Chapter 1 The Midface
The Orbital Retaining Ligament, the Zygomaticocutaneous Ligaments, the Maxillary Retaining Ligaments, and the Masseteric Ligaments
The midface consists of both deep and superficial fat compartments along with two relevant anatomic spaces. The approach to the spaces and compartments has been previously published. The importance of hormonal receptors has been postulated but not investigated as a cause for midface descent, resulting in the aged appearance. Lambros postulated that midfacial aging was the result of volume loss rather than ligamentous or skin relaxation. Studies suggest a selective atrophy of deep fat compartments and relative hypertrophy of superficial fat, and this corresponds with larger adipocyte size in superficial fat compared to deep fat. The recent proposed concept of pseudoptosis or selective deflation of deep fat compartment leading to loss of support and sagging of the superficial cheek fat has led authors to advocate deep volumization techniques. We feel that the real decision lies in whether to inject in a sub-SMAS (subsuperficial muscular aponeurotic system) or supra-SMAS plane. This chapter will demonstrate the anatomy from deep to superficial portraying key anatomical targets for injection.
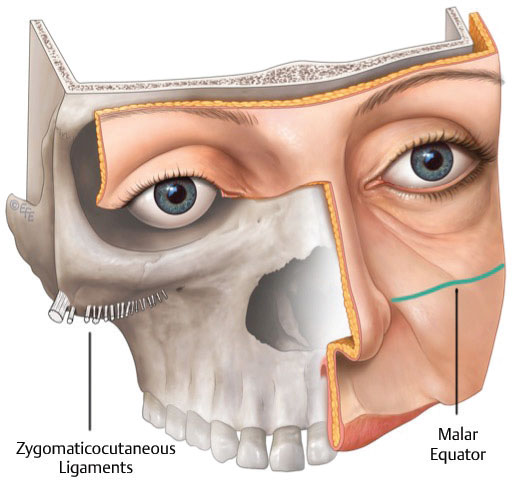
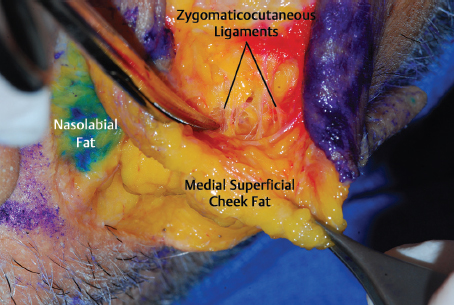
For the purpose of anatomical division, the midface can be divided into upper and lower regions by an imaginary topographic line traversing from the base of the alar crease to the superior tip of the tragus ( Fig. 1.1 ). This line corresponds with the course of the zygomaticocutaneous retaining ligaments that arise from bone and insert onto skin ( Fig. 1.2 ). This line acts as an equator between two distinctly different anatomical regions: the bone-supported cheek and the mobile cheek.
The Upper Midface
The orbital retaining ligament (ORL) is a bilaminar structure originating from the tear trough ligament. The ORL coalesces with the lateral orbital thickening as it traverses along the orbital aperture. The ORL separates the preseptal space from the prezygomatic space in the upper midface.
