Chapter 3 The Perioral Area, the Chin, and the Jowl
The Aging Characteristics of the Lip and Perioral Region: Contemporary Concepts
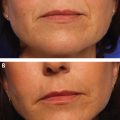
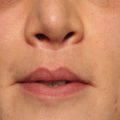
As far as we can tell, the perioral region is the one anatomical subunit of the face where muscle transformation plays a significant role in aging characteristics and appearance. Studies such as Iblher et al. and Penna et al. correlating radiographic change of soft and hard tissues to photometric changes offer the greatest insight into our understanding of the aging lip. Specifically, lengthening of the prolabium and loss of visible vermillion height are pathognomonic for an aging lip. Magnetic resonance imaging (MRI) scans demonstrate a decrease in anterior-posterior (A-P) dimension and increase in length without overall volume loss. Histomorphometric analysis demonstrates statistically significant thinning of the cutis, thickening of the subcutis, and a degeneration of elastic and collagen fibers.
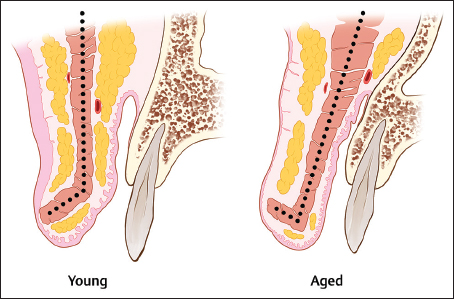
The orbicularis oris muscle, which is composed of a pars marginalis and a pars peripheralis, becomes thinner with age ( Fig. 3.1 ). As a result of pars marginalis descent, the muscle flattens and loses the forward curve (hockey stick) shape that is present in the youthful lip. This forward curve in the youthful lip is responsible for defining the vermillion border and consequently as the muscle changes with age the vermillion becomes less defined. In addition to soft-tissue changes, bony resorption of the anterior nasal spine and alveolus results in loss of anterior upper lip support, resulting in alterations to SNA measurements. Contrary to the upper lip, aging changes occurring in the lower lip are less quantified at present.
Deep Anatomy of the Chin and Jowl: The Mandibular Osseocutaneous Ligament and the Platysma Mandibular Ligament
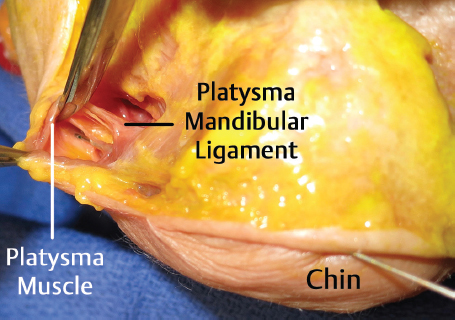
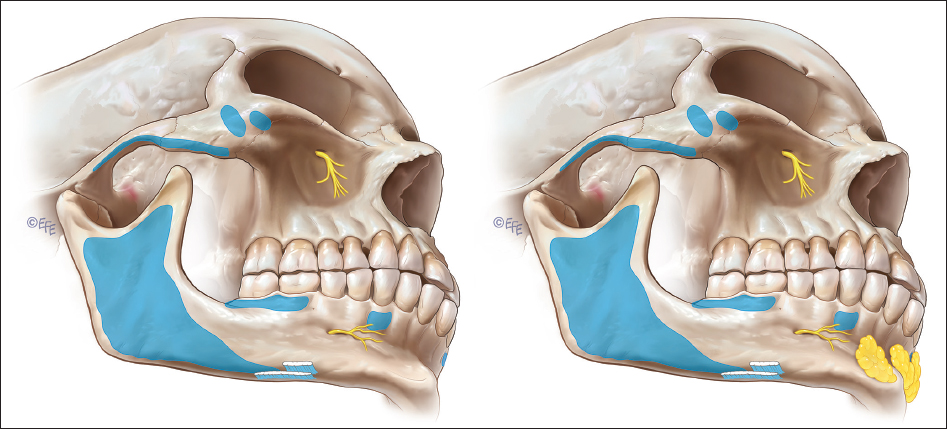
There are two key retaining ligaments in the jowl. The inferior and superior superficial jowl compartments are separated from the more caudal submandibular fat compartment by a defined osseomuscular septum titled the platysma mandibular ligament (PML) or mandibular septum ( Fig. 3.2 ). The PML is located approximately 5 cm distal to the gonial angle just above the mandibular border. It is postulated that this septum acts as “hammock” and physiologic laxity in its structural integrity leads to descent of jowl fat. The encasement of the PML with vascular channels likens it to a septum rather than a ligament. In addition, the PML is a point of muscular stability for the platysma as it glides over the mandible during coordinated movement, a function analogous to the orbital retaining ligament in the midface.
