Chapter 10 AN OVERVIEW OF FAT GRAFTING TECHNIQUES
It has long been recognized that fat is an ideal filler for the human body and face when soft tissue augmentation is necessary. Advantages include the fact that fat can be harvested easily, repeatedly, and cost effectively. 1 Many advances and refinements in fat grafting techniques have been developed to overcome the low survival rate of fatty tissue after grafting and to increase the long-term success rate by maintaining more adipocyte viability, preparing the recipient site, mastering injection techniques, and improving the overall efficiency of the entire procedure.
In this chapter we will provide an overview on fat grafting techniques for autologous fat grafting based on the most recent scientific studies by many investigators. To better summarize the fat grafting procedure, basic fat grafting techniques can be arbitrarily classified into four essential components: (1) harvesting autologous fat; (2) processing the harvested lipoaspirate; (3) preparing the recipient site; and (4) injecting the purified fat in small parcels in a specific way. We will also address a number of other important considerations. An important aim for the future is to develop the best possible standardized technique for fat grafting that is scientifically sound and is supported by most recent well-conducted studies.
DIFFERENT TECHNIQUES BASED ON THE VOLUME REQUIRED
Fat grafting can be divided into three categories based on the volume for recontouring or reconstruction: (1) small-volume fat grafting (less than 100 cc) is performed primarily for facial rejuvenation or for regenerative purposes; (2) large-volume fat grafting (100 to 200 cc) is performed primarily for contouring of the breast and body; and megavolume fat grafting (more than 300 cc) is performed primarily for buttock augmentation and breast augmentation or reconstruction. 2 However, for the purposes of review in this chapter, we will address fat grafting techniques primarily for smaller- or larger-volume fat grafting.
Basic Fat Grafting Techniques
Basic fat grafting techniques include fat harvesting, processing, preparation of the recipient site, and placement of fat grafts. However, fat grafting technique can also be divided into smaller and larger fat grafting based on the volume needed. Each category may have its own respective technique that is specifically developed for the procedure. 3
HARVESTING
Small-Volume Graft Harvesting Technique: Atraumatic Low Negative Pressure Method
Syringe aspiration rather than the standard liposuction approach is supported by more recent studies as a relatively less traumatic method for harvest of fat for autologous grafting and should be considered as a standardized technique of choice, at least for small quantities of lipoaspirate. 4 , 5 However, this technique can be time consuming even for experienced surgeons, and a large quantity of fat grafts may not easily be obtained with this technique. The appropriate size of cannula and syringe used for aspiration to harvest fat grafts remains controversial. A comprehensive study has concluded that the viability of fat grafts is significantly better when fat is harvested with a 2 mm diameter cannula with a blunt tip and several side-holes connected to a 10 cc syringe. The use of a smaller syringe (10 cc) is advisable to maintain a minimal negative pressure during harvesting. 4
The syringe aspiration method, better known as the Coleman technique, is especially useful and predictable for small-volume fat grafting and has been widely used by many surgeons. 3 , 5 , 6 Placement of 2 to 3 mm incisions for harvesting fat can be done with a No. 11 blade in locations in which the scars can easily be concealed. Fat grafts can be harvested through the same incision made for infiltration of the anesthetic solution. A small clamp is used to dilate the underlying subcutaneous tissue through the incision to allow insertion of the harvesting cannula with ease. The anesthetic solution is then infiltrated to the donor site 10 to 15 minutes before fat extraction, which makes harvesting of fat graft easier and less traumatic. The ratio of aspirated fat to tumescent solution should be about 1:1 so that each pass of fat extraction can be more efficient. Pretunneling can be performed after infiltration of an anesthetic solution to make fat harvesting easier and less time consuming.
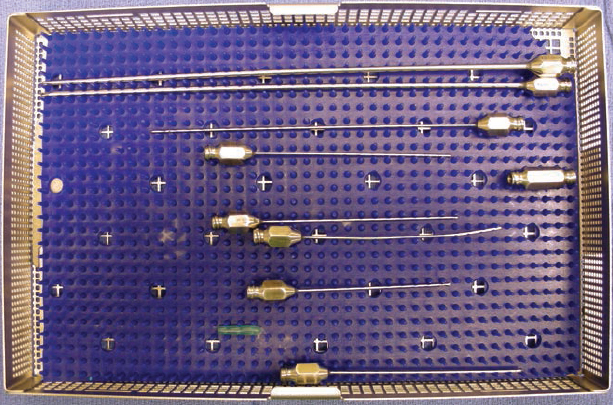
Different sizes and shapes of cannulas are used as needed for fat harvest (small volume) and injection; the forked-tip cannula can be used to release fibrotic tissue, scar, or adhesion.