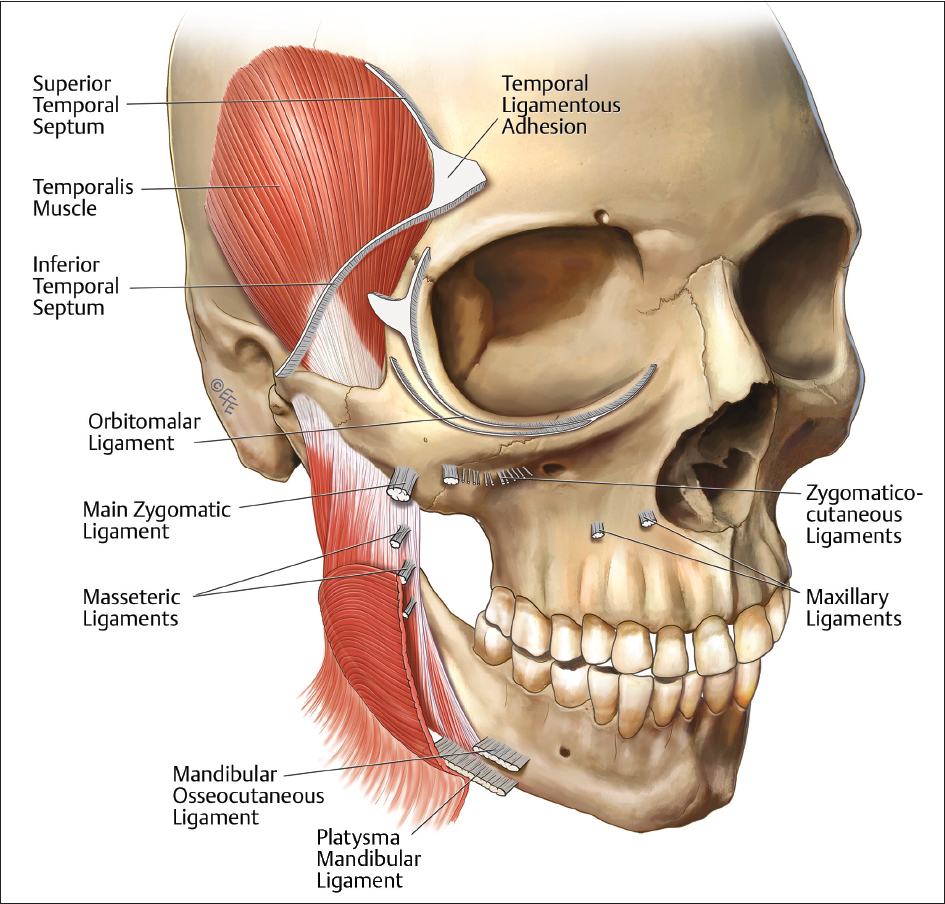
In addition to the zygomaticocutaneous ligaments, the main zygomatic ligament resides at the bony transition between the lateral and anterior midface at the maxillary deflection. As ligaments align with vascularized membranes, this region is clinically referred to as MacGregor′s patch.
The Lower Midface
On the surface of the anterior maxilla reside the maxillary retaining ligaments. The clinical relevance will be discussed later in this chapter in correlation with the premaxillary space. Laterally, the upper and lower masseteric ligaments divide the “fixed SMAS” laterally from the “mobile SMAS” anteriorly.
Fig. 1.3 presents the gross anatomy of the ligaments discussed in this section.
The Preperiosteal Fat Pad and the Deep Pyriform Space
The Upper Midface
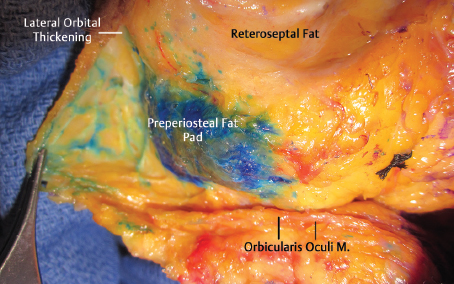
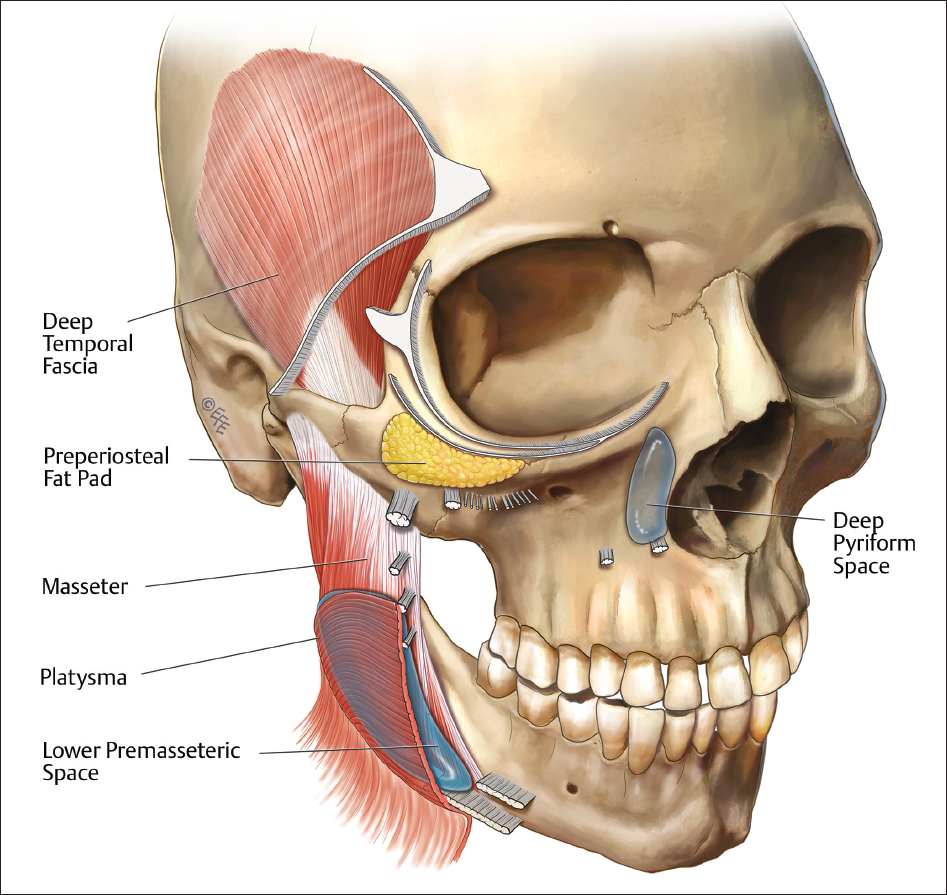
In the upper midface, deep to the orbicularis oculi, lie two layers of fat compartments: the preperiosteal fat compartment and the suborbicularis oculi fat compartment (SOOF), respectively. The SOOF will be discussed and demonstrated later in this chapter. However, deep to the SOOF and the prezygomatic space resides the preperiosteal fat compartment ( Fig. 1.4 ). This fat is adherent to the bone of the maxilla and in cadaveric dissection is often noted to be covered with a dense fascia.
