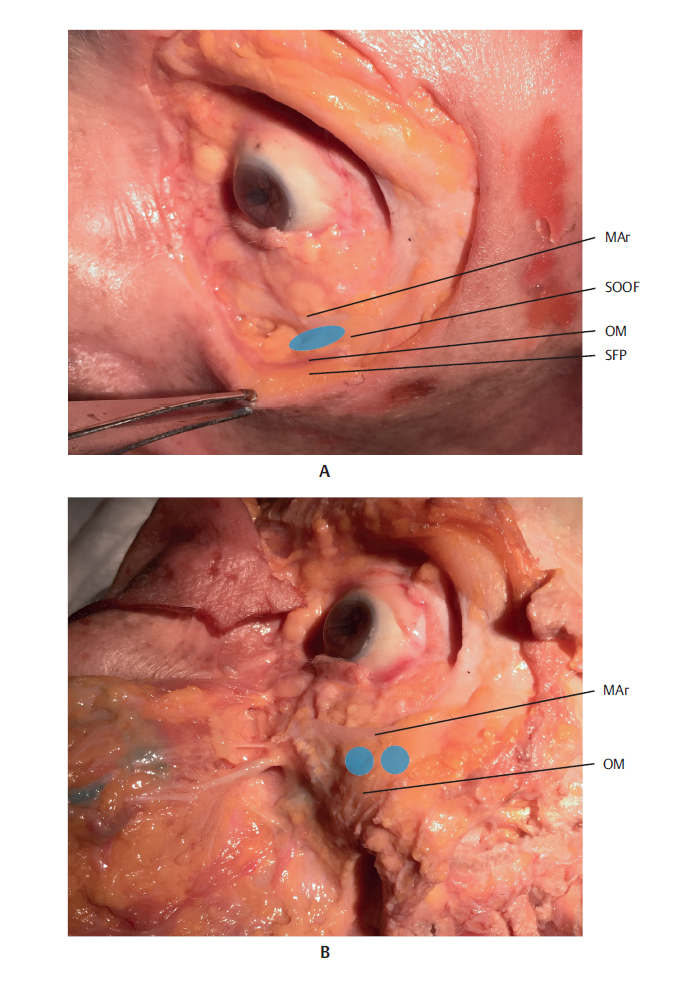
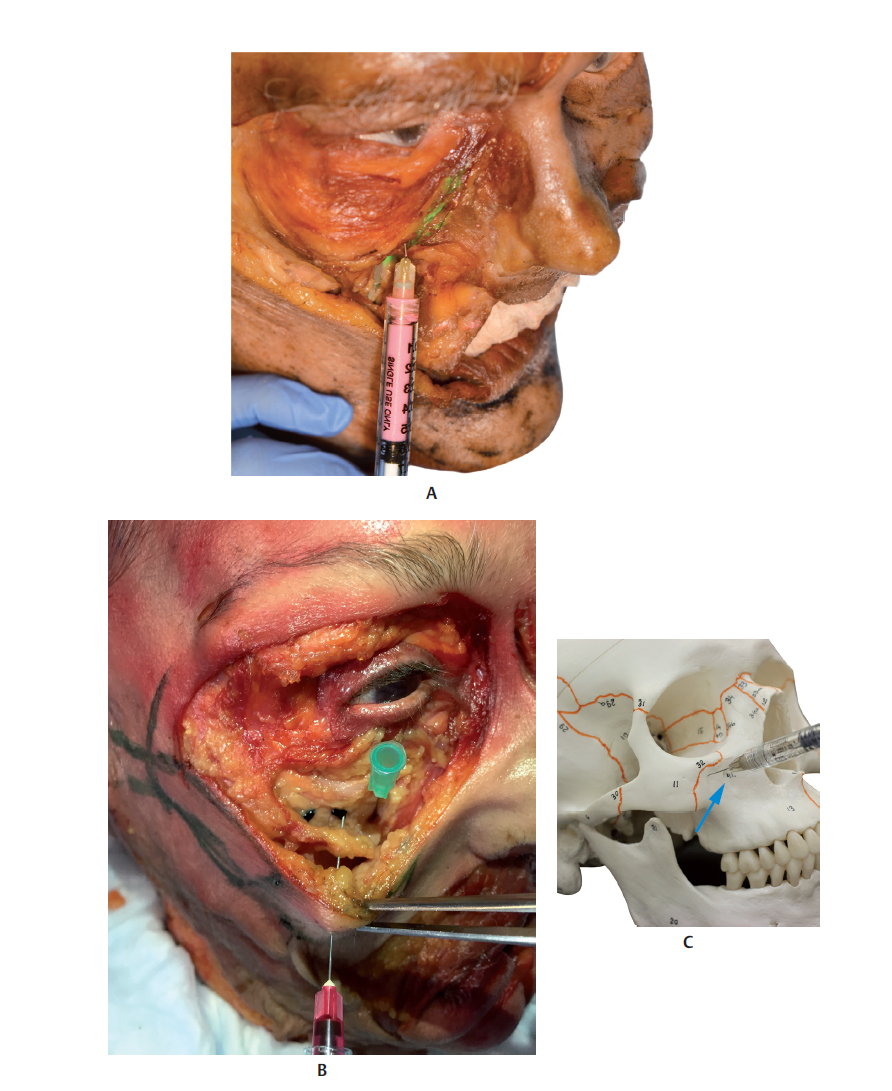
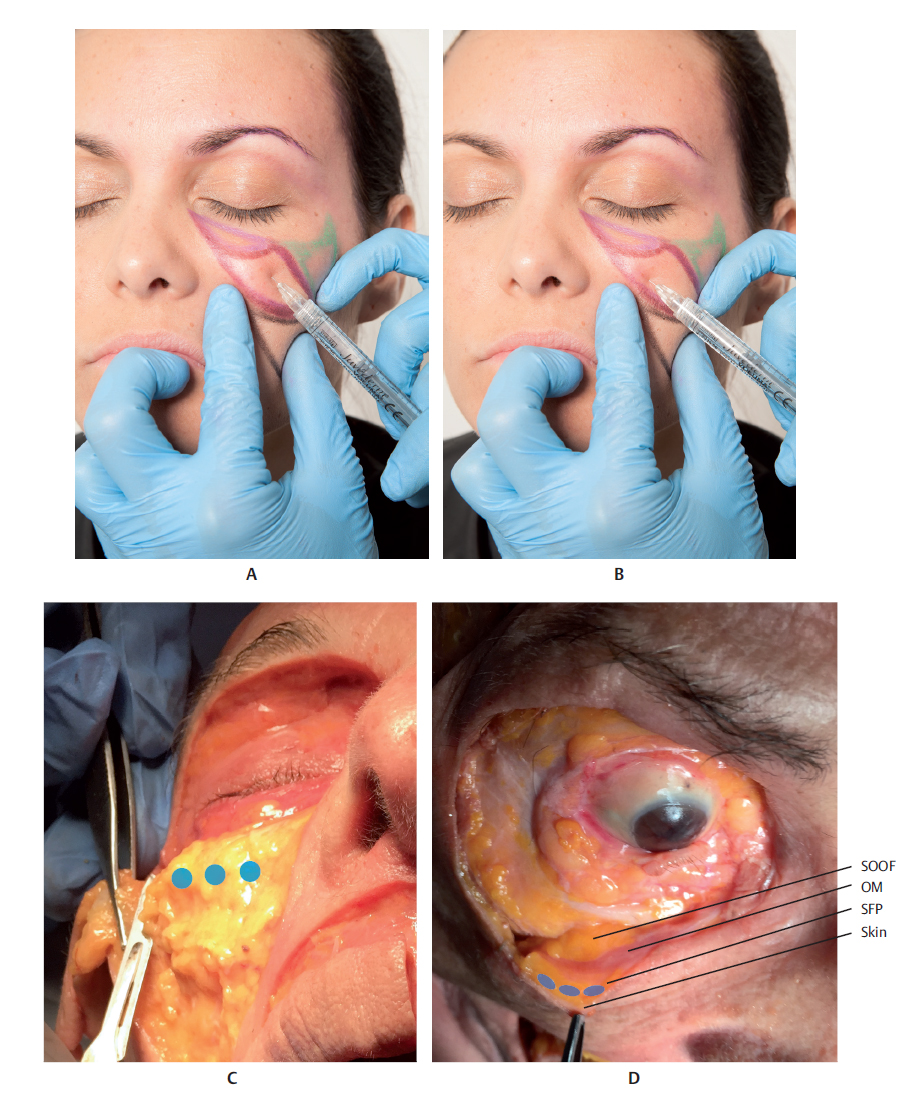
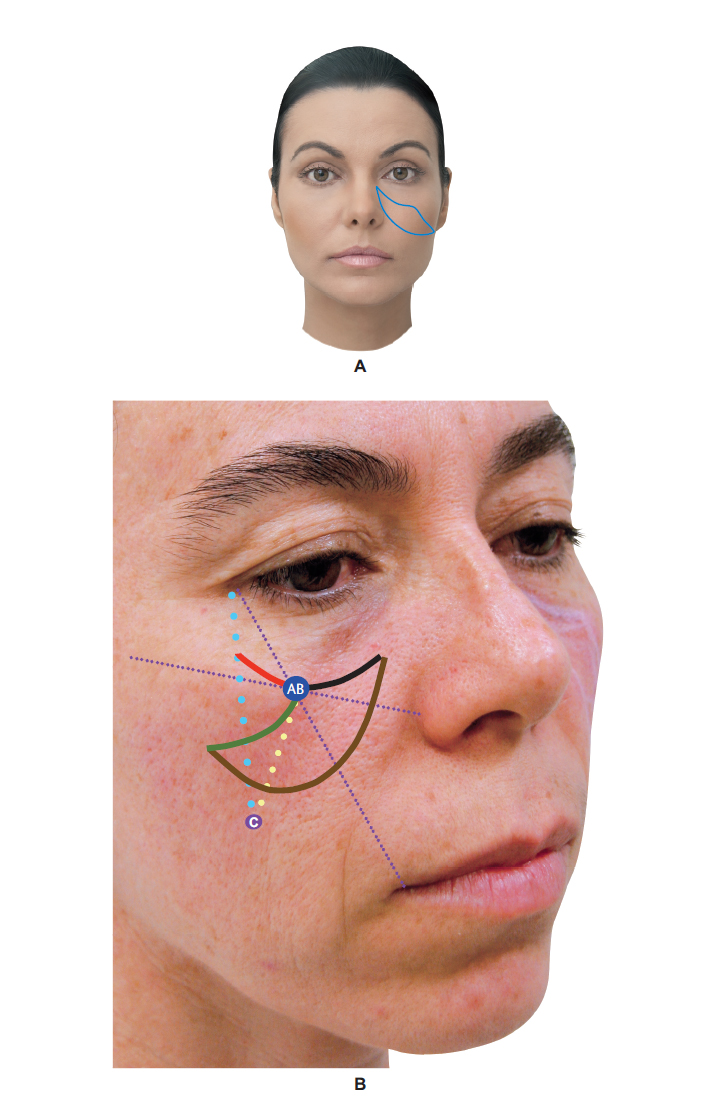
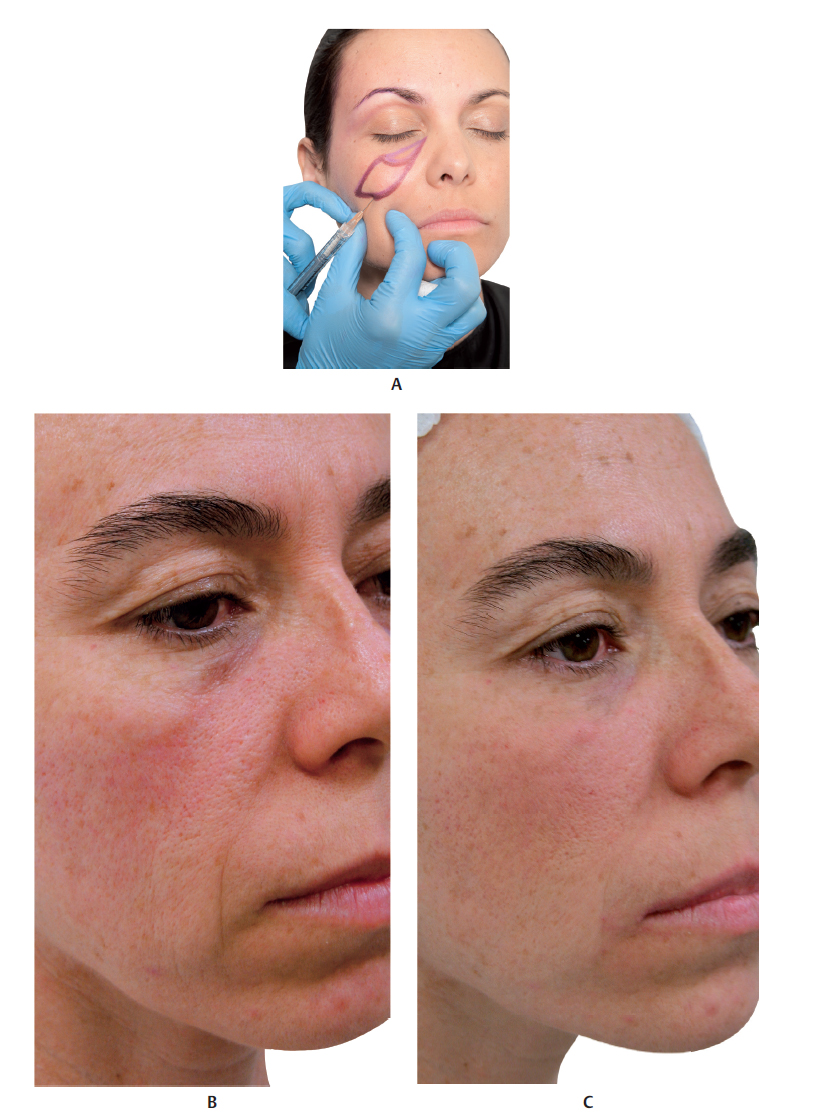
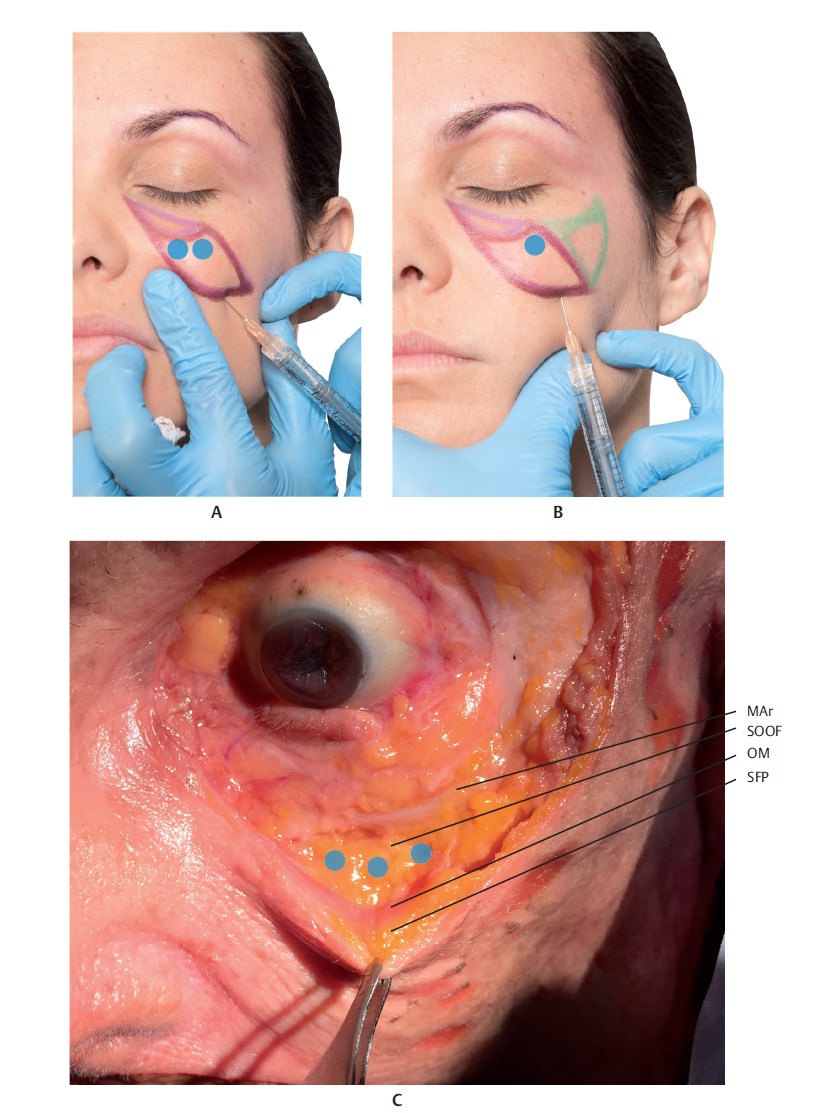
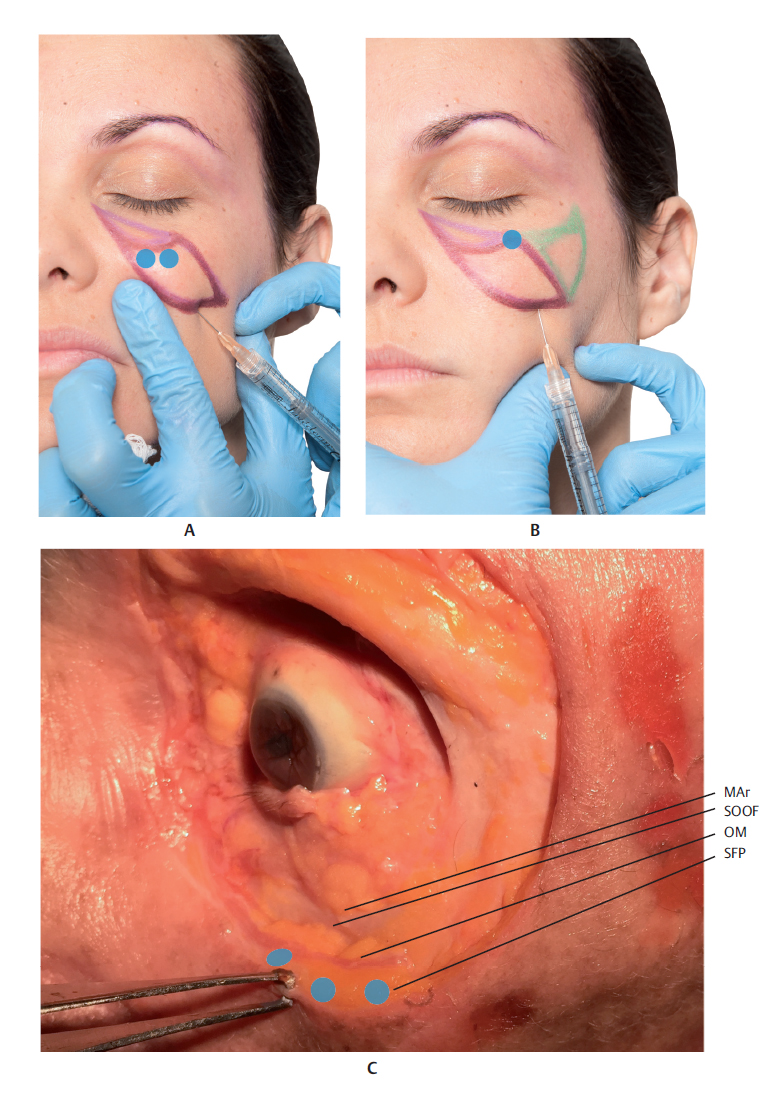
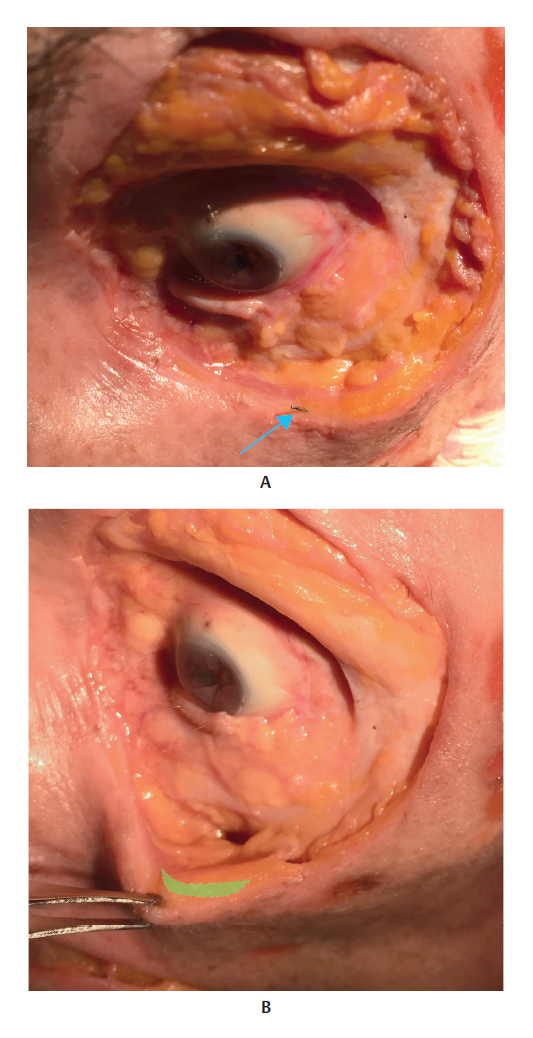
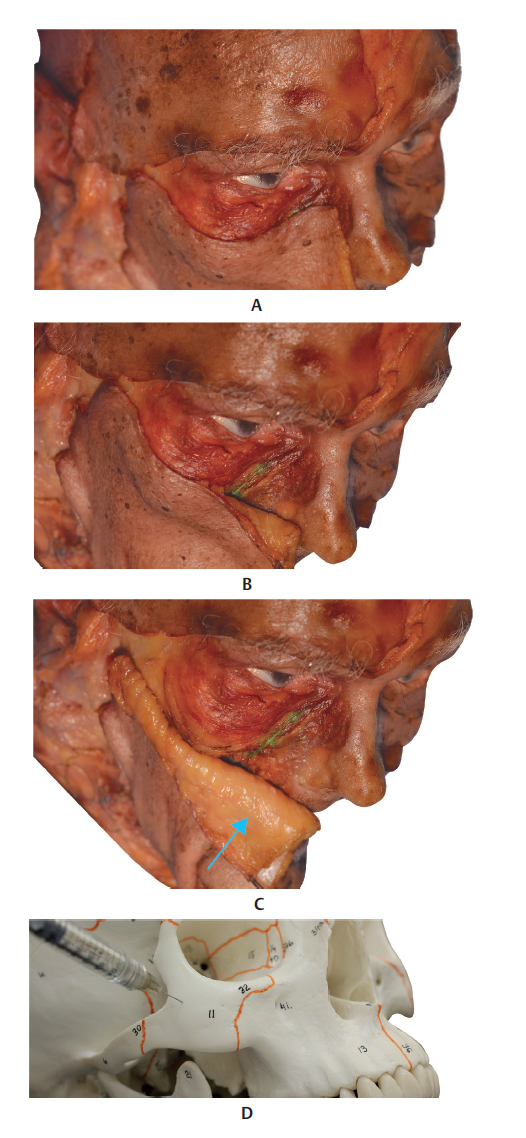
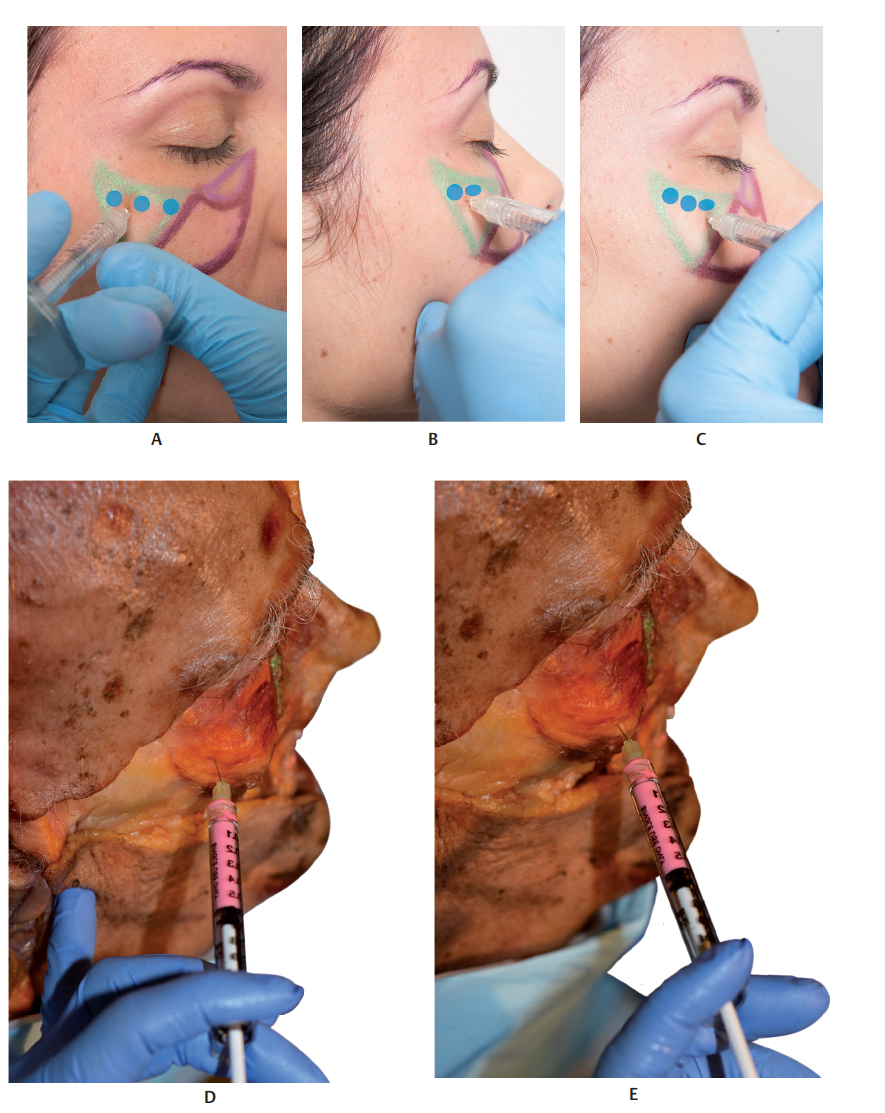
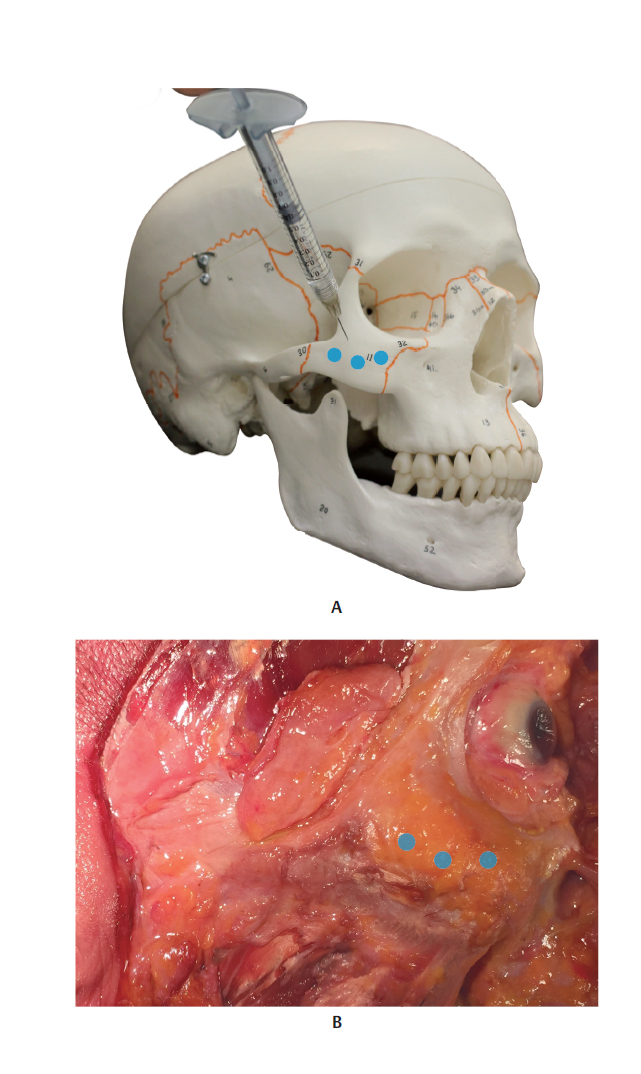
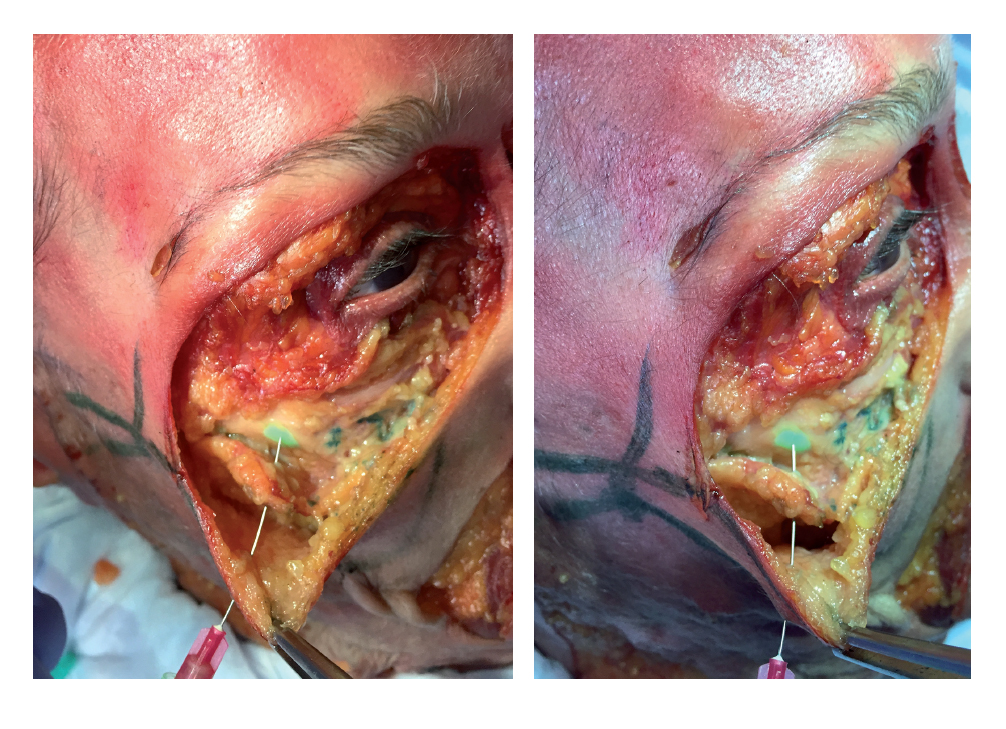
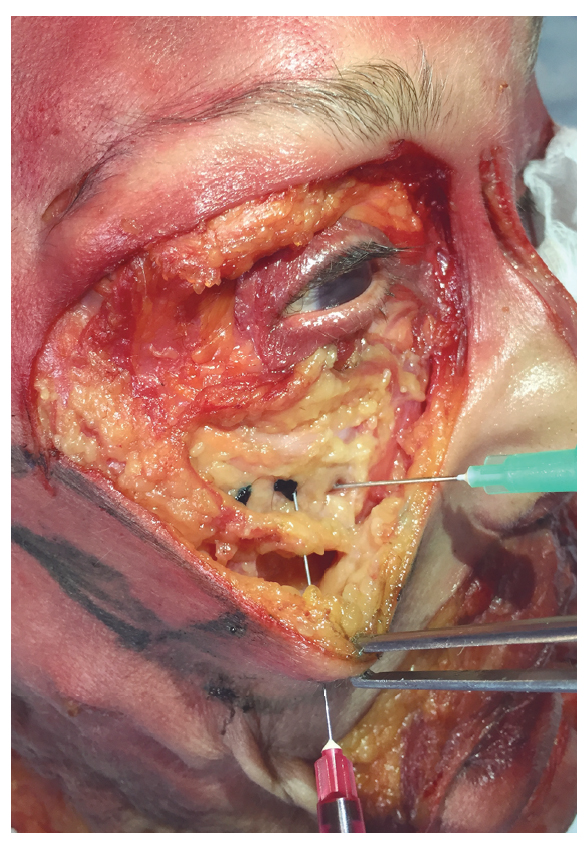
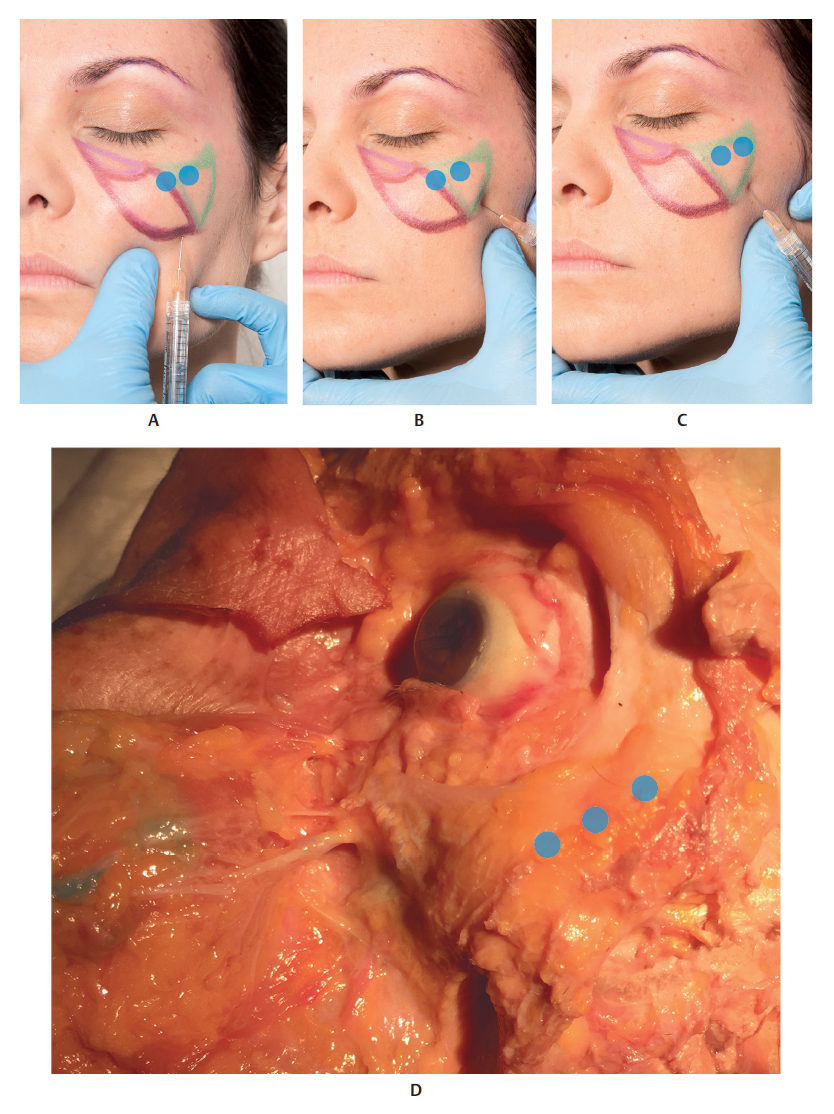
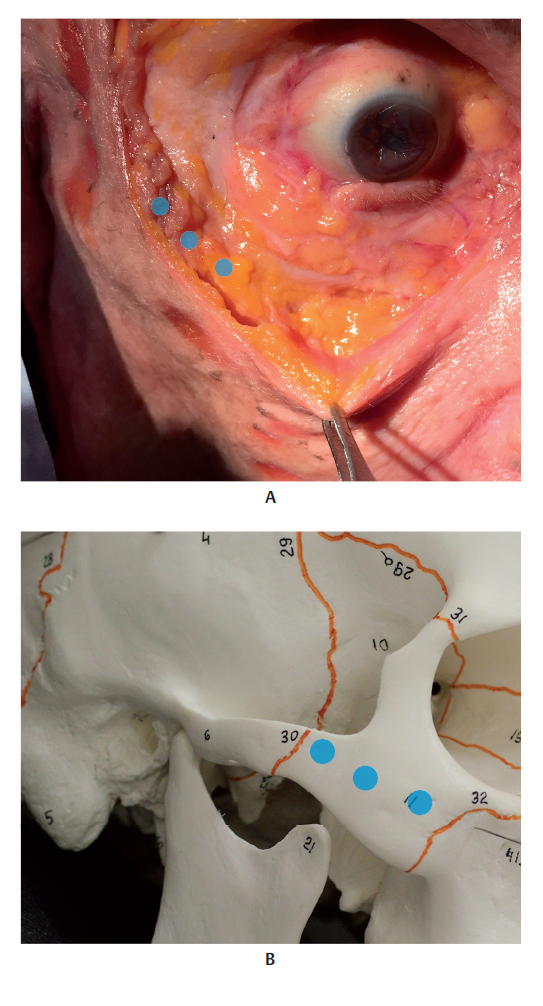
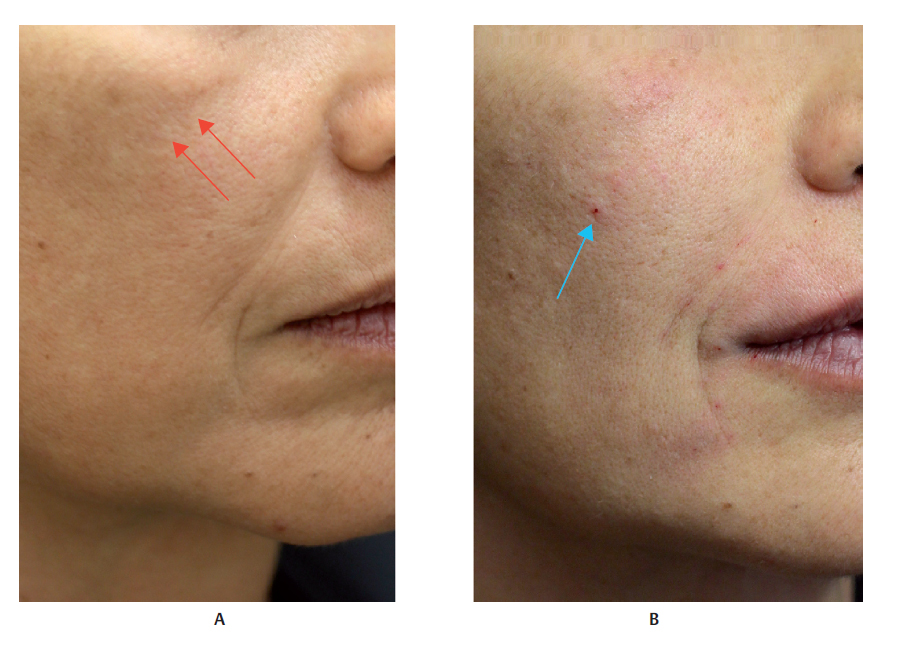
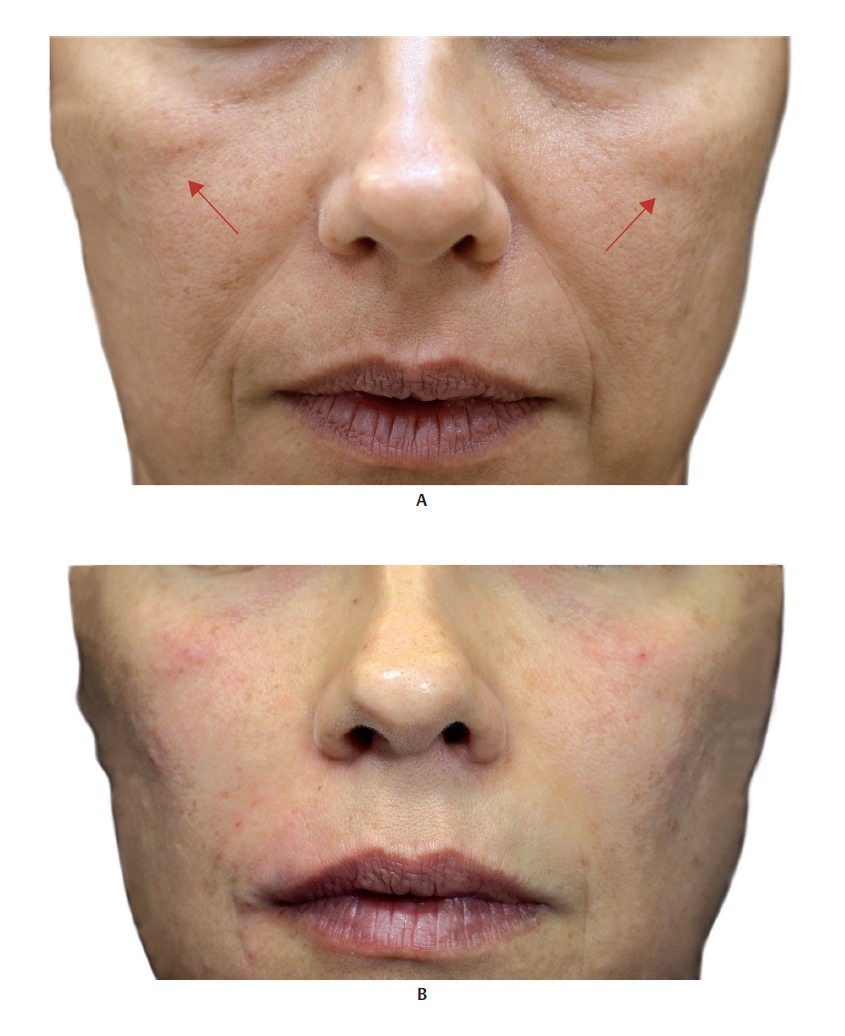
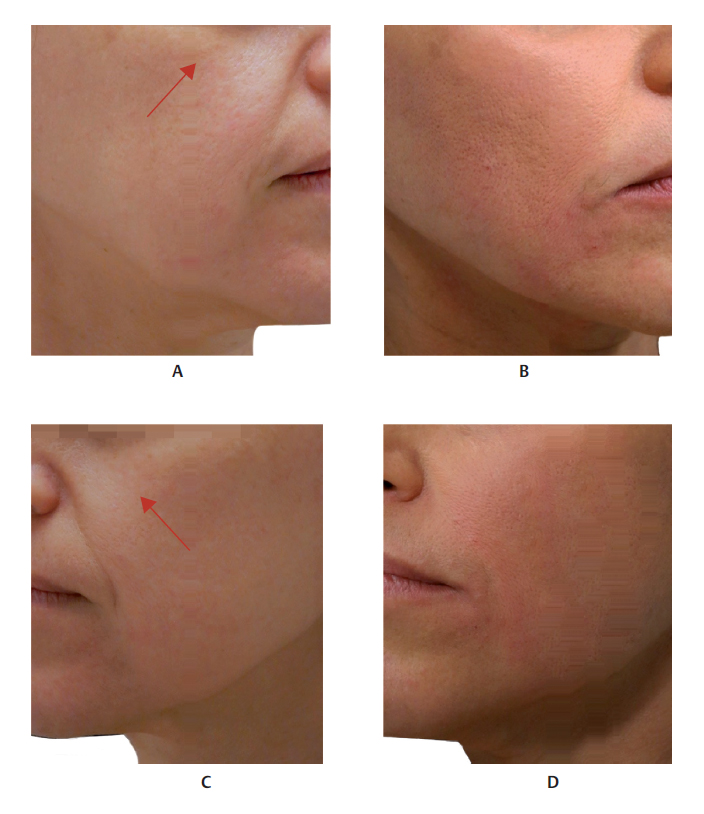
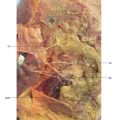
1 Braz AV, Sakuma TH. Midface rejuvenation: an innovative technique to restore cheek volume. Dermatol Surg 2012;38(1):118–1202 Raspaldo H. Volumizing effect of a new hyaluronic acid subdermal facial filler: a retrospective analysis based on 102 cases. J Cosmet Laser Ther 2008;10(3):134–1423 Carruthers JD, Carruthers A. Facial sculpting and tissue augmentation. Dermatol Surg 2005;31(11 Pt 2):1604–16124 Hoff mann K; Juvéderm Voluma Study Investigators Group. Volumizing effects of a smooth, highly cohesive, viscous 20-mg/mL hyaluronic acid volumizing filler: prospective European study. BMC Dermatol 2009;9:95 Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg 2007;119(7):2219–2227, discussion 2228– 22316 Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg 2008;121(6):2107–21127 Whetzel TP, Mathes SJ. Arterial anatomy of the face: an analysis of vascular territories and perforating cutaneous vessels. Plast Reconstr Surg 1992;89(4):591–603, discussion 604–6058 Schaverien MV, Pessa JE, Rohrich RJ. Vascularized membranes determine the anatomical boundaries of the subcutaneous fat compartments. Plast Reconstr Surg 2009;123(2):695–7009 Furukawa M, Mathes DW, Anzai Y. Evaluation of the facial artery on computed tomographic angiography using 64-slice multidetector computed tomography: implications for facial reconstruction in plastic surgery. Plast Reconstr Surg 2013; 131(3):526–53510 Furnas DW. The retaining ligaments of the cheek. Plast Reconstr Surg 1989;83(1):11–1611 Rohrich RJ, Pessa JE. The retaining system of the face: histologic evaluation of the septal boundaries of the subcutaneous fat compartments. Plast Reconstr Surg 2008;121(5):1804–180912 Pilsl U, Anderhuber F, Rzany B. Anatomy of the cheek: implications for soft tissue augmentation. Dermatol Surg 2012;38(7 Pt 2):1254–126213 Ghassemi A, Prescher A, Riediger D, Axer H. Anatomy of the SMAS revisited. Aesthetic Plast Surg 2003;27(4):258–26414 Pessa JE, Garza JR. The malar septum: the anatomic basis of malar mounds and malar edema. Aesthet