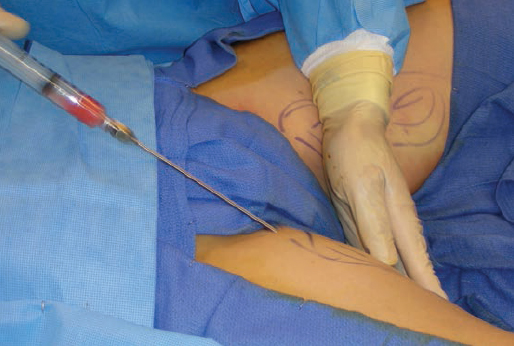
A 10 cc Luer-Lok syringe is connected to a harvesting cannula. We prefer a 10 cc syringe to a larger one, because the 10 cc syringe is less cumbersome in the hand. We use a harvesting cannula that is 15 cm long with a blunt tip and has dual openings like the shape of a bucket handle. Gently pulling back on the plunger creates a 2 cc space vacuum negative pressure in the syringe. With a gentle back-and-forth movement of the syringe, the fat is gradually collected inside the syringe; this method causes minimal trauma to the lipoaspirate. If little fat with too much fluid is drawn up in the syringe, the fluid can be easily pushed out from the bottom of the syringe in a vertical position, and fat extraction can continue. After harvest, all incision sites are closed with interrupted sutures once excess tumescent fluid or blood has been milked out. In general, fat grafts of less than 100 cc can be harvested effectively with this method.
Large or Megavolume Graft Harvesting: Low Suction Pressure Liposuction Technique
For harvest of a large quantity of fatty tissue, one study showed that fat harvested with low-pressure aspiration (lower than 250 mm Hg) yields a higher viable adipocyte count than lipoaspirate harvested with a high-pressure method (greater than 760 mm Hg). 7 Several manufacturers have attempted to develop an “ideal” device that combines fat harvest, processing, and transfer. 8 Unfortunately, only a few such devices have been studied comprehensively for their reliability and superiority, and the findings of these studies are still less than convincing. 9 , 10
One example is the LipiVage device for fat harvest, washing, and transfer (Genesis Biosystem, Inc., Lewisville, TX). 8 It may have certain benefits for less-experienced surgeons for harvesting and processing fat grafts so that their results can be more consistent in terms of adipocyte viability and intact structure. Several other closed devices have recently been developed and used clinically by surgeons. They are the PureGraft system (a closed system with washing and filtration from Cytori Therapeutics, San Diego, CA), 9 the Revolve system (a closed fat-processing system from LifeCell, Branchburg, NJ), 10 and the LipoKit (a closed and manual system with centrifugation from Medi-Khan, West Hollywood, CA). 11 Each of these devices, which combine fat harvesting with processing, may have the potential for use in large-volume fat grafting in the future. However, the usefulness of these devices has not been well accepted by surgeons because of their cost and unconfirmed effectiveness.
Khouri et al 12 advocated low-pressure (300 mm Hg) vacuum liposuction with a specially designed device (the K-VAC syringe from Lipocosm, Key Biscayne, FL) to harvest fat with constant low pressure and a low g force (15 g for 2 to 3 minutes) using hand-cranked centrifugation for megavolume fat harvesting and processing.

A newly designed harvesting cannula by Khouri et al may have many advantages because of its efficiency and less trauma to adipocytes. Such a cannula can be incorporated into a large-volume fat grafting instrument set and can be used in conjunction with lower suction pressure for large-volume fat graft harvest.
PROCESSING
Several methods for processing harvested fat have been proposed, including decanting, cotton gauze rolling, centrifugation, and washing and filtration, to effectively remove the infiltrated anesthetic solution and cell debris within the lipoaspirate and to obtain more concentrated fat for grafting. 13 The best method for performing this stage is the most controversial topic in fat grafting. Most debate concerns whether centrifugation of the lipoaspirate is necessary for fat graft processing.