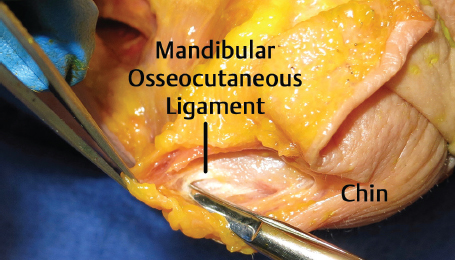
Cephalic to the PML lies the mandibular osseocutaneous ligament (MOCL; Fig. 3.3 ). MOCL sits approximately 5.6 cm from the gonial angle and 1 cm above the mandibular border. The ligament spans 3.6 mm in width and its distal fibers interdigitate with the depressor anguli oris (DAO), forming inferior quadrant of the marionette lines. The MOCL can be palpated clinically as the tethering point between the anterior jowl and marionette line. This gives credence to the well-documented benefit of releasing this ligament for skin mobilization in rhytidectomy. In reference to the location of the mandibular ligament, recent literature confirms the position of the ligament to be at the anterior margin of the jowl, near the parasymphyseal region. Of note, the PML and MOCL are not to be confused with the masseteric cutaneous ligaments, which are nonosseous ligaments attaching muscle to overlying skin.
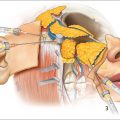
As the marginal mandibular nerve exits the parotid masseteric fascia, it travels sub-SMAS (subsuperficial muscular aponeurotic system) crossing the facial vessels 2.3 cm distal to the gonial angle. As the nerve crosses the vessels, it is 3 mm anterior to the vessel. The nerve does not transition superficially until it reaches the DAO. On average, the nerve will end as two branches with the dominant terminal branch ending 1 cm superior to the MOCL. Note that in accordance with traditional teaching, 81% of the time the nerve travels cranial to the mandibular border.
Injection Pearl
Injections caudal to the labiomental crease are SAFE.
Injection Pearl
Preperiosteal injections on the mandibular border are safe from a medial approach.
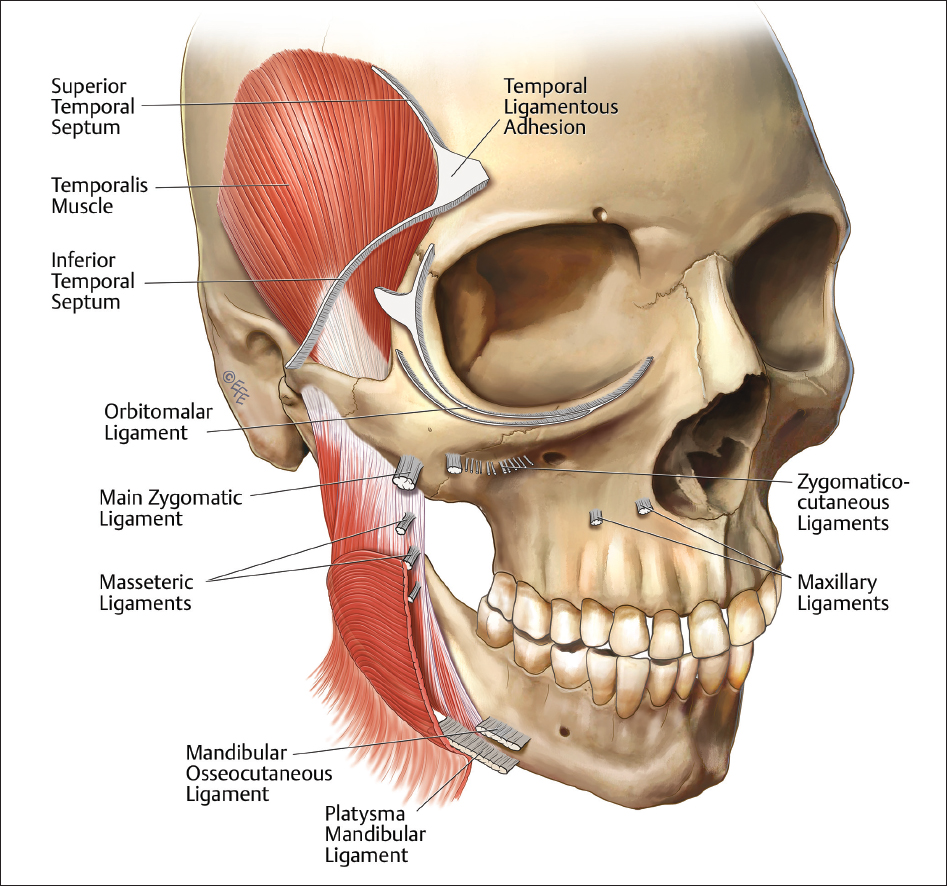
Fig. 3.4 shows the gross anatomy of the key retaining ligaments of the perioral region.