Surg J 1997;17(1): 11–1715 Andre P, Azib N, Berros P, et al. Anatomy and volumizing injections. Paris: E2e Medical Publishing; 2012Fig. 10.1 A. Anterior view of the malar and zygomatic regions.B. Same region after removal of the skin to expose the superficial fat pads (SFPs).C. Same region after removal of the skin and the SFPs to expose the orbital portion of the orbicularis oculi muscle (OM). The medial suborbicularis oculi fat (SOOF) pad is visiblein yellow posterior to the orbital portion.D. Same region after removal of the skin, SFPs, orbital portion of the orbicularis oculi muscle (OM), and the zygomatic muscles. The medial and lateral SOOF pads are visible.Fig. 10.2 A. Anterior view of the malar and zygomatic regions after removal of the skin, the superficial fat pads (SFPs), and the palpebral and orbital portions of the orbicularis oculi muscle (OM) and zygomatic muscles, exposing the medial and lateral suborbicularis oculi fat (SOOF) pads and the infrapalpebral fat bags.B. Same region after removal of the skin, the SFPs, the palpebral and orbital portions of the OM, the medial and lateral SOOF, levator muscle of the upper lip, and the zygomatic major and minor muscles.C. Same region after removal of the levator muscle of the upper lip and the ala of the nose and the levator muscle of the angle of the mouth.D. Bone structure of the malar and zygomatic regions.Fig. 10.3 A. Anterior view of the left side of the face of a 3D digital model.B. Vessels, arteries, and nerves of the malar and zygomatic regions.Fig. 10.4 Anterior view of the face focusing on the malar and zygomatic regions.A. Corresponding arterial vascularization.B. Corresponding venous vascularization.C. Corresponding innervation.Fig. 10.5 A. Lateral view of the right malar and zygomatic regions.B. Same region showing superficial fat pads (SFPs) after removal of the skin.C. Same region after removal of the skin and the SFPs. The palpebral and orbital portions of the orbicularis oculi muscle (OM) can be seen over the medial and lateral suborbicularis oculi fat (SOOF) pads. The levator muscle of the upper lip and the ala of the nose, the levator muscle of the angle of the mouth, and the zygomatic major and minor muscles are above the deep fat pads (DFPs).D. Same region after removal of the orbital portion of the OM, medial and lateral SOOF pads, SFPs, and DFPs. Part of the buccal fat pad (Bichat’s fat pad) can be seen above the buccinator muscle.E. Bone structure of the malar and zygomatic regions composed of the zygomatic bone and maxilla.Fig. 10.6 Right profile view showing the zygomatic and malar regions.A. Corresponding vascularization and innervation.B. Corresponding arterial vascularization.C. Corresponding venous vascularization.D. Arterial and venous vascularization integrated