Case 43 Major Liposuction
43.1 Description
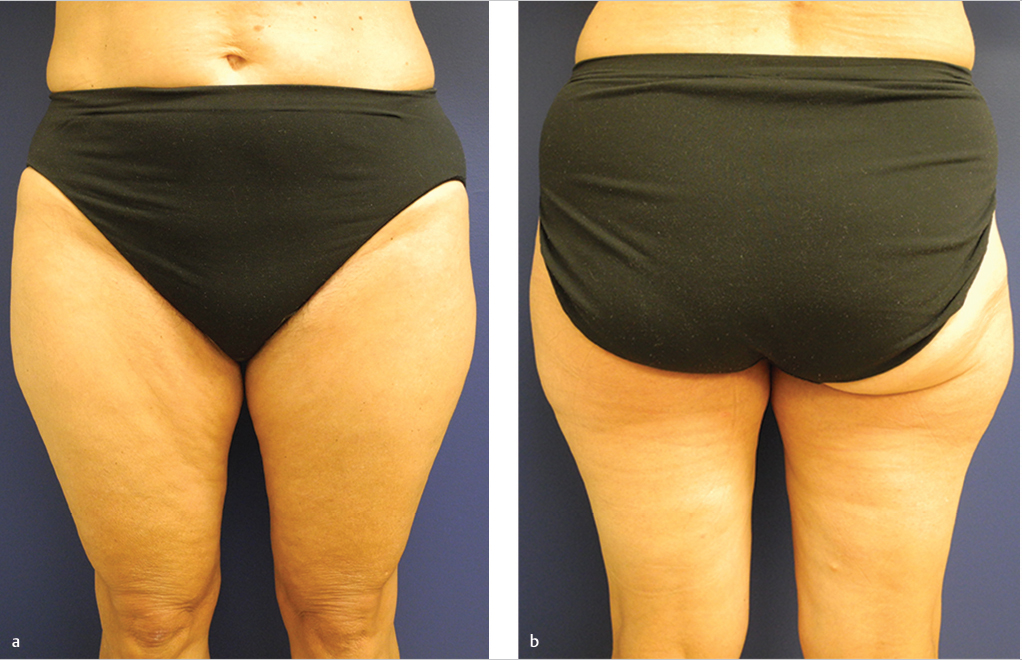
Significant, diffuse lipodystrophy noted bilaterally in saddlebag regions of upper lateral thighs
43.2 Work-Up
43.2.1 History
Weight stability
Medical comorbidities
Patient’s concerns and goals of treatment
43.2.2 Physical Examination
Identify regions of suboptimal contour, asymmetry, and lipodystrophy
Evaluate skin quality and tone (thickness and elasticity): Pinch test
Abdomen: Examine for hernias and diastasis
43.3 Patient Counseling
Discuss risk/benefit profiles of each procedure
Ensure the goals of the patient align with the goals of the procedure
Liposuction is a contouring procedure
Best in areas of thick, elastic skin with underlying contour fat irregularity
Does not address cellulite or obesity: Cellulite thought to be due to hypertrophy of superficial fat within septa and/or increased skin laxity
Does not resect skin
Set expectations in regards to pain and swelling during the postoperative period
43.4 Treatment
Make preoperative markings with patient upright: To determine treatment areas and asymmetries, and outline zones of adherence
Distal iliotibial tract
Gluteal crease
Lateral gluteal depression
Middle medial thigh
Distal posterior thigh
Preoperative considerations
Complete blood count (CBC) if expecting to perform large volume procedure
Deep vein thrombosis (DVT) prophylaxis (see Chapter 42)
Hypothermia and necessary precautions
Positioning
Target deep fat layer and cross tunnel to prevent contour irregularities
Wetting solution technique (see Table 43-1)
Four types of liposuction techniques described based on the volume of infiltration or wetting solution injected: Dry, wet, superwet, and tumescent techniques
Lidocaine, epinephrine, and bicarbonate solution added to saline or Ringer’s Lactate
Provides anesthesia and hemostasis
Maximum lidocaine with epinephrine: 35 mg/kg
Liposuction modality
Suction-assisted liposuction (SAL): Traditional liposuction technique
Power-assisted liposuction (PAL): Motorized oscillating hand piece
Ultrasound-assisted liposuction (UAL): Ultrasonic energy applied after wetting solution to emulsify fat before aspiration
Ideal for fibrous regions: Buttock, lumbar, and gynecomastia
Precautions to avoid cutaneous thermal injury
Laser-assisted liposuction (LAL)
Possible skin tightening effect due to heating of subdermal tissue
Fluid management for large-volume liposuction (Critical safety issue)
Replace preoperative deficits
Employ superwet or tumescent technique
Administer maintenance fluids + replacement of 0.25mL per 1mL of aspirate over 5L
Titrate intravenous fluid (IVF) to patient’s clinical picture (e.g., urine output, vital signs)
Maintain intraoperative fluid ratio: [(IVF + infiltrate)/aspirate] ≈ 1.2
Older technique (Pitman): (IVF + infiltrate) = 2 x (aspirate)
With aspirate, 25 to 30% of infiltrate is removed
If large-volume liposuction (≥4–5L) is performed, it must be done in acute-care hospital or accredited facility
Monitor vitals and fluid balance with Foley catheter; overnight inpatient observation
Warm patient, fluids, and operating room (OR) to avoid hypothermia
Dilute lidocaine further if greater volume of infiltration is necessary
DVT prophylaxis (see Table 42.2 for risk stratification)
Mechanical: Sequential compression devices
Ambulate on postoperative day 0 (day of surgery)
Chemoprophylaxis not routinely required, but should be considered
Postoperative care
Early ambulation
Compression garments 4 to 6 times in a week
Table 43.1 Wetting solutions for liposuction
Technique
Infiltrate
EBL (% volume)
Dry
None
20–45
Wet
200–300 mL/area
4–30
Superwet
1 mL infiltrate: 1 mL aspirate
1
Tumescent
2–3 mL infiltrate: 1 mL aspirate
(or to skin turgor)
1
Abbreviation: EBL, estimated blood loss.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