The Muscular and Compartment Anatomy of the Perioral Region
Muscular Anatomy
The three-dimensional (3D) muscular anatomy of the perioral region has been studied by Olzewski et al., but suffers from an n = 1 sample size. In fairness, the study is a report of methodology and not meant to represent a study of anatomic variability. However, this 3D MRI isotopic study in vivo demonstrates that the perioral musculature has a unique architecture.
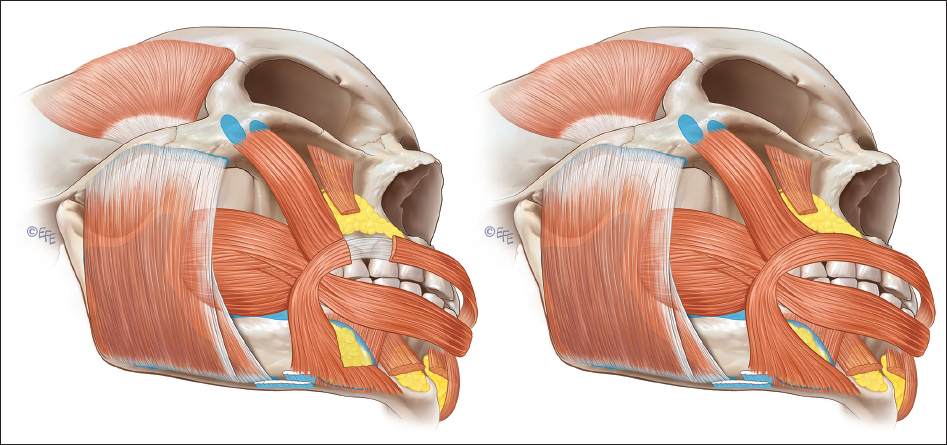
The orbicularis oris muscle is more circular at its lateral extent, than elliptical. The deep fibers of the orbicularis oris are a result of interlacing buccinator muscle fibers, whereas the superficial fibers of the orbicularis oris arise from a coalescence with the lip elevators and lip depressors. The levator anguli oris (LAO) inserts behind the buccinators. The levator labii superioris (LLS) lies immediately alongside the LAO. The zygomaticus major muscle abuts the lateral edge of a vertical component of the orbicularis oris muscle. Of note, a lamina propria exists within the lip sphincter located between the orbicularis muscle and mucosa.