in the frontal muscle, orbicularis oculi muscle (OM), nasal muscle, zygomatic major muscle, buccinator, and masseter muscle.E. Corresponding innervation.Fig. 10.7 A andB. Anterior view of the malar region.C andD. Close-up ofA andB.Fig. 10.8 A. Right side of the face of a fresh cadaver specimen with skin folded back, exposing the suborbicularis oculi fat (SOOF) pad (black arrow) .B. The skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), and below this, the SOOF fat pad are visible on the left side of the face.Fig. 10.9 Anterior view of the superficial fat pads (SFPs) of the middle third of the face: (1) nasolabial fat pad, (2) medial cheek fat pad, and (3) middle cheek fat pad.Fig. 10.10 A. Left side of the face of a fresh cadaver specimen with intact skin.B. Skin being folded back.C. The superficial fat pad (SFP) of the middle third of the face is exposed.Fig. 10.11 Anterior view of the deep fat pads (DFPs) of the middle third of the face: (1) deep medial cheek fat pad, (2) deep lateral cheek fat pad.Fig. 10.12 A. Left side of the face of a fresh cadaver specimen with exposed superficial fat pad (SFP).B. SFP being folded back.C. SFP folded back. The superficial muscular aponeurotic system (SMAS) is visible, together with the deep fat pads (DFPs) of the middle third of the face, namely, deep medial cheek fat pad (DMCFP) and deep lateral cheek fat pad (DLCFP).Fig. 10.13 A. Anterior view of a 3D digital model with the skin folded back, exposing the superficial fat pads (SFPs) of the face.B. Right side of the face showing the SFP of the face and left side of the face, SFPs of the malar region and the orbicularis oculi muscle (OM) (orbital and palpebral portions) have been folded back. The medial suborbicularis oculi fat (SOOF) pad is also visible behind the OM (blue arrow).C. The orbital portion of the OM was removed from the right side of the face. The two portions of the OM were removed from the left side of the face, exposing the medial and lateral SOOF (blue arrow).Fig. 10.14 A. Left side of the face of a fresh cadaver specimen, exposing the superficial fat pads (SFPs) of the face.B. SFPs folded back and showing the orbicularis oculi muscle (OM), palpebral portions,in light pink, and orbital,in red (blue arrow).C. OM, palpebral and orbital portions have been folded back and the medial (green arrow) and lateral (blue arrow) suborbicularis oculi fat (SOOF) have been exposed.Fig. 10.15 A. Right side of the face of a cadaver specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), and suborbicularis oculi fat (SOOF) pad.B. Skin, SFP, and OM being pulled by the forceps. The medial and lateral SOOF and the marginal arch (MAr) are visible.Fig. 10.16 A. Right side of the face of a cadaver specimen in which the superficial fat pad (SFP), orbicularis