The Lower Midface
Deep on the anterior maxilla lies the deep pyriform space ( Fig. 1.5 ). The deep pyriform space passes deep to the angular artery and abuts the recessing pyriform aperture ( Fig. 1.6 ). We postulate that, with age, the pyriform recesses, thereby enlarging the size of this space. In a cadaveric study, we found that the angular artery traverses lateral and superficial to the space and therefore is not preperiosteal at this level. This is an important finding for the injector as volumization in the deep pyriform space is not only effective in pyriform recess effacement, but also can be done safely without concern for intravascular compromise. Cannula pneumatization of the space demonstrates its deep connection to the upper midface through an undefined viaduct (Video 1.1). The lip elevators drape over this space as well, sending interlocking fibers into the nasolabial fold ( Fig. 1.7 ). Volumization of this space may decrease the moment arm effect of these muscles on nasolabial fold elevation and effacement. The cephalic limitation of both the deep pyriform space and the premaxillary space is the tear trough ligament.
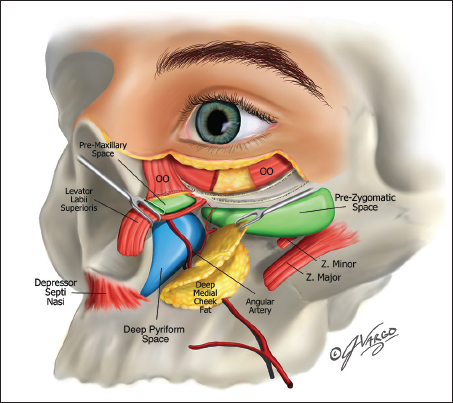
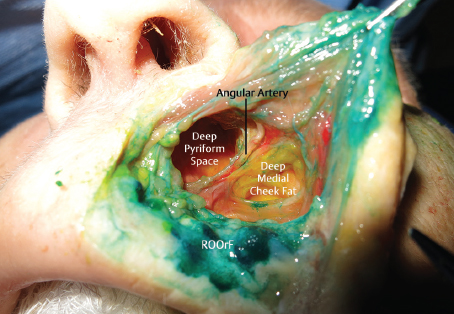
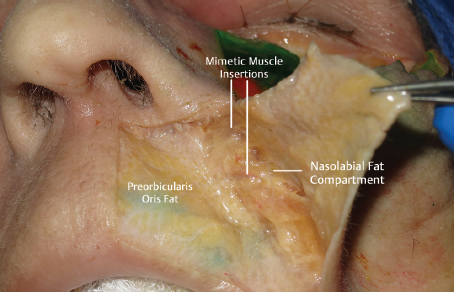
Fig. 1.8 presents the gross anatomy of the fat compartments and sub-SMAS spaces discussed in this section.