Processing Harvested Fat With Centrifugation
Centrifugation, as part of the Coleman technique, is our preferred method for processing lipoaspirate, since most studies support its clinical application. 5 , 6 There are several advantages to centrifugation. More viable adipocytes are found at the bottom of the middle layer after centrifugation even with a force of 50 g for 2 minutes based on viable cell counts, and this makes manipulation of the fat graft easier and results in measurably more reliable viability of the grafted tissue. 14 , 15 Recent studies have shown that proper centrifugation can concentrate not only adipocytes and ADSCs but also several angiogenic growth factors within the processed lipoaspirate. 11 , 16 Because a higher content of stem cells or angiogenic growth factors positively correlates with fat graft survival both in experimental and clinical studies, 17 centrifugation at 3000 rpm (about 1200 g) for 3 minutes appears to offer more benefits, because it is effectively concentrating adipocytes, ADSCs/progenitor cells, and angiogenic growth factors. Allen et al, 18 investigating optimal density in an animal study, reported that higher-density fat grafts have been found to have better survival than lower-density grafts. Thus higher or lower density of fat grafts can be selected accordingly for different but more predictable outcomes after fat grafting. Appropriate centrifugation should be a valid method of choice for processing fat grafts, especially for small-volume fat grafting. 2 – 6

The Luer-Lok aperture of the 10 cc syringe is locked with a plug at completion of harvest, and the lipoaspirate is then ready for centrifugation. Each syringe is covered to prevent prolonged exposure to air and possible contamination. When the needed volume of fat has been harvested, the plunger is carefully removed, and all lipoaspirate-filled 10 cc syringes are placed into a centrifuge and centrifuged at 3000 rpm (1200 g) for 3 minutes. Greater g force or longer duration of centrifugation may be harmful to the adipocytes and is not recommended. 19
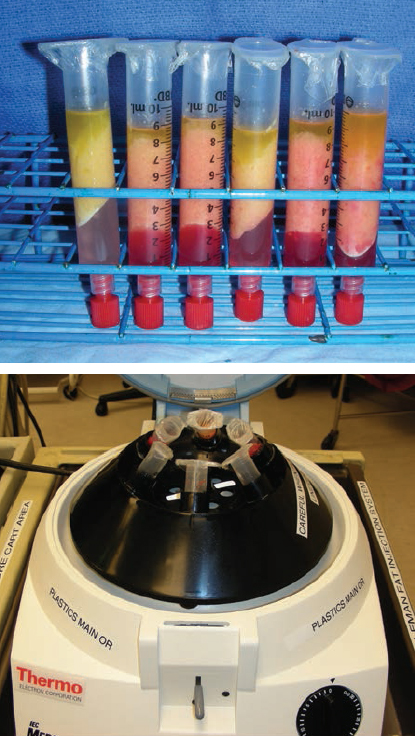
After being centrifuged, lipoaspirate within the syringe will have separated into three layers: the oil content in the upper layer, fatty tissue in the middle layer, and the fluid portion at the bottom. The oil can be decanted from the Luer-Lok syringe. The residual oil is wicked with a cotton strip or swab. The fluid at the bottom can be easily drained once the plug at the Luer-Lok aperture is removed. Through centrifugation, three distinct fractions are formed: oil, fat, and a liquid layer that includes tumescent fluid and debris.
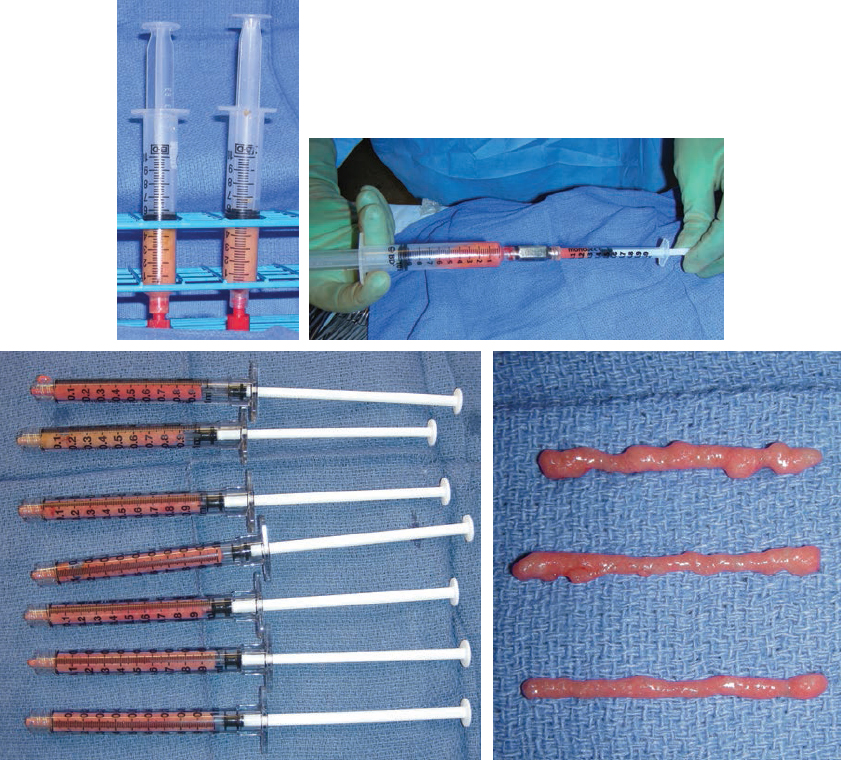
The concentrated fat in the syringe can then be transferred to a 1 cc syringe (our preferred size for fat injection) with an adapter. The 1 cc acrylic syringe is preferred for small-volume fat grafting; it creates little friction or resistance during injection, and thus the surgeon can easily control the injected volume. The air bubble inside the syringe should be removed so that quantification of the volume injected can be recorded precisely. We have also used a 3 cc syringe for large-volume fat grafting.