oculi muscle (OM), and part of the medial suborbicularis oculi fat (SOOF) pad are being pulled by the forceps. The prezygomatic space (PZS) and another part of the medial SOOF pad are also visible.B. Hyaluronic acid (HA)(light blue) applied using a 25 Gx 40 mm cannula with the deep filler injection technique in the malar region. The tip of the cannula is visible in the medial SOOF posteriorly to the OM.Fig. 10.17 A. Anterior view of the left side of the face of a model showing the area to be filled(dark red markings), using a needle technique in the supraperiosteal plane. 27 GX 13 mm needle inserted into the supraperiosteal plane, and product injected with a bolus technique(blue circle).B andC. In the partial and complete profiles, the supraperiosteal point is proximal to the transition between the anterior malar area and the zygomatic region. Injecting into the more medial plane is dangerous and contraindicated because of the proximity of the infraorbital foramen.D. Left side of the face of a cadaver specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), medial and lateral suborbicularis oculi fat (SOOF) pads, and marginal arch (MAr). There are twoblue circles between the SOOF and the MAr that indicate where the product was injected into the supraperiosteal plane.Fig. 10.18 A. Left side of the face of a cadaver specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), suborbicularis oculi fat (SOOF) pad, and marginal arch (MAr). Theblue ellipse between the SOOF and the MAr indicates where the product was injected into the supraperiosteal plane.B. Skin, SFP, OM, and SOOF pulled forward to expose the MAr and maxillary bone (MB). The twoblue circles mark where the product was injected into the supraperiosteal plane.Fig. 10.19 A. Right side of the face of a cadaver specimen in midprofile with the skin and superficial fat pad (SFP) folded back to show the entire orbicularis oculi muscle (OM). Note the syringe with hyaluronic acid (HA) (pink) and needle introduced into the supraperiosteal plane of the anterior malar region.B. Midprofile specimen with long needle inserted up to the supraperiosteum in the lateral part of the maxillary bone. Application of HA (dark blue), in the supraperiosteal plane. Thegreen needle shows the location of the infraorbital foramen. The skin adhering to the medial malar superficial fat pad and the orbital part of the OM has been removed for better visualization.C. Midprofile view of a cranium with a syringe simulating an injection into the supraperiosteal plane of the anterior malar region in the maxillary bone. The safe limit for injecting into this region is laterally to the infraorbital foramen. Theblue arrow shows the location of the foramen.Fig. 10.20 A andB. Left side of the face of a model showing the malar region to be filled(dark red markings). 