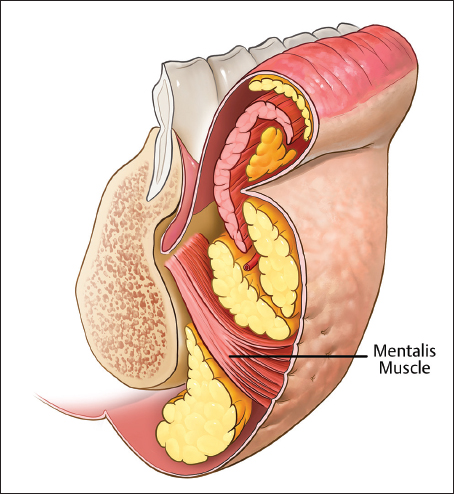
The lower perioral region contains three key muscles. The depressor labii inferioris (DLI), DAO, and mentalis muscle ( Fig. 3.5 ). The DLI muscle originates on the mandible between the symphysis and mental forearm and inserts on the orbicularis muscle and skin. The DAO originates on the mandibular tubercle where it is fused with the platysma and inserts onto the modiolus and the angle of the mouth. Literature regarding mentalis muscle is sparse. The mentalis muscle originates on the upper symphysis and mental fat compartments, the fibers traverse cephalic fanning outward and interdigitating with orbicularis oris and skin of the lower lip. The mentalis muscle has a V-shaped configuration. Added to the DLI, it forms an “M”-shaped configuration in the lower lip. Mentalis strain is largely the result of poor bony support within individuals with Angle′s Class II occlusion or in individuals with atrophy of the mental fat
Deep Lateral Chin Compartment
In the lower lip and prejowl lies the deep lateral chin compartment ( Fig. 3.6 ). This compartment is a key augmentation target for volumization of the prejowl sulcus. This fat pad lies deep to the DAO to facilitate muscle gliding with movement. This subDAO fat has a thin gliding membrane along its anterior surface and protects the mental nerve that has a superomedial course and often accompanies the inferior labial artery. The diameter of the inferior labial artery makes small needle injection in the sub-DAO region a moderately risky proposition. Accessing this fat compartment via a cannula placed in the small triangle bounded by the lateral border of the DLI, the medial border of the DAO, and the caudal border of the orbicularis oris with an inferolateral angulation can be an effective volumization technique ( Fig. 3.7 ). Alternatively, the caudal half of this compartment may be accessed via a paramedian chin pad approach, passing caudal to the mental nerve foramen over periosteum of the mandible, traversing in a medial to lateral direction.
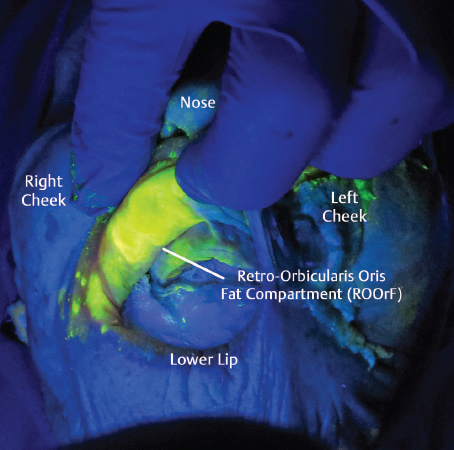
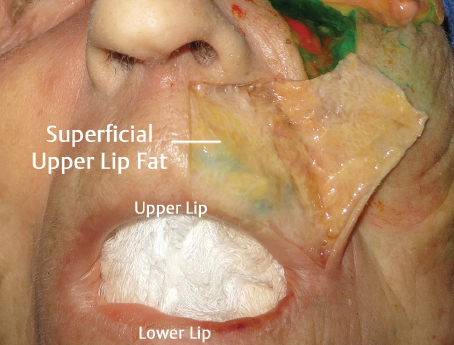
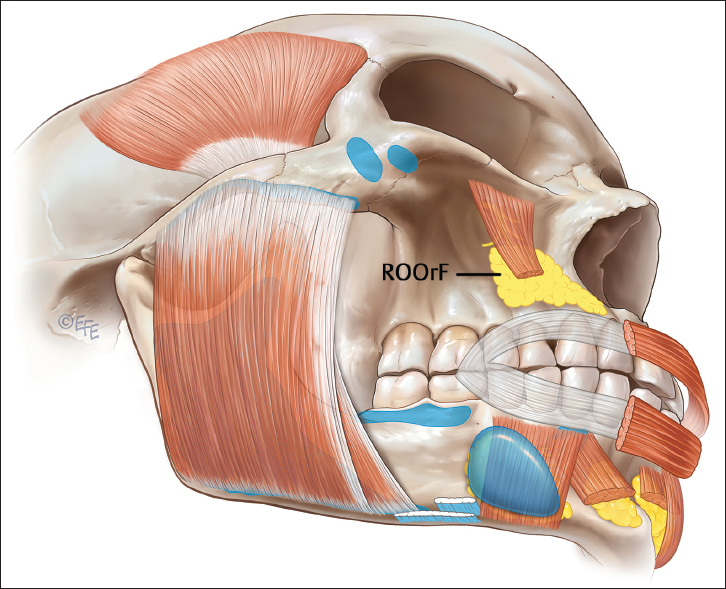
Retro-orbicularis Oris Fat
Within the upper lip, a fibrofatty compartment exists deep to the orbicularis oris muscle, which appears to lose turgor with age. This retro-orbicularis oris fat (ROOrF) compartment has been briefly referenced by other authors who have studied perioral anatomy ( Fig. 3.8 ). The caudal extent of the compartment is roughly the midpoint of the upper central dentition. The cephalad extent stops short of the labial buccal recess. Injection studies of the space freely flow superolateral to the orbicularis oris upper margin and progress from deep to superficial with the skin of the alar base and nasolabial fold. Clinically, we find this compartment to be a useful augmentation target in patients with upper alveolar collapse from previous bicuspid extraction, as well as pyriform aperture retrusion. The consistency of the fat is different than that of its cephalic counterparts. In cadaveric dissection, the fat is unfused with the overlying muscle and soft tissues and displays a sharp transition from its bordering structures outside the perioral aperture.