The Prezygomatic Space
The Upper Midface
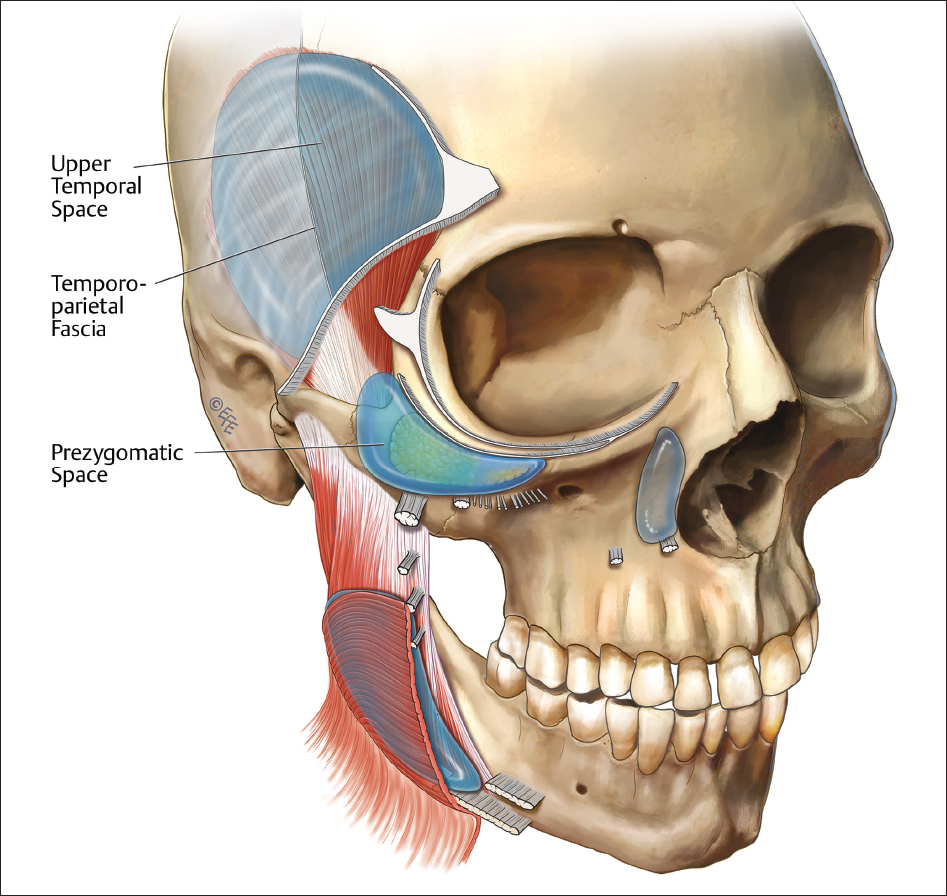
Deep to the orbicularis oculi muscle, between the SOOF and the preperiosteal fat pad, lies the prezygomatic space ( Fig. 1.9 ). The space is bounded superiorly by the ORL, which is synonymous with the orbitomalar ligament. The caudal extension of the space is limited by the zygomaticocutaneous ligaments. These ligaments act as a “hammock” network separating the upper midface from the lower midface. The lateral extent of the space is the lateral orbital thickening with a cephalic extension into the temporal tunnel.