27 GX 13 mm needle inserted into the subcutaneous plane and product injected with a bolus technique.C. Right side of the face of a fresh cadaver specimen with skin folded back to show the superficial fat pad (SFP) of the middle third of the face, where hyaluronic acid (HA) was injected(three blue circles).D. The skin, SFP, orbicularis oculi muscle (OM), and suborbicularis oculi fat (SOOF) pad are visible. HA was injected into the SFP of the middle third of the face(blue ellipses).Fig. 10.21 A. The malar region to be treated has been marked.B. Mark the anterior malar region or zygomatic region for treatment (depending on the case). The area where volume has been lost is marked using an imaginary line from the lateral commissure of the eye to the oral commissure, and another imaginary line from the tragus to the superior ala of the nose. Point AB represents the intersection of these lines. A concave line (black) is marked from point AB, delimiting the inferior portion of the nasojugal groove. Another concave line (green) is marked from point AB, going around the posteroinferior portion of the zygomatic bone. Finally, a convex line (brown) is marked to show the anterior limit of the loss of volume above the nasolabial fold. Point “C” is ~ 4 cm from point “AB” (line parallel to the nasolabial fold). Point “C” shows the site where the orifice should be made for inserting the cannula.Fig. 10.22 A. Right midprofile view of a model showing the malar area to be filled (dark red markings) and 25 G cannula simulating an injection in the malar region.B andC. Right midprofile view of a patient before and after injection of hyaluronic acid (HA) with a 25 G cannula in the anterior malar region, in the superficial medial cheek fat pad, and the suborbicularis oculifat (SOOF) pad.Fig. 10.23 A. Anterior view of the left side of the face of a model showing the malar region to be filled(dark red markings). 25 GX 40 mm cannula inserted into the submuscular plane and product injected using a bolus technique(blue circle) in the superior region, and retrograde injection in the inferior portion.B. The model in the same position with tip of the cannula positioned laterally, in the transition between the anterior malar region and the zygomatic region.C. Left side of the face of a cadaver specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), medial and lateral suborbicularis oculi fat (SOOF) pads, and marginal arch (MAr). There are threeblue circles between the OM and the MAr, indicating where the product was injected into the medial SOOF, in the prezygomatic space.Fig. 10.24 A. Left side of the face of a specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), and medial suborbicularis oculi fat (SOOF) pad. The tip of the 25 GX 40 mm cannula