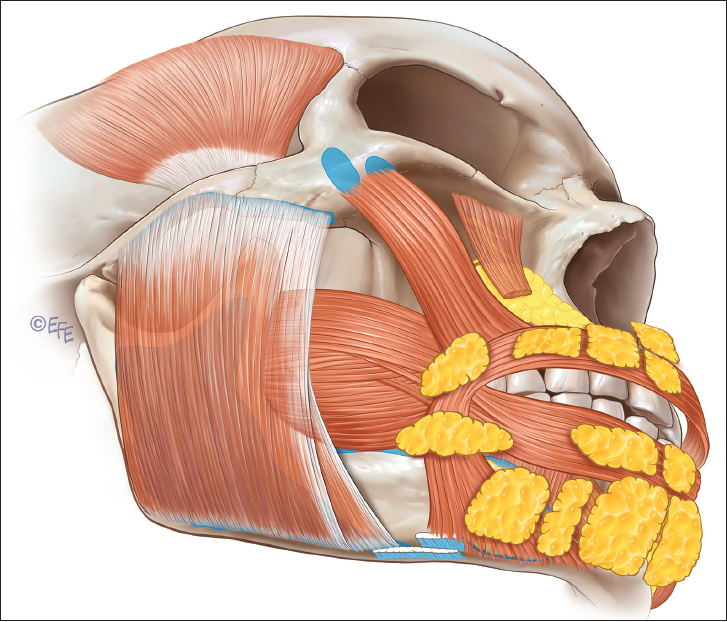
Superficial Lip Compartments
According to Pessa et al, the upper lip contains a series of superficial fat compartments ( Fig. 3.9 ). These compartments are separated by vascularized septa containing arteries smaller than the outside diameter of 30-gauge needles, with the exception of the arteries coursing near or just slightly lateral to the philtral columns: the superior upper lip compartment, lateral upper lip compartment, inferior lateral upper lip compartment, and the central upper lip compartment. The central upper lip compartment contains an inferior and a superior quadrant. Clinically, these subcutaneous compartments are thin and compartmental division corresponds with vascular septation similar to other regions of the face. These septations are manifested as vertical perioral rhytids.
According to Pessa et al, the lower lip contains a trio of superficial fat compartments: the central lower lip fat compartment, lateral lip compartment, and the inferior chin compartment. The medial boundary of the lateral lip compartment is the septum containing the inferior labial artery. The arteries cephalic to the inferior labial–buccal sulcus are of the very small size, making intra-arterial cannulation by injection in these areas unlikely, and therefore render these compartments as potential targets for volumization.
Perioral Potential Spaces
Within the lower lip, a potential space exists over the ill-defined white roll. Arterial vasculature immediately deep to this space is intimate with the SMAS of the lower lip orbicularis oris. Cannula passage from commissure directed medially can easily traverse the entire lower lip. Cannula passage from a paramedian port, directed laterally, in this space finds a hard membranous barrier at the commissure and extending caudally a short distance.
Potential spaces also exist within the subvermillion of both the upper and lower lips. The upper lip has a potential space that is frequently medially partitioned posterior to the wet dry junction and a second space that is rarely partitioned anterior to the wet dry junction. The lower lip has a subvermillion space that is present both anterior and posterior to the wet–dry junction. The anterior space extends across the entire width of the lip and the posterior space ends at a midline partition.
The gross anatomy of the ROOrF is shown in Fig. 3.10 , and Fig. 3.11 depicts the superficial fat compartments of the perioral region.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