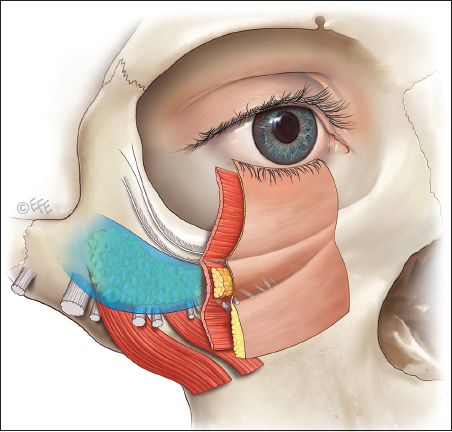
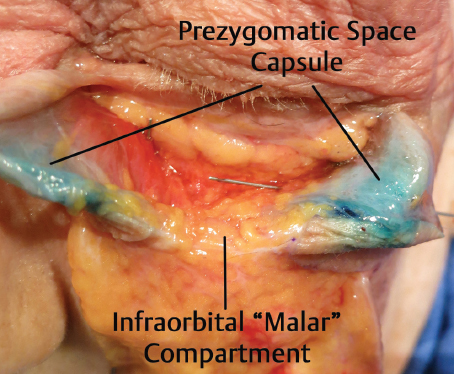
On the floor of this space lies the preperiosteal fat. The investing fascia of SMAS on the posterior border of the orbicularis oculi is contiguous with the fascia overlying the preperiosteal fat compartment. The uniform construct of these structures forms a prezygomatic space capsule as described by Mendelson ( Fig. 1.10 ). On blunt cannula access to this space from the lateral approach, the injector will use their opposite hand to “pinch and pull” the skin and orbicularis upward, allowing the cannula to pass deep and enter the prezygomatic space ( Fig. 1.11 ; Video 1.2). Entrance into the space is confirmed by a palpable and audible penetration of the prezygomatic space capsule. The injector will feel and hear a “pop” once when they pass through the capsule into the space.

Injection Pearl
For consistent deep volumization of the cheek, the prezygomatic space can be a secret weapon.
Fig. 1.12 depicts the gross anatomy of the prezygomatic space.
The Medial and Lateral Suborbicularis Oculi Fat Compartments and the Deep Medial Cheek Fat Compartment
The Upper Midface
The SOOF is a thin layer of fat residing between the undersurface of the orbicularis oculi muscle and the dense posterior capsule of SMAS. The SOOF is partitioned into medial and lateral components by an arterial branch supplying the palpebral eyelid.
The Lower Midface
The unique anatomical architecture of the lower midface exists caudal to the zygomaticocutaneous ligaments. The deep medial cheek fat (DMCF) compartment has been found to become deficient in volume with age and is associated with small adipocyte size, in contrast to the supra-SMAS fat compartments that have been shown to hypertrophy with age. Initially described by Pessa and Rohrich in cadaveric dissection, the three-dimensional construct of the DMCF was studied through computed tomography by Mathias Gierloff.
By definition, the deep medial cheek compartment lies anterior to the zygomaticomaxillary buttress. The DMCF is partitioned by the levator anguli oris creating medal and lateral components.
Related posts:
 Chapter 2 The Lymphatic Anatomy of the Lower Eyelid and the Malar Region of the Face
Chapter 2 The Lymphatic Anatomy of the Lower Eyelid and the Malar Region of the Face
 Chapter 3 The Perioral Area, the Chin, and the Jowl
Chapter 3 The Perioral Area, the Chin, and the Jowl
 Chapter 4 The Temple and the Brow
Chapter 4 The Temple and the Brow
 Chapter 5 SNIF: Sharp Needle Intradermal Fat Grafting
Chapter 5 SNIF: Sharp Needle Intradermal Fat Grafting
 Chapter 4 Perioral Rejuvenation
Chapter 4 Perioral Rejuvenation
 Chapter 8 Midface Volume Rejuvenation With Fillers
Chapter 8 Midface Volume Rejuvenation With Fillers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