can be seen in the medial SOOF, where the product should be injected(blue arrow). When the loss of volume is severe, the prezygomatic plane can be chosen for treatment, as it is deeper.B. Specimen with 25 GX 40 mm cannula inserted into the medial SOOF with hyaluronic acid (HA)(light blue).C. Specimen with skin, SFP, OM, and SOOF pulled anteriorly. Note the injection of HA(light blue) with the cannula anterior to the marginal arch (MAr), in the prezygomatic space.Fig. 10.25 A. Left side of the face of a model showing the malar region to be filled(dark red markings). 25 GX 40 mm cannula inserted into the supramuscular plane and product injected with a bolus technique(blue circle).B. The model in the same position with tip of the cannula positioned laterally, in the transition between the anterior malar region and the zygomatic region.C. The superficial fat pad (SFP), orbicularis oculi muscle (OM), medial and lateral suborbicularis oculi fat (SOOF) pads, and marginal arch (MAr) are visible. Note the threeblue circles in the SFP between the skin and the OM, indicating where the product was injected.Fig. 10.26 A. Left side of the face of a cadaver specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), medial suborbicularis oculi fat (SOOF) pad, and marginal arch (MAr). The tip of a 25 GX 40 mm cannula can be seen in the SFP, where the product should be injected(blue arrow). When the loss of volume is severe, the deeper plane (SOOF and prezygomatic space) can also be chosen for treatment.B. Fig.A with hyaluronic acid (HA)(green) in the medial malar SFP.Fig. 10.27 A andB. Anterior view of a 3D digital model showing the area to be filled in the zygomatic region (blue markings).C andD. Close-ups ofA andB.Fig. 10.28 A. Right side of the face of a fresh cadaver specimen exposing the palpebral part of the orbicularis oculi muscle (OM).B. Skin and superficial fat pad (SFP) being folded back and exposure of the OM more medially.C. Right side of the face of a cadaver specimen with the skin being folded back, exposing the SFP of the middle third of the face (blue arrow) . The entire OM (palpebral and orbital portions) is visible.D. Right midprofile view of a cranium with a syringe indicating the application in the supraperiosteal plane of the zygomatic bone.Fig. 10.29 A,B, andC. Right side of the face of a model in three different profile positions, showing the zygomatic area to be filled(greenmarkings). 