Processing Fat With a Device, Filtration, or Gravity Sedimentation
The manufacturers of several fat processing systems (such as the Revolve System, LifeCell, Branchburg, NJ; PureGraft, Cytori Therapeutics, San Diego, CA; or LipoKit, Medi-Khan, West Hollywood, CA) 9 – 11 have claimed that their devices produced equivalent or higher concentrations of purified fat with reduced red blood cell debris and free oil compared with alternative methods such as centrifugation. However, these studies in fact might have problems in their experiment designs and were not tested independently. In addition, they failed to prove their superiority in fat graft processing in terms of the concentration of viable adipocytes and in vivo fat graft retention rates.
Some surgeons advocate the use of a filtration technique or even just gravity sedimentation to process large or megavolume harvested fat grafts. However, without proper centrifugation, fat grafts processed with filtration only or sedimentation only may not be pure enough for transfer; they might contain potentially inflammatory materials such as free fatty acids and fragmented RBCs. Therefore proper centrifugation, even for large or megavolume fat grafting, may be considered an advisable technique.
One technique for large or megavolume fat graft processing has been described by Khouri et al. 12 Lipoaspirate is harvested with low (300 mm Hg) vacuum pressure using a 12-gauge cannula with 12 side-holes. The lipoaspirate is then collected into IV bags, and each bag is centrifuged at 15 g for 3 minutes, using a centrifugation machine or a hand-cranked centrifuge. Once the infranatant fluid is drained, the supernatant fat is concentrated in the same collection container, which becomes the graft delivery container. Compared with the pastelike, compacted graft obtained from 1200 g centrifugation, a dilute slurry of graft material is acquired from low g manual bag centrifugation. It is a preferred method by its advocates for large or megavolume fat grafting with the specifically designed device because of its speed and effectiveness.
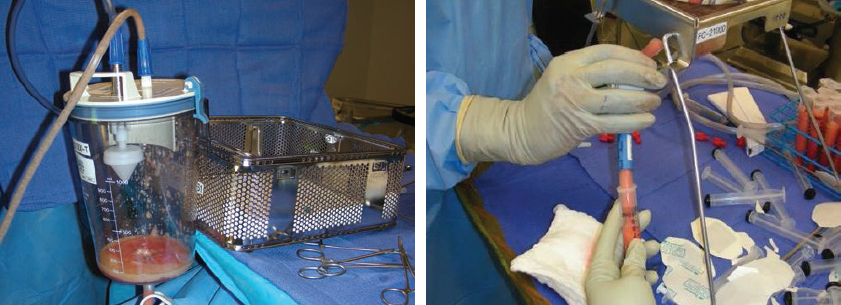
Alternatively, standard centrifugation can still be performed to process lipoaspirate harvested with low-pressure suction and a multiple side-hole cannula. 2 This is the method used in the senior author’s practice (L.L.Q.P.) for large-volume fat harvest and processing. In this system, a cannula with multiple side-holes (see Fig. 10-3) is used to harvest fat under low-suction pressure. Lipoaspirate is first collected into the canister and is then transferred into multiple 10 cc syringes for centrifugation.
Related posts:
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 5 ANTIINFLAMMATORY STEM CELL PRINCIPLES
Chapter 5 ANTIINFLAMMATORY STEM CELL PRINCIPLES
 Chapter 9 GROWTH FACTORS IN THE LIPOASPIRATE
Chapter 9 GROWTH FACTORS IN THE LIPOASPIRATE
 Chapter 8 DETERMINATION OF FAT VIABILITY
Chapter 8 DETERMINATION OF FAT VIABILITY
 Chapter 2 ANALYSIS OF THE PATIENT
Chapter 2 ANALYSIS OF THE PATIENT
 Chapter 1 THE COLEMAN TECHNIQUE
Chapter 1 THE COLEMAN TECHNIQUE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