27 GX 13 mm needle inserted in the supraperiosteal plane, and the product injected with a bolus technique(blue circles).D andE. Right side of the face of a fresh cadaver specimen with skin and superficial fat pads (SFPs) folded down, exposing the entire orbicularis oculi muscle (OM). Note the syringe with the needle inserted into the supraperiosteal plane of the zygomatic region in two different positions.Fig. 10.30 A. Right midprofile view of a cranium with syringe simulating a bolus application in the supraperiosteal plane of the zygomatic bone.B. Right side of the face of a fresh cadaver specimen in which the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), and part of the suborbicularis oculi fat (SOOF) pad have been folded back. Part of the SOOF pad and zygomatic arch are visible. The threeblue circles mark where the product was injected into the supraperiosteal plane.Fig. 10.31 Right side of the face of a fresh cadaver specimen with long needle inserted up to the supraperiosteum of the zygomatic bone and showing application of hyaluronic acid (HA) (light green). The skin adhering to the superficial middle cheek fat pad, orbital part of the orbicularis oculi muscle (OM), lateral suborbicularis oculi fat (SOOF) pad, and prezygomatic space (prezygomatic fat) were removed for better visualization of the zygomatic bone.Fig. 10.32 Right side of the face of a fresh cadaver specimen with a long needle inserted up to the supraperiosteum of the zygomatic bone. Application of hyaluronic acid (HA) (dark blue) at the junction between the zygomatic process and the maxillary bone, and also in the maxillary bone more medially, lateral to the infraorbital foramen, in the supraperiosteal plane. The infraorbital foramen is marked by thegreen needle. The skin adhering to the medial malar superficial fat pad (SFP), orbital part of the orbicularis oculi muscle (OM), lateral suborbicularis oculi fat (SOOF) pad, and prezygomatic space (prezygomatic fat) were removed for better visualization of the zygomatic bone.Fig. 10.33 A, B, andC. Left side of the face of a model withlight green markings delimiting the zygomatic arch. 25 Gx 40 mm cannula inserted into the submuscular plane and orifice made as explained in Fig. 10.21. The product was injected using a bolus technique(blue circles) in the superior part, and retrograde injection in the inferior part.D. Left side of the face of a cadaver specimen in which the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), and part of the suborbicularis oculi fat (SOOF) pad have been folded back. Part of the SOOF pad and zygomatic arch are visible. The threeblue circles mark where the product was injected into the submuscular plane.Fig. 10.34 A. Right side of the face of a fresh cadaver specimen exposing the skin, superficial fat pad (SFP), orbicularis oculi muscle (OM), suborbicularis oculi fat (SOOF) pad, and marginal arch (MAr). The threeblue circles between the SOOF and the MAr indicate where the product was injected into the submuscular plane, in the zygomatic region.B. Right midprofile view of a cranium with threeblue circles marking where the product was injected into the zygomatic bone, in the submuscular plane.Fig. 10.35 A. Right side of the face of a patient withindication for a filler injection of the malar region. The shadows in the region indicate atrophy of the fat pads (red arrows).B. Patient after filler injection in the malar region with volumizing hyaluronic acid (HA). Note the correction of shadows visible inA and the orifice made for inserting the cannula (blue arrow).Fig. 10.36 A. Anterior view of a patient with indication for a filler injection of the malar region. Note the shadows in the region that indicate atrophy of the fat pads (red arrows) and appearance of the nasolabial fold.B. Patient after filler injection in the malar region with volumizing hyaluronic acid (HA). The shadows seen inA have been corrected and the nasolabial fold has been improved.Fig. 10.37 A. Right side of the face of a patient with indication for a filler injection of the malar region. Note the shadows in the region that indicate atrophy of the fat pads (red arrows) and appearance of the nasolabial fold.B. Patient after filler injection in the malar region with volumizing hyaluronic acid (HA). The shadows visible inA have been corrected.C. Left side of the face of a patient with indication for a filler injection of the malar region. Note the shadows in the region that indicate atrophy of the fat pads (red arrows) and appearance of the nasolabial fold.D. Patient after filler injection in the malar region with volumizing hyaluronic acid (HA). Note that the shadows visible inC have been corrected.
____________
a The facial artery originates at the external carotid, crosses the inferior border of the mandible, anteriorly to the masseter muscle; it then divides into the inferior and superior labial branches and continues ascending over the levator muscle of the upper lip and the ala of the nose. It anastomoses with the infraorbital artery, and ends in the medial commissure as the angular artery.b At the level of the parotid gland, the superficial temporal artery divides into two branches that supply the malar region: the transverse facial artery and the zygomatic-orbital artery. The transverse facial artery divides into two branches: the superior branch flows 5 to 26 mm (mean 14 mm) below the zygomatic arch, branching into the superior masseter muscle, zygomatic major muscle, and malar region.c The zygomatic ligament comprises robust fibers measuring 6 to 8 mm, which originate at the inferior edge of the anterior portion of the zygomatic arch below the origin of the zygomatic minor muscle, and insert directly into the skin as a point of anchor. It is important from surgical point of view, when the skin needs to be pushed forward, but can be absent in up to 10% of patients
Only gold members can continue reading. Log In or Register to continue